
Abstract
Introduction
We compared the effectiveness of 5 heated hypothermia wrap systems.
Methods
Physiologic and subjective responses were determined in 5 normothermic subjects (1 female) for 5 heated hypothermia wraps (with vapor barrier and chemical heat sources) during 60 min of exposure to a temperature of −22°C. The 5 systems were 1) user-assembled; 2) Doctor Down Rescue Wrap; 3) hypothermia prevention and management kit (HPMK); 4) MARSARS Hypothermia Stabilizer Bag; and 5) Wiggy's Victims Casualty Hypothermia Bag. Core and skin temperature, metabolic heat production, skin heat loss, and body net heat gain were determined. Subjective responses were also evaluated for whole body cold discomfort, overall shivering rating, overall temperature rating, and preferential ranking.
Results
The Doctor Down and user-assembled systems were generally more effective, with higher skin temperatures and lower metabolic heat production; they allowed less heat loss, resulting in higher net heat gain (P<0.05). HPMK had the lowest skin temperature and highest shivering heat production and scored worse than the other 4 systems for the “whole body cold discomfort” and “overall temperature” ratings (P<0.05).
Conclusions
The user-assembled and Doctor Down systems were most effective, and subjects were coldest with the HPMK system. However, it is likely that any of the tested systems would be viable options for wilderness responders, and the choice would depend on considerations of cost; volume, as it relates to available space; and weight, as it relates to ability to carry or transport the system to the patient.
Introduction
Patients exposed to a cold environment for an extended period present a challenge for rescue, medical care, and transport under austere conditions. In addition, trauma increases the complexity of caring for the cold patient. Not only are trauma patients at greater risk of developing hypothermia, but cold increases the mortality and morbidity of traumatic injuries.1,2 Therefore, effective management of the prolonged, cold-exposed patient (whether normothermic or hypothermic) requires prevention of continued heat loss and, if possible, external warming to prevent development or worsening of hypothermia and frostbite. 1 –4 These goals can be addressed by providing a portable heat source within an enclosure system commonly referred to as a “hypothermia wrap.”
Several studies have evaluated different insulators, such as blankets, rescue bags, bubble wraps, space blankets, plastic covers, quilts, mountain casualty bags, and military survival bags. 5 –9 Studies have also compared different active warming sources such as chemical and charcoal heat packs, electric heating pads, forced-air warming, and body-to-body warming. 10 –13 Some of these studies included insulation only or insulation combined with a heat source; however, we are unaware of any study comparing complete systems that all include an insulating enclosure, vapor barrier, and heat source (eg, a heated hypothermia wrap [HHW] system). This combination is advantageous because it not only improves total body heat balance but also provides thermal comfort; it is also more relevant for actual use in prehospital settings.
Research and teaching on the care of cold-exposed patients often focuses on the search for the “single, best device or strategy.” However, it is important to note that responders need not focus on finding one single, best method.14,15 Rather, there may be several effective and acceptable methods, the choice of which may depend on practical factors such as cost, weight, volume, whether and how much heat is donated, the amount of insulation provided, and the conditions for its intended use (eg, at the scene and/or during human-powered or motorized transport).
The HHW systems for prehospital use are either available commercially or can be assembled piecemeal by the response team (user-assembled). In some cases it may not be feasible to purchase and use a commercial HHW. A user-assembled HHW may be preferable because it can be cheaper and its volume and weight are usually lower and can be varied dependent on the season (eg, the enclosure can vary from a light single-season bag to a heavy winter bag, and the number of heat sources can also be varied).
Although several commercial HHWs are available, their relative efficacy has not been directly compared. It is also not known how a user-assembled HHW would compare to these commercial units. Therefore, 4 commercial HHWs that are among the most commonly used and 1 user-assembled HHW were compared for their physiologic responses (skin and core temperature, shivering heat production, skin heat loss, and body net heat gain) and subjective ratings (cold, shivering, and comfort) for system effectiveness in reducing heat loss and providing heat. Three commercial HHWs (Doctor Down, MARSARS, and Wiggy's) are typical systems with heavy-weight enclosures. The fourth commercial HHW (the hypothermia prevention and management kit [HPMK]) has a compact, light design and a single-layer enclosure with no added insulation; it is commonly used by military organizations.
Because these systems are designed for protection of cold-exposed patients, whether injured but still normothermic or actually hypothermic, they should insulate maximally and provide the most efficient amount of heat possible with 2 main goals: 1) prevent a normothermic patient from becoming hypothermic; or 2) stabilize or increase the core temperature of a hypothermic patient. Thus, arguments could be made to study either normothermic or hypothermic subjects. Because we are most interested in the differences in heat donation through the skin and total body net heat gain, we chose the former; we did not feel this analysis justified exposing subjects to discomfort and the potential complications of becoming hypothermic on 5 occasions.
The systems were tested in cold air (−22°C) for 60 min; however, core temperature was not expected to change with any system. Although subjects were likely to feel cold and even shiver in some trials, it was expected that the combination of insulation, applied heat, and shivering heat production would prevent any decrease in core temperature in healthy subjects over 60 min. It is reasonable to expect, however, that any significant changes in net heat gain might eventually result in meaningful changes in core temperature over an extended period of time in a cold, and possibly traumatized, patient.
Therefore, the following systems (all including an enclosure, vapor barrier, and heat source) were compared: 1) user-assembled; 2) Doctor Down Rescue Wrap; 3) HPMK; 4) MARSARS Hypothermic Stabilizer Bag; and 5) Wiggy's Victims Casualty Hypothermia Bag. It is important to note that it was not the purpose of this study to measure technical aspects of the enclosure bags, such as insulation values and dead air space. Rather, the study focused on the practical effectiveness of the systems as indicated by primary outcomes of decreased skin heat loss and higher body net heat gain, with secondary outcomes including higher average skin temperature, lower shivering heat production, and better subjective ratings.
We hypothesized that the MARSARS system would be the most effective because of its large mass of insulation combined with the fact that its gel chemical heat packs cover more of the high–heat-transfer areas (chest, axillae, and upper back). We also hypothesized that the HPMK system would be least effective because of its lack of insulation.
Methods
SUBJECTS
Five volunteers (1 female) (aged 18–45 y) were recruited through word-of-mouth from the university community. Subjects were eligible if they were healthy, physically active, and free from any cardiorespiratory conditions or conditions exacerbated by cold exposure. The protocol was approved by the education/nursing research ethics board at the University of Manitoba. A signed informed consent was obtained from each subject.
