
Abstract
We present a case report of a helicopter pilot who fell into a crevasse during a fuel delivery in Antarctica. He was trapped alone in the crevasse for 3 h while waiting for a rescue team to arrive, and a further 1 h during the extrication process. His condition deteriorated during the extrication and he lost consciousness and signs of life minutes after being dragged over the lip of the crevasse. He was then loaded into the rescue helicopter and treated with intermittent cardiopulmonary resuscitation during the 39-min return flight. Initial esophageal temperature on arrival at the Davis Base medical facility was 24.2°C. After 18 h of further treatment (mechanical ventilation with warm humidified O2, with internal and external warming) he was pronounced dead. The cause of death was hypothermia with minimal physical injury. This case highlights some of the extra challenges facing operational, rescue, and medical personnel in an isolated location. These complications include the tendency for flight crew to remove cold weather clothing during flight due to restricted mobility and excessive heat load from cabin heating; extended time for arrival of the rescue crew; extrication in a confined space; limited helicopter cabin space for transporting the rescue team and their rescue and medical equipment; and extended transport time to the nearest medical facility.
Introduction
Antarctica has many research stations with many workers deployed across the continent in harsh, potentially dangerous conditions. Risks include severe cold exposure and, in some areas, falling into a crevasse. The main threats to survival to a worker who has fallen into a crevasse are trauma, suffocation from inability to breathe, and cold exposure. 1
All stations should be prepared to adequately manage rescue operations that are relevant to their specific location and to treat injuries and medical conditions including severe hypothermia. Until the victim is raised to the snow surface, medical care is limited to basic measures. For example, if spinal injury is suspected, spinal immobilization may be attempted before raising the victim. 2 Similarly, if the patient is hypothermic, it would be advantageous to handle the patient as gently as possible, and preferably raise the victim in a horizontal position. 3 Extreme conditions may distract rescuers from the fact that rapid and rough handling, especially if the patient is vertical, may exacerbate the patient’s condition. 3
We present a case report of a helicopter pilot who fell into a crevasse during a fuel delivery in Antarctica. He was trapped alone in the crevasse for 3 h while waiting for a rescue team to arrive, and a further 1 h during extrication. He went into cardiac arrest about 10 min after being extricated from the crevasse and was pronounced dead 18 h after transport to a base medical facility, after prolonged efforts at resuscitation. This case highlights complications facing operational, rescue, and medical personnel in an isolated location. These include the tendency for flight crew to remove their issued cold weather clothing during flight due to excessive heating; extended time for arrival of rescue personnel; rescuer safety; accessing victims in confined spaces; freeing and raising wedged victims; extricating the victim over the crevasse edge; limited helicopter cabin space for transporting the rescue team and their rescue and medical equipment; and extended transport time to the nearest medical facility.
Case Report
The Australian Antarctic Division administers and supports research operations from Davis Base, Antarctica. In the summer of 2016, 2 helicopters (each with a single pilot occupant) delivered fuel from Davis Base to a fuel cache on the West Ice Shelf. One pilot (62 y, 188 cm, 96.8 kg) delivered his load and landed the helicopter to unhook the suspension system (longline cable, swivel, and drum hooks) from the fuel drums. After disconnecting the drum hooks from the drums, he carried the cable system (total weight ∼35 kg) to the helicopter rear door, where he broke through a snow bridge concealing a crevasse (Figure 1). He fell ∼15 m into the crevasse (Figure 2) until he became wedged vertically between the narrowing ice walls. Much of his weight was supported by his flight helmet, which was wedged between the ice walls; this allowed him to continue breathing, although no further movements were possible. Surface air temperature was ∼14°C.
