
Abstract
Introduction
A better understanding of the nature of morbidity and mortality in avalanche accidents helps direct both rescue efforts as well as preventive strategies to reduce fatalities.
Methods
We reviewed all avalanche fatalities from the avalanche years beginning in 1994 to 2015 in the state of Colorado, United States, using the database maintained by the Colorado Avalanche Information Center. For each fatality, we obtained the coroner’s official determination of cause of death, and autopsy records if one was performed. We used these records to determine cause of death. Injury severity scores (0–75 scale) were calculated for those victims who underwent autopsy.
Results
Mortality information was available for 110 fatalities occurring during the 21-year study period. Of these, 64 underwent autopsy. Asphyxia was the cause of death in 65% of fatalities (72/110). Trauma was the cause of death in 29% of the fatalities (32/110). Of these, the primary cause was multiple system trauma in 38% (12/32), head trauma in 31% (10/32), and spinal injuries in 19% (6/32). Of the victims who died of asphyxia and had autopsy, only 10% (4/42) also had significant trauma, defined as an injury severity score greater than 15. There were 6 fatalities from other causes, including hypothermia, drowning, and primary cardiac arrest. There was no correlation between trauma and mode of travel, avalanche type, or starting zone elevation.
Conclusions
Asphyxia was the primary cause of death in avalanche fatalities in Colorado during our study period. The incidence of fatal trauma was 29% and did not correlate with user group demographics or avalanche characteristics.
Introduction
Snow avalanches and the fatalities they cause have plagued mountain communities the world over. In the United States, the state of Colorado has historically led the country in human deaths from avalanches (Figure 1). Although mining contributed to the majority of fatalities before World War II, recreationalists have been the victims in the majority of cases since 1950. 1 Over the past 21 years, from 1994 to 2015, avalanches have been the cause of 124 deaths in the state of Colorado, with nearly all of them (117/124) associated in some way with recreational activities. Of the 7 nonrecreational deaths, 4 were residents and 3 were working ski patrollers. Current avalanche safety education and prevention strategies emphasize avoidance; nonetheless, avalanche accidents continue to occur. As