Sample size was calculated according to similar data comparing heat loss (one of the primary outcome variables in the present study) through various body covers. 16 To achieve 95% power (α=0.05, 1-tailed test; β=0.05; power index of 3.28), the sample size required to detect a statistically significant difference (mean±SD) for heat loss of 14±8 W was 4. Thus, although we normally test 6 subjects in this type of study, given the number of conditions to be tested with each subject, we believed that 5 would provide enough power to detect important practically significant differences, if any existed.
INSTRUMENTATION
Subjects wore underwear, gym shorts, and a short-sleeve shirt or T-shirt. A single-channel electrocardiogram monitored heart rate. Core temperature was measured with a disposable esophageal thermocouple (T
SUBJECTIVE RATINGS
Likert-type scales were used for the following subjective variables.
Whole body cold discomfort
Every 10 min, subjects provided ratings ranging from 0 (no sensation of cold) to 10 (unbearable cold) (Table 1). 19
Subjective scales used for whole-body cold discomfort, overall temperature, and system preference
Overall shivering rating
After 60 min of cold exposure, subjects estimated their level of shivering as 1 (no shivering), 2 (low shivering), or 3 (high shivering).
Overall temperature rating
After 60 min of cold exposure, subjects rated their thermal sensation, ranging from 1 (very warm) to 5 (very cold) (Table 1).
Preference ranking
At the end of their final trial, subjects ranked the 5 systems ranging from 1 (most preferred) to 5 (least preferred) (Table 1).
ENCLOSURE SYSTEMS
Four commercial and 1 user-assembled HHW systems were studied (Figure 1, Table 2). The commercial systems are among the most commonly used by response units across Canada and the United States. Internal vapor barriers and chemical heat packs were used with all systems. Three systems used gel chemical heat packs, which can be “recharged” after use by being put in boiling water until the solidified gel becomes liquid again. Two systems used dry chemical heat packs, which were disposable.
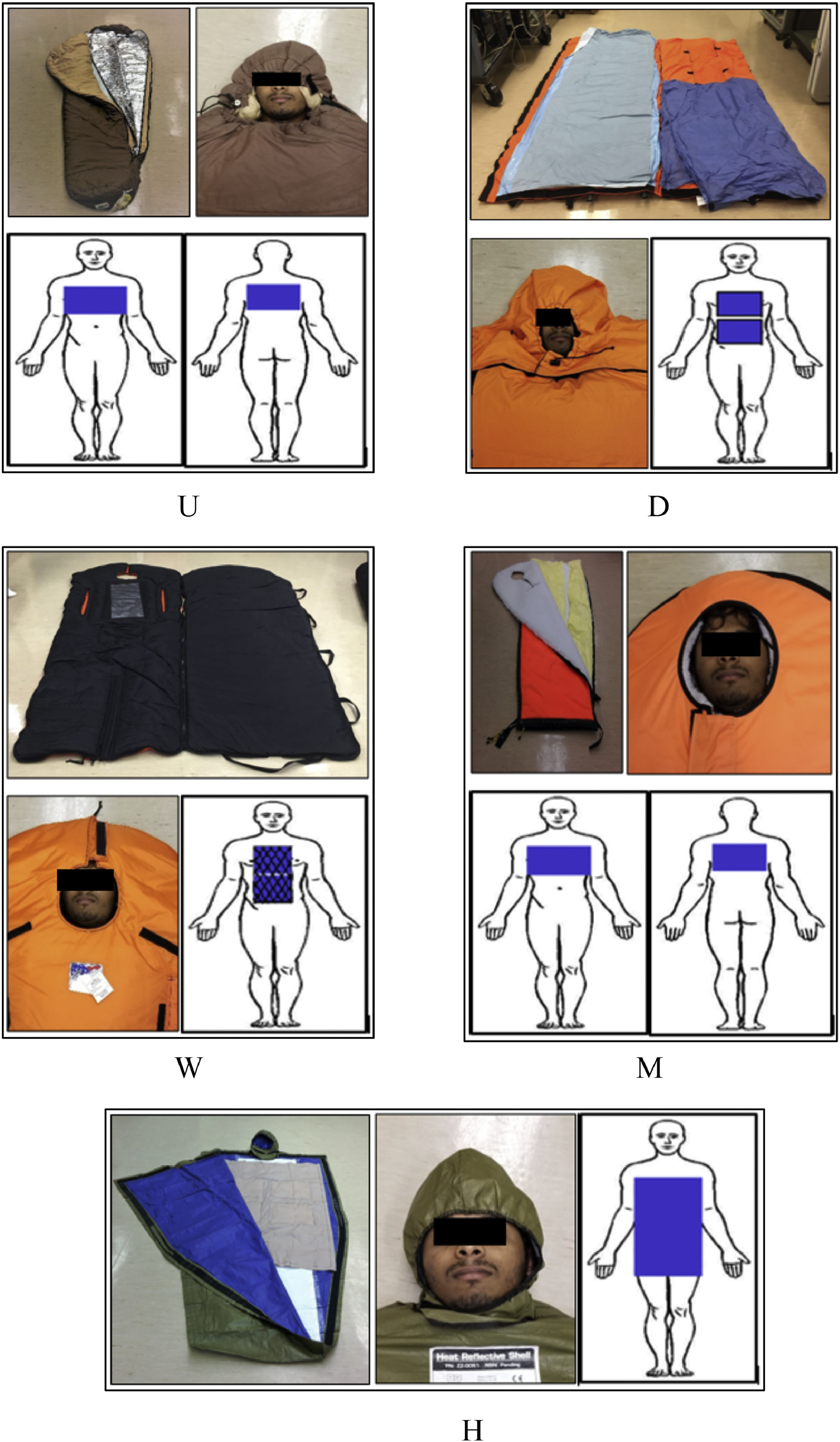
Five heated hypothermia wrap systems, each section showing the enclosure, a view of the head/face, and placement and size of the chemical heat source(s). Gel or dry chemical type indicated for each system as follows: U) user-assembled system (gel); D) Doctor Down (gel); W) Wiggy's (dry); M) MARSARS (gel); and H) Hypothermia Prevention and Management Kit (dry).
Characterists of heated hypothermia wrap systems (listed and shown in order of packed volume)

HPMK, Hypothermia Prevention and Management Kit.
Four dry chemical heat packs inserted in 1 heat blanket.