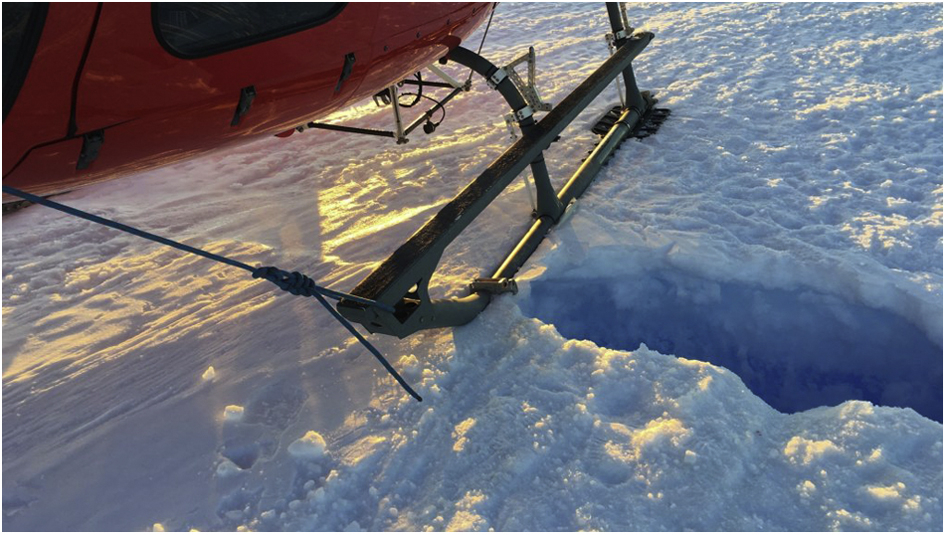
Helicopter and hole through which the pilot fell into the crevasse. The width at the surface was 60 cm.
Surface view of 60-cm wide crevasse with solid edges that allowed rescuers to stand securely near the crevasse edges.
During the incident, the cable and drum hooks also fell into the crevasse. The helmet was damaged by one of the hooks. The top of the crevasse was 60 cm wide, and it was possible to safely stand close to both edges.
The second pilot landed his helicopter nearby, approached the crevasse, conversed with the victim, and determined that he was relatively uninjured but cold and immobilized. He then departed for Davis Base to get help because he was unable to perform a rescue at the time. He immediately radioed the base to report the accident and the need for rescue.
The flight to base took 39 min. Following a 55-min turnaround, the helicopter departed with 3 field training officers (FTOs) who were trained in rescue techniques. This flight took 64 min due to strong headwinds. It is noteworthy that a medical practitioner, who had some cross-training in rescue techniques, was not included in the team due to space constraints on the helicopter, and advanced rescue training was deemed the priority. Also left behind was the medical practitioner’s equipment bag (including a monitor-defibrillator, oxygen and resuscitation equipment, and a portable automated external defibrillator).
At the accident site, extrication started following a 12-min site assessment (elapsed time in the crevasse, 179 min). The victim was conscious and “yelling” loudly enough to be heard on the surface. One FTO was lowered and inverted himself to reach the victim, who was found in a vertical position with both arms above his head. At this point, he still had enough strength to grasp the cable so tightly that his fingers had to be pried loose.
Initial efforts to free the victim from his wedged position were made by wrapping 25 mm-wide webbing around the victim’s right arm near the elbow. The sling was attached to a haul rope from an improvised hauling system, which had a 9:1 mechanical advantage. It took significant effort from the 2 FTOs and the pilot on the surface to pull hard enough to free the victim. A sling was then placed under his armpits (because he was not wearing a harness), and he was hauled to the surface in a vertical position.
During this period, the rescue team remembered from their training that if a casualty has been cold for a long time, special care must be taken during handling. Although it was preferable to place the victim in a horizontal position, this was not attempted for 2 reasons: 1) owing to the victim’s deteriorating condition, it was believed that this would take too much time; and 2) the crevasse was not wide enough for the victim to lie in a supine position, which is typical when someone is supported horizontally. The option of rotating the victim in the frontal plane (eg, in a cartwheel motion) so he was horizontal, but on his side, was not considered. Once the victim reached the lip of the crevasse, he was quickly pulled by the waist over the edge onto the snow surface.