asphyxia has been identified as the leading cause of death if caught in an avalanche, 2 techniques and equipment to improve survival focus on reducing time under the snow. These include using safety devices such as airbags designed to reduce complete burial, transceivers to locate a buried subject quickly, and shoveling techniques to dig them out rapidly. Other causes of fatalities in avalanche accidents have not been as well addressed, with many cases unrelated to asphyxia. Previous studies have found rates of fatal traumatic injury as high as 24% in Canada 3 and as low as 5.6% in Europe. 4 A better understanding of the nature of morbidity and mortality in avalanche accidents will enhance prevention, as well as response when accidents occur.
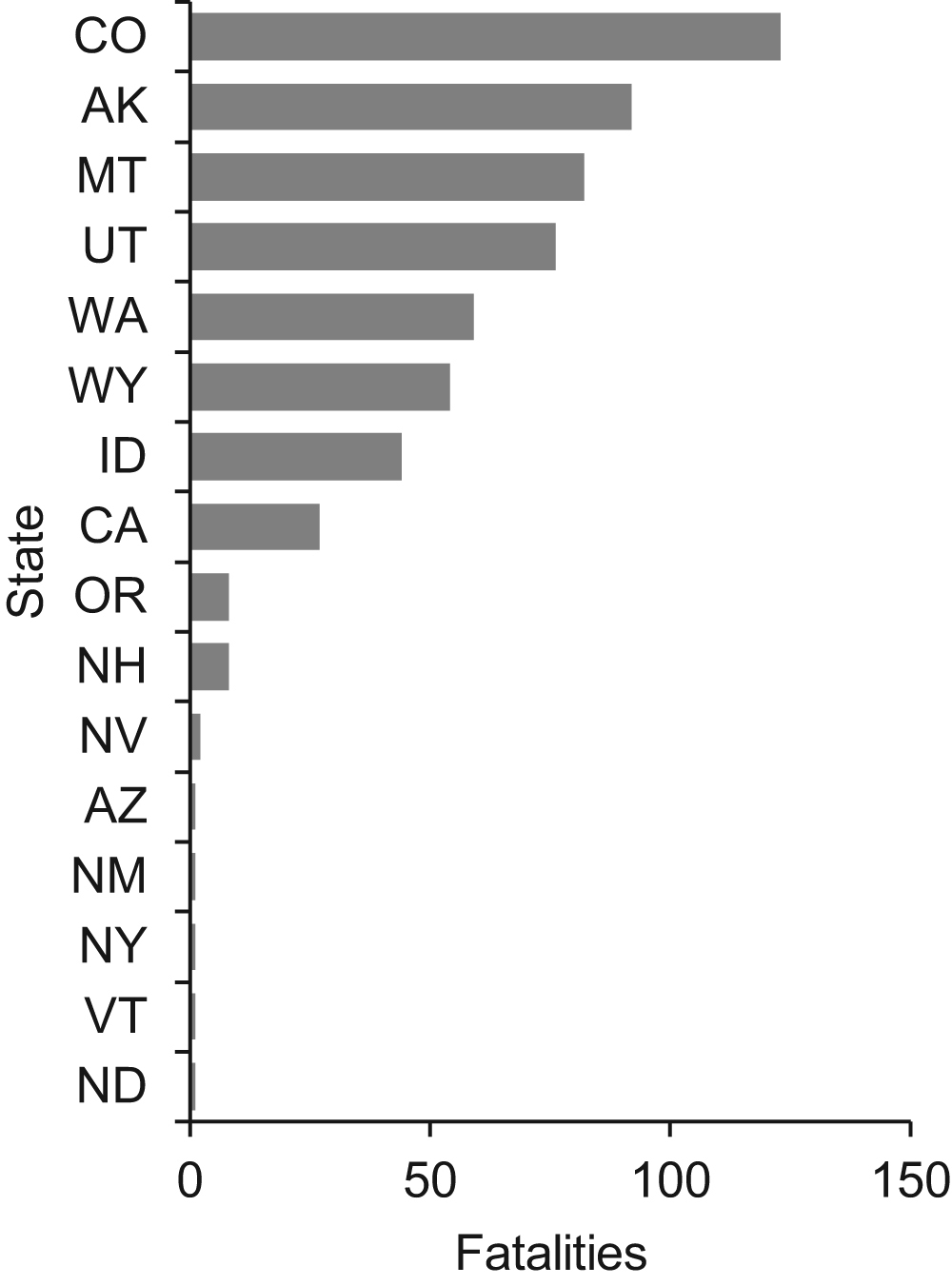
Avalanche fatalities by state, 1994 to 2015.
Our primary goal was to determine the cause of death in avalanche fatalities in Colorado during the study period and to examine the frequency and severity of traumatic injuries. A secondary goal was to investigate whether the incidence of fatal trauma in avalanches correlated with avalanche characteristics or user groups.
Methods
Population
We reviewed all snow avalanche deaths in the Colorado Avalanche Information Center database for the avalanche years 1994 to 2015. 5 We excluded incidents in which avalanche was not a primary contributor to the fatality. We also excluded the 3 avalanche fatalities that resulted from slides off a roof or building, as they did not occur in a wilderness or mountain environment.
Data Collection and Abstraction
Avalanche data was abstracted from Colorado Avalanche Information Center records by a single investigator (SL) who was blinded to the cause of death. Fields included elevation, date, group size, demographic information about victims, mode of travel, and avalanche characteristics.
We contacted individual county coroners to obtain records including the official cause of death and, if performed, the autopsy report. In total, we requested records for 124 fatalities from 26 separate county coroners in the state of Colorado.
A single investigator (AS) abstracted mortality data. For all cases, the investigator assigned cause of death based on the coroner’s official determination of the principal cause of death. Other data abstracted included organ systems involved and type of injury sustained, if any. If an autopsy was performed, the investigator calculated an injury severity score (ISS).