User-Assembled System
Because the user-assembled system is assembled piecemeal, the enclosure can range from a very light to a very heavy sleeping bag. In this case, a midweight bag was used. The 3-season mummy-style hooded sleeping bag measures 70 × 220 cm and weighs 2.3 kg (Hollofil II insulation; Mountain Equipment Co-op). A drawstring allowed tightening of the hood around the face. A separate internal vapor barrier (reflective blanket) was used with the reflective side toward the subject. Three gel chemical heat packs (sodium acetate salt solution; 20 × 46 cm and 1.1 kg; ThermoPad Re-usable Heat Pad, Hood Thermo-Pad Canada Ltd; these heat packs are commonly used by the Canadian Coast Guard) were placed on the chest, axillae, and upper back. 20 The gel packs were activated 10 min before application.
Doctor Down Rescue Wrap
This bag (11-1001, Doctor Down Inc, Polson, MT) measures 94 × 203 cm and weighs 6.4 kg. The outer shell is made of storm-tech (3-layer multipolymer) and is breathable, waterproof, and windproof. It includes a disposable vapor-proof liner that absorbs biological fluids. An insulated hood was attached to the bag. A drawstring allowed tightening of the hood around the face. The bag has 2 pockets (27.5 × 28 cm) inside of the top layer at the chest and abdomen level to hold 2 gel chemical heat packs (sodium acetate salt solution; 20 × 20 cm and 0.6 kg; Doctor Down Re-usable Heat Pack). The gel packs were activated 10 min before application.
Hypothermia Prevention and Management Kit
The total system (North American Rescue, Greer, SC) weighs 1.6 kg. The enclosure bag measures 109 × 198 cm and weighs 0.8 kg; it is tapered toward the feet and has an attached hood with a drawstring to allow tightening of the hood around the face. It is a tough, water- and wind-proof shell made from a polyolefin 4-ply composite fabric. The system includes a 4-panel dry chemical heating blanket (Ready-Heat; 86 × 122 cm and 0.8 kg). The total system is enclosed in a vacuum pack, which measures 17 × 27 × 14 cm. The heating blanket covered the subject's chest, axillae, and abdomen. The dry chemical heat pads are activated by exposure to air for 10 to 20 min before application.
MARSARS Hypothermic Stabilizer Bag
This bag (MARSARS Water Rescue Systems Inc, Shelton, CT) measures 70 × 210 cm and weighs 5.4 kg. It has a polyester–pile liner. The bag is waterproof and windproof. There is no separate hood; rather, a 17.5 cm diameter hole is inserted in the top surface to accommodate the face. There is no drawstring to tighten the blanket around the face. A separate internal vapor barrier (Bio-liner, Safecross First Aid, North York, Canada; 142 × 229 cm and 0.3 kg) was used inside the bag. The top insulation shell is made of 240 denier nylon, and bottom insulation shell is made of 1000 denier cordura nylon. This bag has no pockets to contain a heat source. However, the manufacturer provides 3 reusable gel chemical heating pads (Heat Solution, Pristech Inc, San Antonio, TX; 19 × 42 cm and 1.1 kg). Two felt pouches are provided to contain the heat packs. A long pouch (91 × 20 cm) holds 2 heat packs and was placed on the chest and axillae. A shorter pouch (45 × 20 cm) holds 1 heat pack and was placed beneath the upper back. The gel packs were activated 2 min before application.
Wiggy's Victims Casualty Hypothermia Bag
This bag (Wiggy's Inc, Grand Junction, CO) measures 88 × 229 cm and weighs 3.6 kg. The top panel's exterior and interior lining are made of 200 denier oxford nylon, and the bottom panel linings are made of 1000 denier cordura nylon. There is no separate hood; rather, a 15 cm diameter hole is inserted in the top surface to accommodate the face. There is no drawstring to tighten the blanket around the face. The interior and exterior of the bag are waterproof; therefore, no separate vapor barrier was needed. This bag has a mesh chest pocket (62 × 30 cm) on the inside of the top layer, which can hold 1 or 2 chemical heat pads against the chest and abdomen. However, this manufacturer does not supply any heat packs. Therefore, 2 disposable dry chemical heating pads (Ready-Heat; 1 panel, TechTrade; 15 × 20 cm and 0.2 kg) were placed inside the pocket. The dry chemical heat pads are activated by exposure to air for 10 to 20 min before application.
COMPARISON OF CHEMICAL HEAT PACK TYPES
One benchtop trial was conducted to determine the general temperature profiles of the uninsulated surfaces of the 5 heat sources. Surface temperatures were measured for 25 hours after simultaneous activation at an ambient temperature of ∼23°C.
PROTOCOL
Subjects were each studied 5 times (once for each HHW) at approximately the same time of day, with each trial separated by at least 48 h. The protocol followed a repeated measures design with the order of conditions following a balanced design. After instrumentation, subjects sat for 10 min of baseline measurements. They then lay supine on a movable bed and were enclosed in one of the hypothermia wrap systems. The bed was then rolled inside a cold chamber (−22°C). Every 10 min, subjects were asked to provide subjective feedback. Feedback included whether skin that was in contact with the heat sources felt too hot, as an indication of potential skin burning. There were no such incidents, as would be expected within the short 60-min period of warming, especially if skin blood flow was not compromised by injury, disease, or other factors. After 60 min, subjects were removed from the cold chamber and warmed, if necessary.
DATA ANALYSIS
The 12 skin sites for each temperature/heat flux probe were assigned regional percentages adapted from Layton et al 21 as follows: head—forehead (9%); upper torso—right chest (4.5%), left chest (4.5%), axillae (4.5%), and upper back (4.5%); lower torso—mid abdomen (6%), lateral abdomen (6%), and lower back (6%); arms—posterior arm (7%), anterior arm plus hand (12%); and legs—anterior leg (18%), posterior leg (18%). The sum of regional percentages equaled 100%, and positive heat flux values indicated heat loss to the environment.
The area-weighted skin temperature (°C) was calculated for the total body (TskTotal) and for the anterior torso (TskTorso).
Heat flux (W) for each of the 12 sites was calculated. If a site was either not covered by a heat source at all or was completely covered by a heat source, the site regional percentages listed were used as follows:
If a site was partially covered by a heat source, the area within the site that was exposed to the heat source was directly measured. Heat flux for that site was then calculated as the sum of heat flux from the heated surface area and nonheated surface area as follows:

Therefore, for each condition, heat flux values represent 100% of the total BSA. The total body skin heat flux (HFTotal) (all 12 sites) and torso skin heat flux (HFTorso) (7 torso sites) were then calculated by adding absolute values of heat flux from the appropriate sites.