Total time for approach plus extrication was 61 min, during which the victim’s condition deteriorated to being unresponsive and in respiratory distress. Soon after removal from the crevasse, he rolled into a fetal position and lost consciousness. He was placed in a hypothermia bag, put on a stretcher, and loaded into the helicopter 9 min after removal from the crevasse. Shortly thereafter, there was a change from rigidity to relaxation, eyes were open with pupils dilated, and there was no breathing or palpable pulse. During the return flight to Davis Station, one FTO performed an extended carotid pulse check and then performed intermittent cardiopulmonary resuscitation (CPR) as his endurance allowed. Three water bottles, which had been filled with warm water 2 h 40 min previously, were placed in the bag. Two FTOs remained on site because the helicopter had no room for them. Upon arrival at Davis Base, the victim’s esophageal temperature (Tes) was 24.2°C. The base doctor immediately commenced resuscitation efforts consisting of external warming (forced-air warming), internal warming (3 L of warmed IV saline and warm bladder lavage), and intubation and ventilation with warm humidified O2. The doctor was assisted by 4 lay surgical assistants and 6 other staff members who rotated in shifts. After ∼18 h, Tes had increased to 32°C, but there were no signs of life and the patient was pronounced dead.
Postmortem examination indicated no significant internal or external injuries, with the exception of an area of brown/black necrotic skin over the anterior aspect of the right elbow. This was likely caused during the initial extrication process when all force was applied through the sling to the right arm. This probably caused a combination of crush damage to the muscle and an ischemic injury to his entire right forearm. The cause of death was stated as hypothermia leading to cardiac arrest.
Every ground and surface worker, as well as every pilot, is issued a high-insulation protective clothing ensemble for the Antarctic environment. In this case, the pilot had taken this suit off because it was uncomfortably warm to wear while flying. When he fell in the crevasse, he was wearing only a cotton T-shirt, a light long sleeve polar fleece jacket, heavy cotton/polyester pants, wool socks, fingerless wool mittens, rubber booties, and his carbon fiber flight helmet.
Discussion
This case provides valuable insights into the risks and difficulties in working, and providing rescue and medical care, in isolated extreme environments. The victim’s condition worsened throughout the ∼60-min extrication due to continued cold exposure.
We have considered the victim’s signs and symptoms, in combination with the cold exposure survival model, 4 to estimate that his core temperature decreased from ∼31.5°C to ∼28.0°C during the extrication. At heart temperatures below 28°C, the heart may spontaneously go into ventricular fibrillation cardiac arrest, as a primary result of cooling the heart tissue. Ventricular fibrillation can also be provoked by mechanical stimulation such as rough handling during extrication and by additional toxins released from crush injuries and prolonged tissue ischemia. 5 Finally, ventricular fibrillation can also be precipitated by increasing the workload of a cold heart, as might occur during hypotension caused by blood pooling in the legs (common with cold patients in a vertical position, as well as during suspension or harness hang syndrome).6,7 This positional hypotension can be exacerbated by decreased epinephrine output (a proposed mechanism for rescue collapse, also referred to as circum-rescue collapse). 8 Thus, the combination of raising the victim in a vertical position and quickly pulling him over the crevasse edge may have contributed to unconsciousness and subsequent lack of discernable cardiac activity. Based on these mechanisms, a cold victim should be placed in a horizontal position as soon as possible. 3 It is not known if this procedure would have altered the outcome in this case.
Several factors might have decreased the probability of this case ending in a fatality. First, if the victim had been wearing his thermal protection suit, his rate of core cooling would have been slowed and his chance of survival would have increased. Second, anything that could have shortened the interval before the extrication process started would have decreased the exposure time and therefore the amount of core cooling. Finally, any actions to handle the victim more gently or facilitate a horizontal extrication might have delayed or prevented cardiac arrest.