The ISS 6 is an anatomical scoring system for injured patients based on the abbreviated injury scale. An abbreviated injury scale is assigned to each of 6 body regions, and the 3 highest scoring regions are individually squared and then added together to produce the ISS score. The values range from 0 to 75, with severe trauma being defined as a score greater than 15.
Statistical Analysis
We examined the incidence of traumatic fatalities for correlation with avalanche characteristics and some demographic data of the victims. We used χ2 tests to assess possible correlation of trauma with avalanche type or with victim’s primary travel mode. We used Mann-Whitney U tests to assess possible correlation of trauma with avalanche starting zone elevation or with victim age. 7
Results
We identified 121 eligible avalanche fatalities during the specified 21-year study period. Through the study period, the number of avalanche fatalities by calendar year ranged from 3 to 11, with a mean of 6.1 and standard deviation of 2.1. All fatalities occurred in the months of October through May. Mortality data was available for 110 of these; 64 had complete forensic autopsies performed.
The primary cause of death was determined to be asphyxia in 65% (72/110) of cases. Trauma was determined to have been the cause of death in 29% (32/110) of the fatalities. Of these traumatic fatalities, the primary cause was multiple system trauma in 38% (12/32), head trauma in 31% (10/32), and spinal injuries in 19% (6/32) of victims. There were 6 fatalities from other causes, including hypothermia, drowning, and primary cardiac arrest (Table 1).
Primary cause of avalanche fatalities
We calculated ISS scores for all 64 victims who had forensic autopsies performed. Injury types for scores below 10 are generally only superficial abrasions and lacerations or isolated closed extremity fractures. Scores of 15 to 30 can be more complex fractures and internal injuries that may or may not be immediately life threatening. Greater than 30 are injuries likely to cause death rapidly; for example, in our study this included severe craniofacial injuries, vascular injuries of the aorta or other major vessels, and multisystem trauma. Multiple injuries in the same body region may score lower as only the most severe injury for anatomical region is used to calculate the ISS score.
Of the 64 autopsies reviewed, 17 (26%) were determined to have trauma as the primary cause of death, and 42 (65%) as asphyxia. The ISS calculated on the 17 trauma fatalities indicated severe injuries for all victims, and ranged from 16 to 75 with a median of 35, mean of 38, and standard deviation of 20. In the subjects whose cause of death was nontraumatic, 30 had ISS of 0 or 1, and only 4 had ISS greater than 15 (Figure 2). The incidence of severe trauma in asphyxia victims was 4/42 (10%) of those who underwent autopsy.