Metabolic heat production (M [W]) was calculated
22
and respiratory heat loss (RHL [W]) was computed from metabolic heat production as follows23,24:
Finally, net heat gain (NHG) was calculated as follows:
All statistical analyses were accomplished with the SigmaStat package within SigmaPlot 14. Because the study was not designed to detect whether system differences were sex dependent, all data were pooled before analysis. Repeated-measures 2-way analysis of variance (factor A, enclosure type; factor B, time) compared the physiological variables. Post hoc analyses for significant differences were accomplished using the Holm-Sidak post hoc test.
A nonparametric test (Friedman analysis of variance) compared the subjective responses. Post hoc analyses for significant differences were accomplished using an “all pairwise multiple comparison procedure” (Student-Newman-Keuls Method). P<0.05 was considered significant for all tests.
Results
The 5 subjects were 29.4±4.2 y old. See Table 3 for further details.
Characteristics for 1 female and 4 male subjects
BSA, body surface area.
Mean and SD values provided for males.
HEAT PACK SURFACE TEMPERATURES (BENCHTOP TRIAL)
All gel chemical heat pack surfaces warmed similarly and to a higher temperature (up to 47°C) than the dry chemical heat packs for 60–90 min, but then cooled off rapidly (Figure 2). Although dry chemical heat packs remained warm for more than 8 hours, they did not reach a very high temperature (<40°C). Figure 2 (inset) shows these temperature profiles specifically for the first 2 h, a period that would encompass many rescue scenarios.
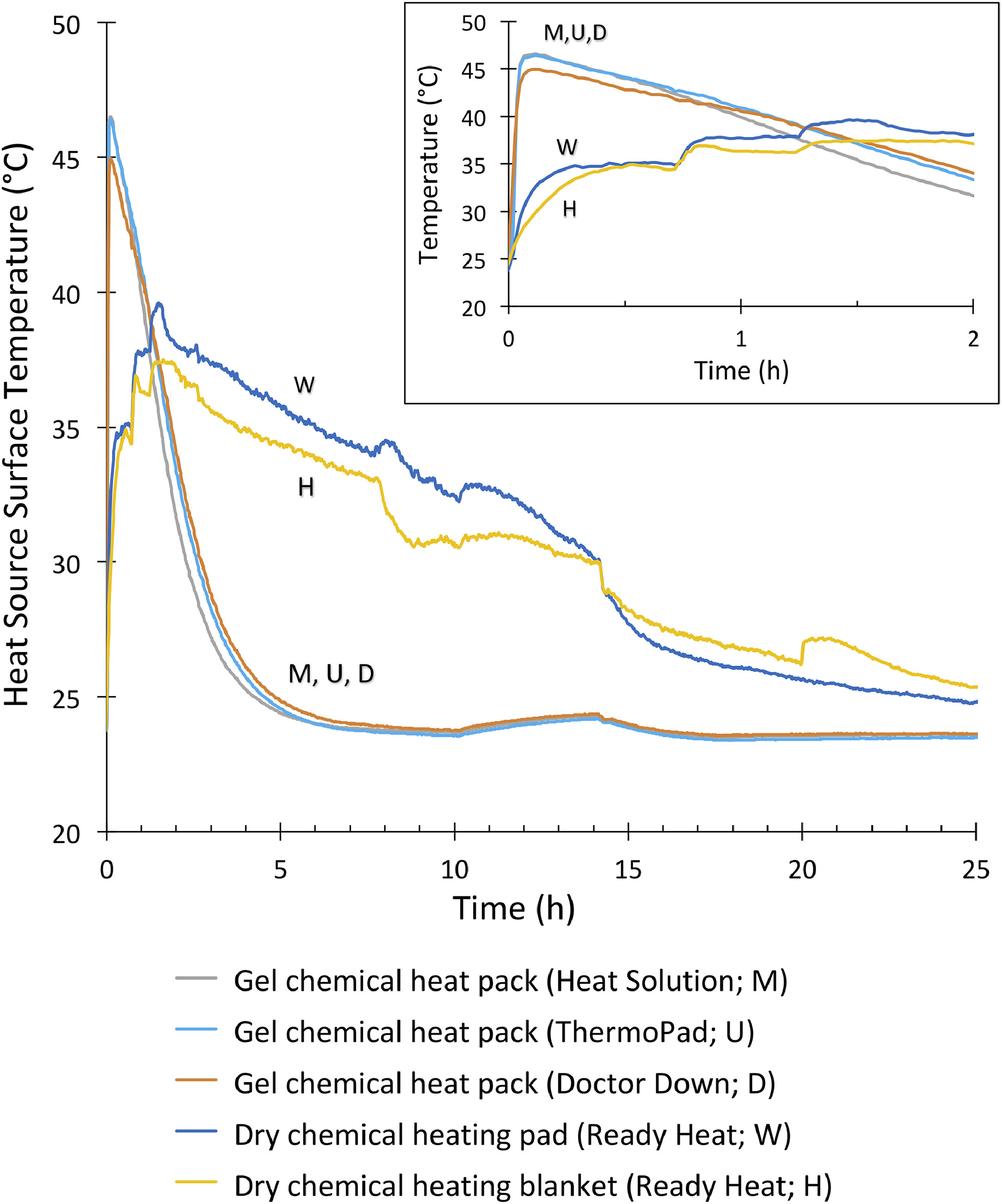
Temperature profile for the uninsulated surface of 5 chemical heat sources at an ambient temperature of 23°C for 25 h. Time 0 indicates activation. Inset provides data for only the first 2 h.
CORE TEMPERATURE
As expected, Tes was normal during baseline for all conditions (37.2±0.2°C) and did not change throughout any of the trials for any of the systems.
AVERAGE SKIN TEMPERATURE
For TskTotal (Figure 3, top), there was statistical significance for condition, time, and interaction (P<0.001 for each factor). After 60 min of cold exposure, TskTotal was significantly lower than baseline with HPMK and Wiggy's and higher than baseline with Doctor Down and user-assembled (P<0.05). Throughout cold exposure TskTotal was generally higher with Doctor Down and user-assembled and lower with HPMK. TskTotal values for MARSARS and Wiggy's were in the middle, with MARSARS and Wiggy's being greater than HPMK and lower than Doctor Down, and Wiggy's being lower than user-assembled (P<0.05).