The rescue team performed a very complicated rescue in a very confined space, where accessing the victim required extraordinary measures. They recalled several cold-related rescue principles, such as the need to go slow to handle cold patients gently, and the benefits of raising the victim in a horizontal position. However, both principles were very difficult to apply in these conditions.
The team did not attempt to transition the victim to a horizontal position for several reasons, including that they did not think they could spare the extra 7 to 12 min to do so, and the crevasse was not wide enough to place him in the traditional supine position. We believe, however, that in a 4-h cold exposure, taking this extra time to transition the victim to a better position would not have worsened his condition, compared to the benefits that proper positioning would provide throughout the remainder of the extrication. 3 When a crevasse is not wide enough to accommodate a horizontal supine position, placing a patient in a horizontal lateral decubitus position (eg, with the patient lying sideways) would be better than performing a raise in a vertical position. A method for transitioning a patient from a vertical position to a horizontal position is unlikely to be developed during an emergent event in harsh confined spaces. Rather, it could be developed and practiced during training in simulated or real crevasses (Figure 3).

Manikin demonstration showing a method to transition a hanging victim from a vertical to horizontal position, rotating in the frontal plane to be hanging on the side rather than supine; the facing wall has been removed for demonstration purposes, but the procedure can be performed in a realistic confined space. Initially, the rescue rope is attached via a self-contained haul system (in its shortened configuration) to the upper body. A second rope can then be attached via another haul system (in its extended configuration) to a sling around the legs (at mid-thigh to knee level). The upper body haul system can then be lowered, and the lower body haul system can be raised; these combined actions move the manikin from vertical to horizonal on its side.
The perceived need to extricate quickly also likely influenced the team to rush when bringing the victim over the crevasse edge. They simply grabbed him and quickly pulled him onto the snow surface. The presumed need for speed may have outweighed the risk of mechanical stimulation when roughly handling a cold patient. 3 Gentle extrication over the lip of the crevasse can also be practiced during rescue training (Figure 4).