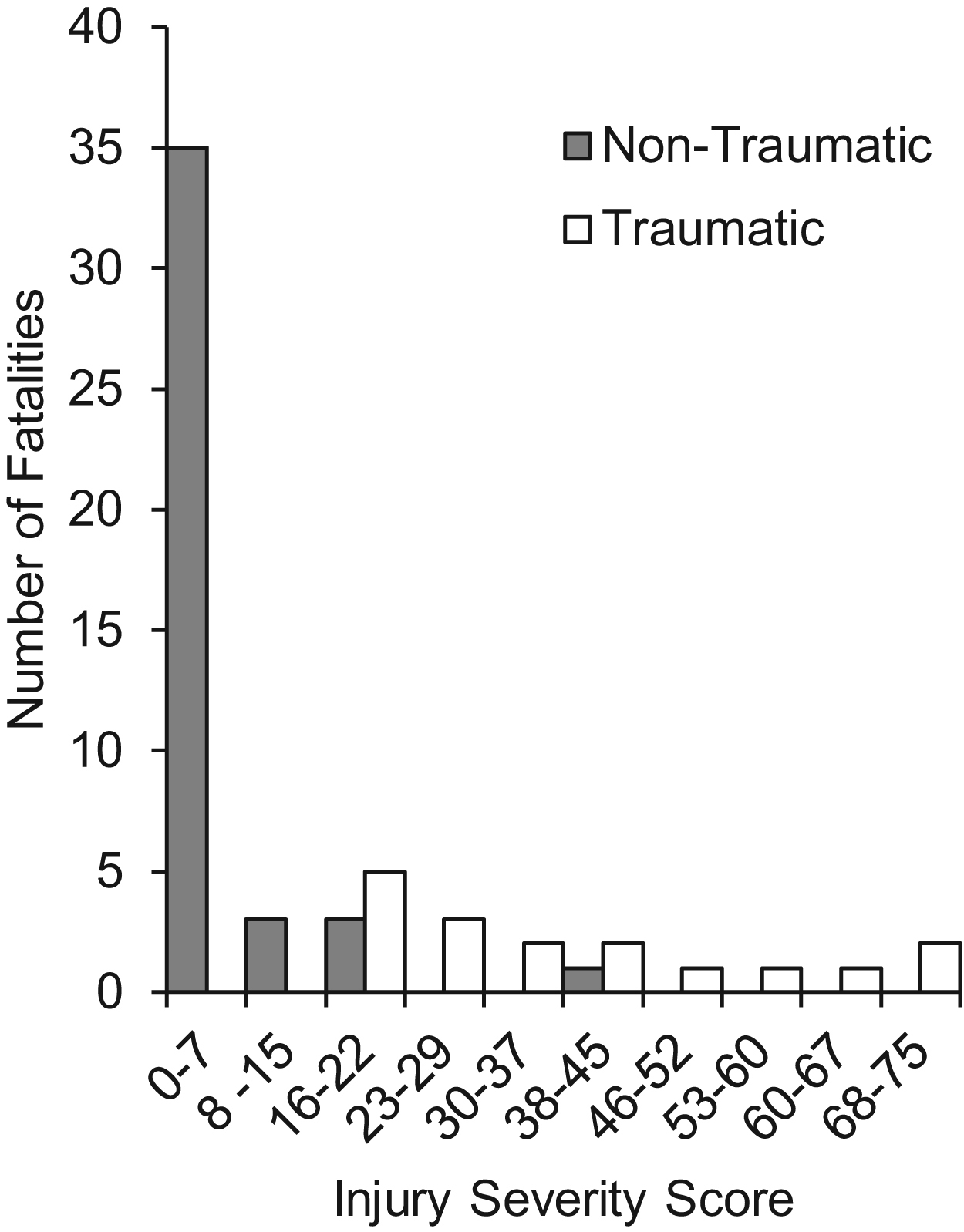
Comparison of ISS in nontraumatic and traumatic fatalities.
Incidence of trauma did not vary widely with respect to mode of travel (Table 2) or avalanche type (Table 3). The percentage of trauma did not differ with the victim’s primary activity (χ2 [7%, n=107] = 4.25; P=0.75) or age (U=1145; P=0.50). Likewise, the percentage of trauma did not differ with the avalanche type (χ2 [3%, n=107]=3.24; P=0.36) or starting zone elevation (t [104]=1.98; P=0.37).
Number of fatalities by primary activity and percent of traumatic fatalities
Number of fatalities by avalanche type and percent of traumatic fatalities
Discussion
Asphyxia was responsible for the majority of deaths in our study. This is consistent across similar previously published studies. 2 –4 Reducing the occurrence and duration of critical burial, where the victim’s head is under the surface of the snow and breathing is impaired, has the potential to result in the largest reduction in fatalities. 8 This is especially true in light of the low (10%) incidence of major traumatic injuries in asphyxia victims who had autopsy performed. If these victims had avoided critical burial or been uncovered rapidly, it is possible that some would have had a good chance of survival.
Nearly one third of victims in our study died of traumatic injuries. The incidence of trauma as the cause of avalanche deaths in Colorado is markedly higher than previous studies found in Europe and Utah 4 ,9,10 and slightly higher than reported in Canada. 3 It is lower than the incidence of trauma that has been reported in summer accidents in Switzerland. 11 Researchers have attributed these differences to factors such as geography, topography, season, and activity. 3 ,10,11 In the United States, researchers found trauma to be relatively common as avalanches swept many victims through or into trees, cliffs, rocks, and gullies. 12 However, in the Colorado data, no significant differences were found based on the elevation of the avalanche starting zones. Using 3500 m as an approximation of the tree line elevation, 13 there was no increase in trauma at lower elevations. Avalanches in forested terrain do not appear to increase the potential for traumatic fatalities. The lower rates of trauma in the European studies may reflect the different research methods and lack of autopsy data more than terrain or activity.