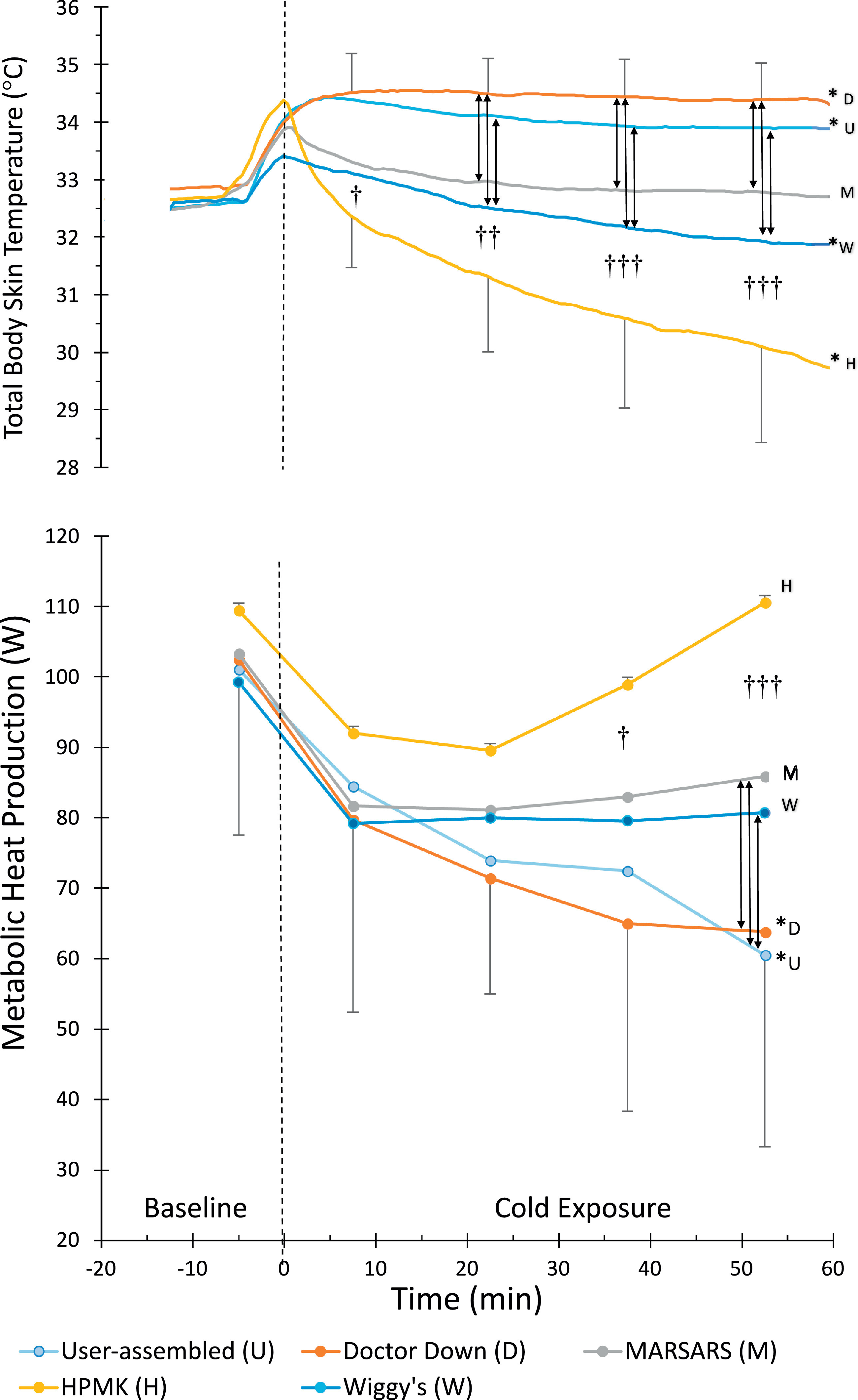
Total body skin temperature (top) and metabolic heat production (bottom). Time 0 indicates entrance to the climatic chamber (bars, SD). HPMK, Hypothermia prevention and management kit. * Significantly different from baseline. † HPMK different from Doctor Down and user-assembled. †† HPMK different from all but Wiggy's. ††† HPMK different from all other systems (P<0.05). Vertical lines (with arrow heads) indicate other significant differences (P<0.05). For clarity, SD bars are only included for top and bottom lines, and system type is indicated at the end of each line.
After 60 min of cold exposure, TskTorso was significantly higher with user-assembled (37.5±0.4°C) and HPMK (37.4±0.4°C) than with Wiggy's (36.3±0.2°C) (P<0.05). Values for Doctor Down (37.1±0.8°C) and MARSARS (37.0±0.4°C) were not different from any system. Forehead skin temperature was lower for MARSARS (15.1±4°C) compared with user-assembled (30.4±1°C) and Doctor Down (29.2±2°C) (P<0.01); no statistical significance was shown for HPMK (21.1±3°C) or Wiggy's (21.2±8°C).
METABOLIC HEAT PRODUCTION
For metabolic heat production (Figure 3, bottom), there was statistical significance for condition (P<0.001), time (P<0.001), and interaction (P=0.003). There were no differences during baseline and the first 30 min of the cold exposure. During the last 15 min, however, heat production was higher with HPMK than with all other systems (P<0.05). User-assembled and Doctor Down systems were the only conditions with values below baseline at the end of cold exposure (P<0.05). Values for MARSARS and Wiggy's were in the middle, with MARSARS and Wiggy's being lower than HPMK and greater than user-assembled, and MARSARS being greater than Doctor Down (P<0.05).
HEAT FLUX
For total body HF (Figure 4, top), there was statistical significance for condition (P<0.001), time (P=0.016), and interaction (P<0.001). Total heat loss with HPMK, MARSARS, and Wiggy's systems was higher than that of the other 2 systems throughout cold exposure and was higher than baseline at the end of cold exposure (P<0.05).
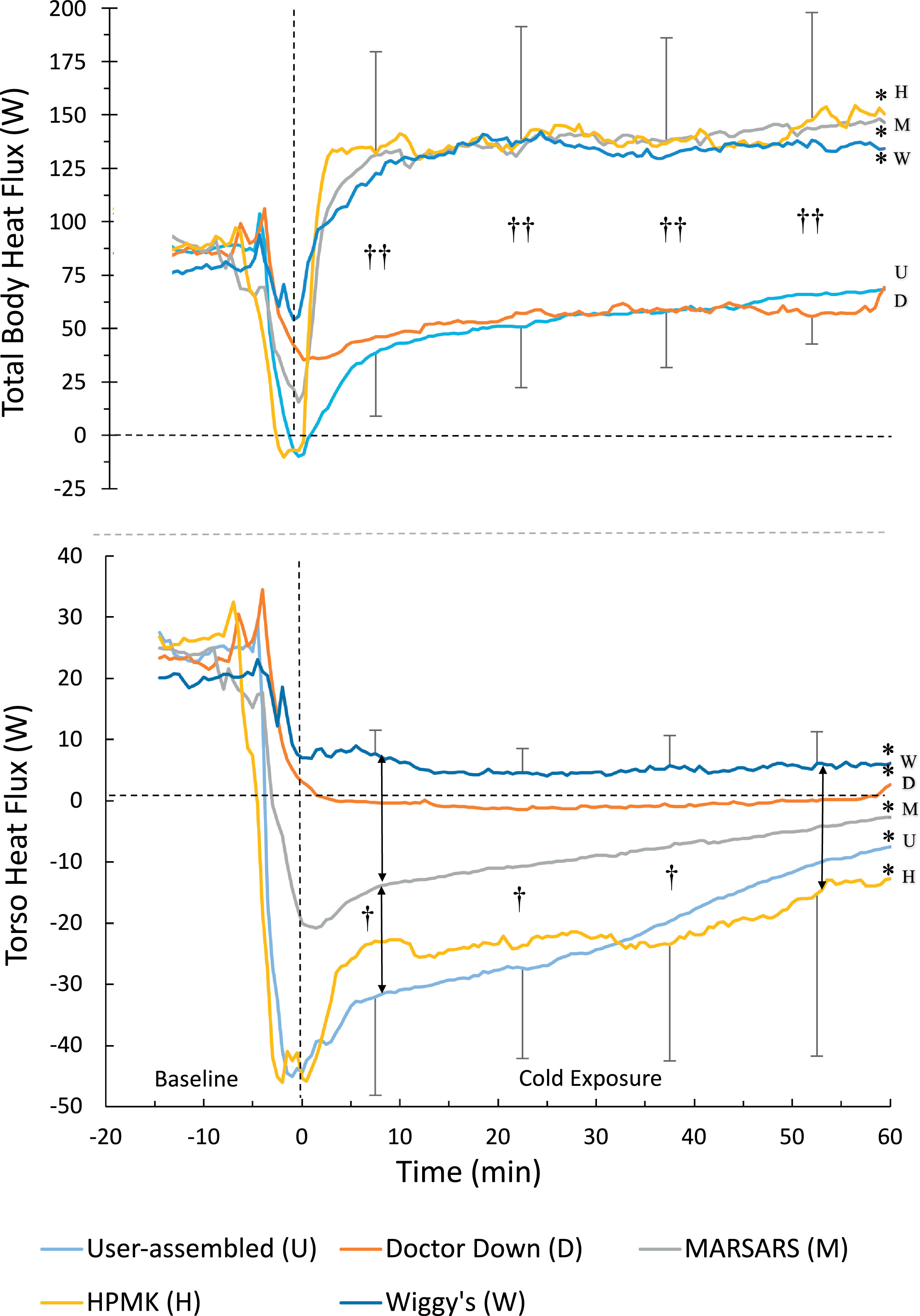
Total body heat flux (top) and torso heat flux (bottom). Time 0 indicates entrance to the climatic chamber (bars, SD). * Significantly different from baseline. †† HPMK, MARSARS, and Wiggy's greater total heat loss than user-assembled and Doctor Down. † User-assembled and HPMK greater torso heat gain than Doctor Down and Wiggy's (P<0.05). Vertical lines (with arrow heads) indicate other significant differences (P<0.05). For visual clarity, SD bars are only included for top and bottom lines, and system type is indicated at the end of each line.
For torso HF (Figure 4, bottom), there was statistical significance for condition (P=0.003), time (P<0.001), and interaction (P<0.001). During the first 45 min of cold exposure, there was more heat gain (negative values) through the torso with user-assembled and HPMK than with Doctor Down and Wiggy's (P<0.05). By the end of cold exposure, only the difference between Wiggy's and HPMK was significant; however, values for all conditions were different from baseline (P<0.05).
NET HEAT GAIN
For net heat gain (Figure 5), there was statistical significance for condition (P=0.003), time (P=0.003), and interaction (P<0.001). During the first 30 min of cold exposure, net heat gain was positive and higher with Doctor Down and user-assembled compared with the other 3 systems (P<0.05). By the end of cold exposure, these differences became less evident. However, at this point the HPMK, Wiggy's, and MARSARS values were lower than baseline (P<0.05), whereas Doctor Down and User-assembled remained at baseline values.