A 2013 revision to international avalanche resuscitation guidelines gave more importance to trauma care. 8 More attention to trauma management in the on-site care of avalanche victims has been recommended, 14 and the high rate of trauma found in our series supports that suggestion. It is notable that most safety equipment currently in use focuses on mitigating the potential for asphyxia as a consequence of critical burials. In our series, the use of preventive equipment such as air bag packs, AvaLungs (Black Diamond Equipment, Salt Lake City, UT), and transceivers may not have prevented these traumatic fatalities. Given the high rate of trauma found in our avalanche victims it is important that travelers in avalanche terrain have appropriate first aid training. Likewise, rescuers should also be prepared to manage serious traumatic injuries.
Head injury was the primary injury in nearly one-third of the traumatic fatalities in Colorado. This rate is notably less than the 42% reported in Canada 3 but greater that the 21% reported in a series of avalanche deaths in Utah. 15 Collectively, the experience in western North America contrasts sharply with an Austrian study 4 that found no lethal head injuries in a review of avalanche fatalities. Although helmets have been recommended 3 ,10,15 for those in avalanche terrain it is not definitively known whether use of currently available helmets offers significant protection in the event one is caught in an avalanche.
In comparing avalanche type, mode of travel, age of victim, and elevation we did not find statistically significant differences in the proportion of traumatic fatalities. This suggests that all backcountry travelers, regardless of demographics, are at risk for fatal trauma if caught in an avalanche. This would suggest that we need further research into the effectiveness of equipment and other mitigation strategies intended to prevent injuries.
Over the decades, a number of other studies have looked at the cause of death in avalanches; however, limitations in study design, small sample sizes, incomplete information, and unusual conditions limited the meaningful conclusions.16,17 Previous authors of avalanche fatality research have highlighted the importance of autopsy, or at least full external forensic examination as the minimum from which to draw postmortem conclusions. 17
Limitations
We were able to obtain documentation of the coroner’s determination of official cause of death for 110 of 121 (91%) of eligible avalanche incidents. It is possible although not likely that information in the missing 11 records would substantially alter our results or our conclusions.
Although 64 of 121 (60%) of the subjects in our study had definitive forensic autopsies performed, the remainder had cause of death attributed by external examination only. It is possible that this could result in misclassification in some cases. For example, fatal internal traumatic hemorrhage may have only minimal external physical findings. In this situation, asphyxia may be mistakenly assumed to be the cause of death.
We were unable to draw any conclusions about traumatic injuries sustained in avalanches in general, if the incident did not result in a fatality. These nonfatal cases were not part of this investigation, and involved parties rarely document them unless a formal rescue is required. 18
Conclusions
Based on autopsies and external forensic examinations asphyxia was the primary cause of death for most avalanche victims. However, lethal trauma killed nearly one-third of victims, which is a notably higher rate than reported in Europe, but similar to the rate previously reported in Canada. The incidence of fatal trauma did not correlate with the victim’s activity or mode of travel, the avalanche type, or the starting zone elevation.
Although prevention is the best action to ensure survival in avalanche terrain, rapid rescue and prompt and appropriate resuscitation will result in the best opportunity to save additional lives. These data also suggest that further consideration should be given to strategies that would decrease the likelihood of trauma if one is caught in an avalanche, and equipment such as helmets, which could possibly mitigate the severity of injury.
Acknowledgments: We acknowledge Josh Rubinsky RN, trauma coordinator at Boulder Community Health, Boulder, CO, for his assistance with ISS scoring. Many thanks to the avalanche professionals around Colorado who document avalanche accidents.
Author Contributions: Conception and design of the study (AS, DW, SL, DA); data acquisition, analysis and interpretation of data (AS, DW, SL, DA); drafting and revising the article (AS, DW, SL, DA); final approval of the submitted version (AS, DW, SL, DA).
Financial/Material Support: None
Disclosures: None