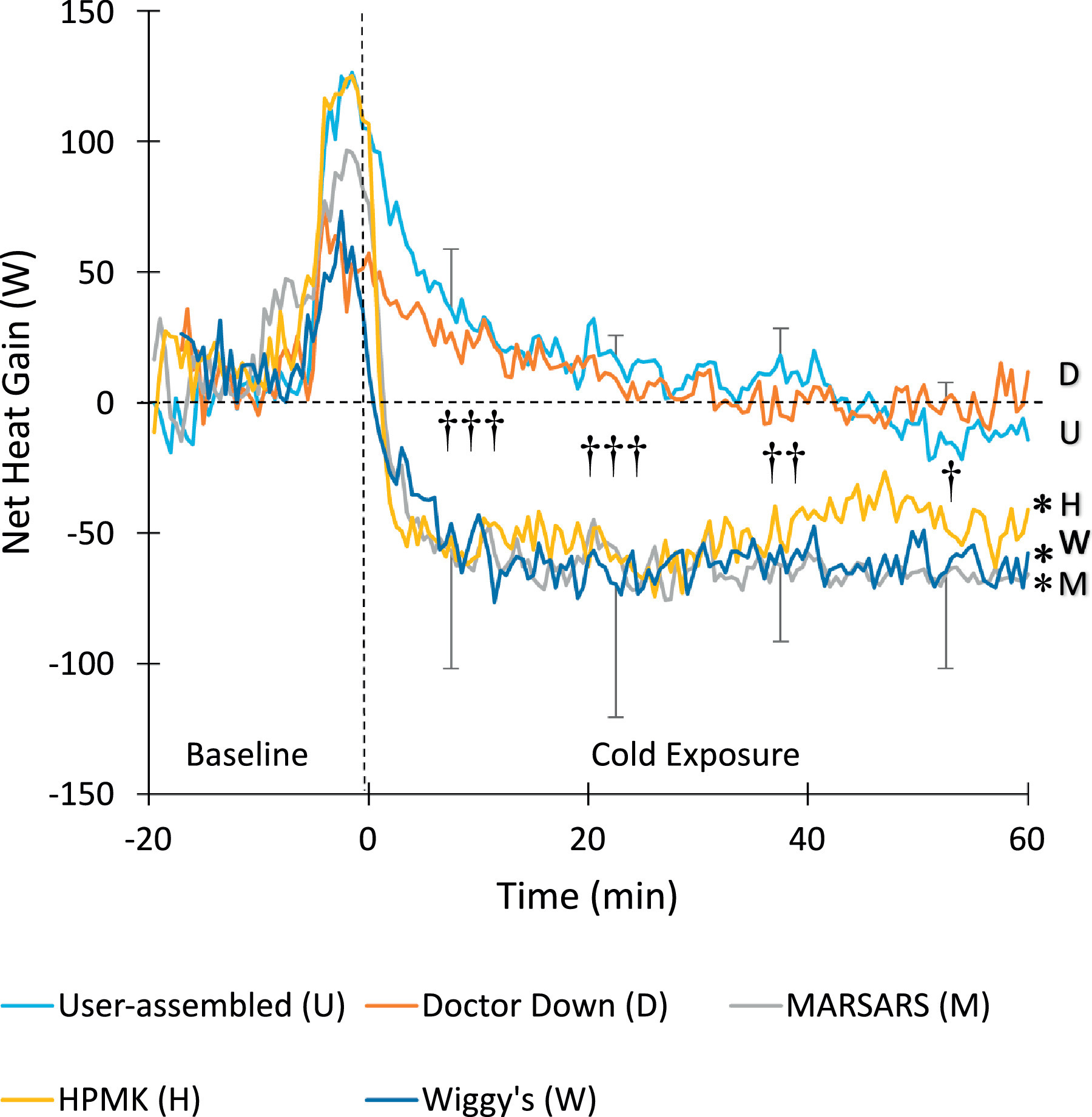
Net heat gain. Time 0 indicates entrance to the climatic chamber (bars, SD). * Significantly different from baseline. ††† Doctor Down and user-assembled different from MARSARS, HPMK, and Wiggy's. †† Doctor Down and user-assembled different from Wiggy's and MARSARS, and Doctor Down is also different from HPMK. † Doctor Down and user-assembled different from MARSARS, and Doctor Down also different from Wiggy's (P<0.05). For clarity, SD bars are only included for top and bottom lines, and system type is indicated at the end of each line.
SUBJECTIVE EVALUATIONS
Table 4 lists the median values for the subjective responses. Data for all four scales passed both the normality and equal variance tests. For both the whole-body cold discomfort and overall temperature ratings, median HPMK values were significantly higher (indicating feeling colder) than all other systems (P<0.05); this is consistent with the colder skin temperature shown in Figure 3. No significant differences were detected for overall shivering rating or preference ranking.
Subjective results presented as median (range) for 5 subjects for 4 subjective rating scales
HPMK, Hypothermia prevention and management kit.
Whole-body cold discomfort scale from 0 (no sensation of cold) to 10 (unbearable cold).
Overall shivering rating from 1 (no shivering) to 3 (high shivering).
Overall temperature rating from 1 (very warm) to 5 (very cold).
Preference ranking from 1 (most preferred) to 5 (least preferred).
Significantly different from all other conditions (P<0.05).
Discussion
This was the first study to compare commercial and user-assembled HHW systems that each included passive insulation enclosures, vapor barrier, and active warming sources. The Doctor Down and user-assembled systems were generally more effective, with higher skin temperatures and lower metabolic heat production; they allowed less heat loss, resulting in higher net heat gain.
We hypothesized that the MARSARS system would result in greater net heat gain. Our results did not support this specific hypothesis. The MARSARS system resulted in a lower facial skin temperature, likely because the face opening could not be tightened around the face. It is also noteworthy that 3 subjects believed that this system was very tight, with 1 subject terminating the trial early because he felt claustrophobic.
We hypothesized that the HPMK system would be least effective. As predicted, this system had the lowest skin temperature and highest shivering heat production. It also scored worse than the other 4 systems for the whole body cold discomfort and overall temperature ratings. Although the HPMK system had significantly lower skin temperature than all systems and higher total heat loss than user-assembled and Doctor Down, it actually allowed less torso heat loss than the Wiggy's system (likely because the HPMK's large heating blanket covers the entire torso).
Some previous studies have compared insulation-only systems to one or more combinations of insulation and warming systems. Zasa et al 9 and Allen et al 25 confirmed that active heating provided a benefit when added to an insulated enclosure. Watts et al concluded that a hot pack combined with a cotton blanket was better than various isolated insulations for trauma patients during prehospital transport. 13 However, Lundgren et al failed to demonstrate a positive effect of combined active and passive warming devices during transport, 26 possibly because all patients were already in a warm transport vehicle.
We are aware of only 1 previous study in which all conditions included active warming. Lundgren et al compared 4 active torso warming devices (albeit with the same insulation bag) using a human model of severe hypothermia in which shivering was pharmacologically inhibited. They found that 2 hot water bags, or a charcoal heater, produced higher rewarming rates than 2 gel chemical heating pads. 12 It is difficult to compare our results to the results of these other studies because ours is the only one to include insulation, vapor barrier, and active heating in all 5 systems.
POSSIBLE MECHANISMS FOR THE RESULTS
From a physiologic perspective, the user-assembled and Doctor Down systems were more effective. This can be explained by the mass of insulation material (Doctor Down); low dead space (mummy style bag in the user-assembled system); gel heat packs, which provide more heat in the first hour or two; or the areas covered by these packs. With the user-assembled system, the 3 gel chemical heat packs covered a large surface area (chest, axillae, and upper back). With the Doctor Down system, the greater amount of insulation compensated for the fact that the 2 gel heat packs covered a smaller area and were confined to the chest and abdomen.
Although the MARSARS system provided a higher mass of insulation and its 3 gel chemical heat packs covered a large surface area, it was less effective than the user-assembled and the Doctor Down systems. This system was uncomfortably tight for 3 of the 5 subjects. Subjects also reported having a cold face with MARSARS, likely because this was the only system that did not allow minimization of face exposure by covering the forehead. Wiggy's also did not have a drawstring, but there was enough head room above the face opening to allow placement of the forehead under the cover (Figure 1). We measured the temperature of the forehead because this is an area that should, and can, be insulated without obscuring patient vision or compromising airway access.
Physiologic responses with the Wiggy's system were similar to those of the MARSARS system (ie, less effective than Doctor Down and user-assembled). This is consistent with Wiggy's moderate mass of insulation and smaller surface area of heating. Its 2 dry chemical heating pads (which provide less heat than gel packs) were placed over the chest and abdomen; the abdomen is not as effective for heat transfer as the axillae. Lower effectiveness of the HPMK system is not surprising given that the enclosure is thin and has no added insulation. The main advantages of the HPMK, however, are its large warming blanket and its small volume and weight, which make it easier to transport to victims in a greater number of scenarios.
PRACTICAL IMPLICATIONS
The choice of HHW system will depend on multiple factors, including effectiveness, volume, weight, and cost. Thicker and heavier insulation generally prevents heat loss more effectively. The benchtop portion of this study demonstrated that gel chemical packs heat to a higher uninsulated surface temperature (up to 47°C) than do dry chemical heat packs, but they then cool off rapidly (Figure 2). Although dry chemical heat packs remain warm for more than 8 hours, they never reach a very high temperature (uninsulated surface temperature <40°C). Responders should always consider burn prevention when applying external heat to a patient. During the 60-min warming periods, maximum skin temperatures (seen on the chest, axillae, abdomen, or back) only reached 43°C (maximum of 43.4°C) in 3 of the 25 trials. In each case temperature started to decline within 5 min; thus, the risk of even minor skin burning was minimal. The risk would increase if manufacturer instructions were ignored and insulation was removed from between the skin and the heat pack.
Gel chemical packs are heavier but are reusable after being “recharged” in boiling water. Dry chemical packs require exposure to air to operate, so they cannot be wrapped in a vapor barrier indefinitely. Because the skin of a patient with heat packs must be examined approximately every 30 min to prevent burns, dry heat packs would still receive enough air to function properly. Gel heat packs might be safer and more efficient if the chemical content could be altered so the total energy could be expended more evenly over time.
Heat transfer effectiveness is dependent on the size of the pad(s) and application to areas of optimal heat transfer. The chemical heat packs used in the user-assembled and MARSARS systems were larger than the Doctor Down packs, and they were placed on the areas of high heat transfer (chest, axillae, and upper back) rather than the chest and abdomen.
The size of the enclosure bag is important. Optimally, dead air space within the bag should be minimal; however, the bag should not be so small that it causes discomfort or claustrophobia. Therefore, it would be an advantage to have adjustable straps on the outside of a larger bag so it can be snugged up against the victim to reduce dead air space within the bag. It is also important that the face opening be adjustable to cover the forehead and tighten around the face. Finally, it was beneficial that each system had at least 1 windproof layer, which is important to reduce convective and evaporative heat loss in windy conditions.
POTENTIAL LIMITATIONS
Insulation values of the enclosures were not measured, either as an average for the enclosure or specifically in compressed and uncompressed areas. This was not the focus of the study; rather, the focus was on the overall performance (eg, heat loss and balance, skin temperature, subjective ratings) of the complete systems as they are sold or assembled.
The study was open to both sexes, and only 1 woman volunteered. Although she was the shortest and lightest subject (Table 3), her results were similar to those of the male subjects and therefore did not skew our findings or conclusions. For example, for metabolic heat production and net heat gain, this subject's overall mean values for all 5 trials and for each individual condition were within 0.05 to 1.4 standard deviations of the group mean.
This study involved a small sample size (n=5), yet power analysis and the results themselves indicate that more subjects would be unlikely to reveal any different results related to the important variables studied or change any of the conclusions.
Finally, a recent comparison of BSA formulae has revealed discrepancies in calculated results by as much as 0.5 m2. 27 First, this variability is greater for people with abnormal physiques or for children; therefore, potential errors in our estimates would likely be much lower in our young, healthy subjects. Second, the significance of errors in BSA calculation is primarily important in clinical situations such as cancer chemotherapy, transplantology, and burn treatment, where BSA may affect choice of treatment or drug dosage. However, any errors in BSA in this study would be consistent for all subjects and conditions and therefore would not affect comparisons in heat flux or net heat gain.
Conclusions
Five HHW sytems, each containing an enclosure bag, vapor barrier, and heat source, were compared in a cold environment. The systems had great variability in weight, volume, cost, and effectiveness. The user-assembled and Doctor Down systems had superior physiologic performance (higher total body skin temperature and net heat gain, lower heat loss, and no shivering). Only the user-assembled and HPMK sytems could realistically be carried in backpacks, whereas the other sytems would require at least a sled, if not a vehicle or aircraft for transport to the victim. One further advantage of the user-assembled system is that a smaller or larger sleeping bag can be used and the number of heat sources can be varied as space allows or as environmental conditions change.
As expected, during the 1-h cold exposures, core temperature did not decrease with any of the systems studied, indicating that all could be effective in similar exposure types and durations. It is possible, however, that clinically important differences might be seen between systems with extended exposures of cold and/or injured patients, who themselves are at greater risk of becoming hypothermic. Future studies with more subjects and longer exposures, potentially with hypothermic conditions, may be valuable.
Footnotes
Funding
Financial support obtained from the Natural Sciences and Engineering Research Council Canada, UMGF, Duff Roblin Fellowship, and Faculty of Kinesiology and Recreation Management at the University of Manitoba.
Acknowledgment
The authors thank the Natural Sciences and Engineering Council of Canada.
Author Contributions
Study concept and design (GG, RD, PG, AS); obtaining funding (GG, RD); acquisition of the data (RD, KK, GG); statistical analysis of the data (GM, RD, KK, GG); drafting of the manuscript (RD, GG); critical revision of the manuscript (PG, AS, KK); and approval of final manuscript (GG, AS, PG, GM).
Financial/Material Support
Systems were provided for testing by MARSARS and Doctor Down. Remaining systems were purchased.
Disclosures
None.