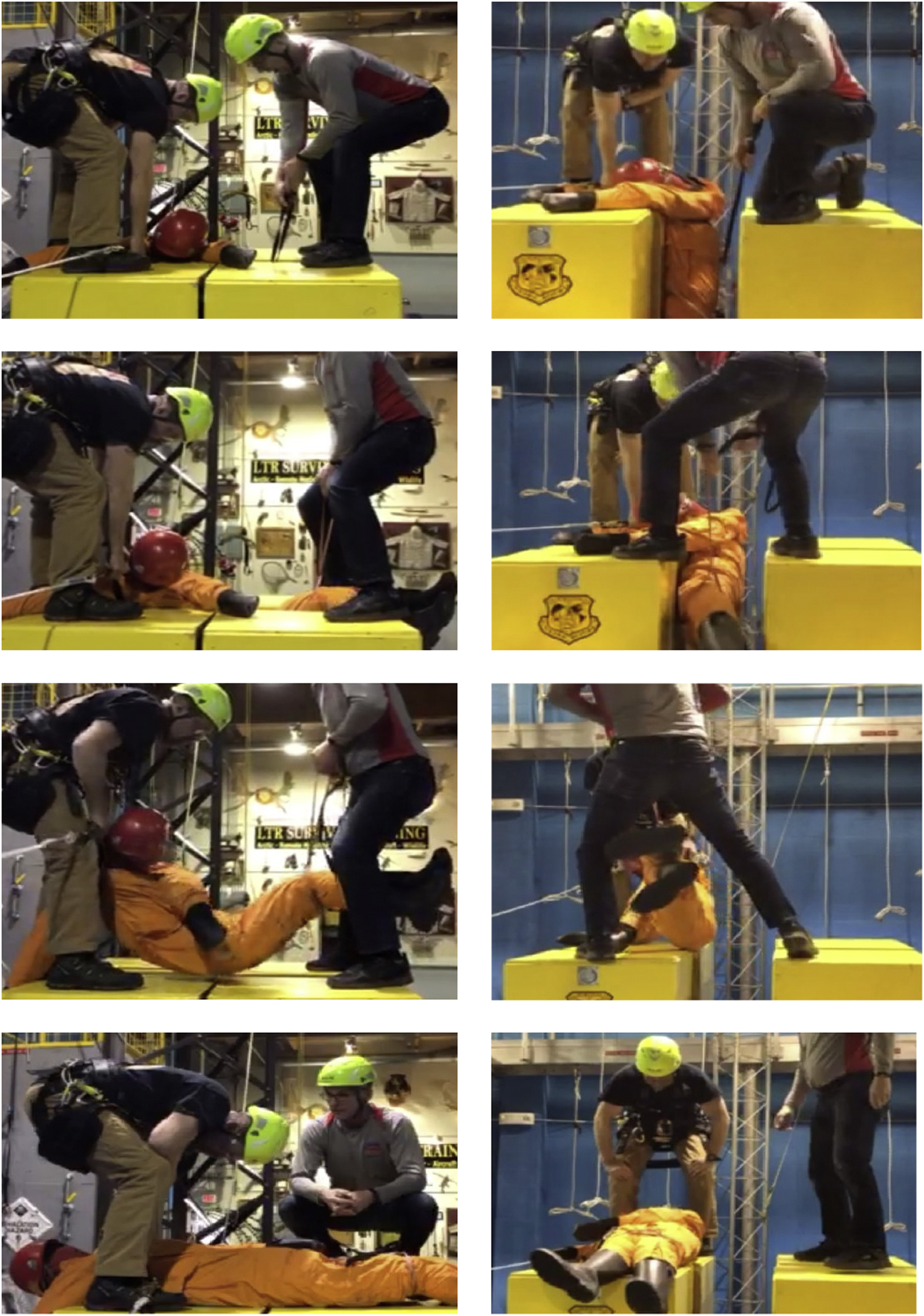
Perpendicular (left) and cross sectional (right) views of an extrication of a 75-kg manikin from a crevasse model (60 cm wide). If the victim must remain vertical while being raised to the ice surface, a sling or rope is placed around the legs between the mid-thigh and knee level. Both surface rescuers can then assume a straight back posture and slowly and gently lift the manikin out of the crevasse and gently place the victim gently on the surface. Top row of photos: attach sling/rope to the legs at the knees. Second row of photos: lift legs up to bring body to an approximate horizontal position. Third row of photos: lift victim slowly and gently up; rescuers may straddle the crevasse. Bottom row of photos: lay victim gently on the surface.
Recommendations
This case provides valuable observations concerning several aspects of rescue and medical operations in isolated areas such as Antarctica.
Worker Safety
Consideration should be given to designing high-insulation clothing ensembles that can be worn comfortably in a warm helicopter cockpit, where freedom of movement and dexterity are required.
Training
A base medical practitioner could be cross-trained in rescue techniques to the necessary competency to be included in a search and rescue (SAR) event in which it is reasonably expected that the victim will need advanced medical treatment.
All SAR personnel should be trained with the principle that the colder the patient is, the more care is required to perform an extrication that is as gentle and horizontal as possible. Realistic crevasse rescue training could include techniques for transitioning a victim from vertical to horizontal in both the supine position and on the side (for narrower spaces). Training should also emphasize that, even if a victim must be raised in a vertical position, a simple technique of using an additional sling or rope under the knees allows a simple, gentle, and horizontal extrication to the snow shelf. Realistic training could be conducted in a real or simulated crevasse, as demonstrated in Figure 4.
Training should also include awareness, causes, symptoms, and prevention of rescue collapse. Trainees should consider trying to prevent mental relaxation during rescue. 8 Rescuers could use positive, upbeat instructions like “I’ve got you, but you need to keep fighting with me. We’re going to get out of this together, keep fighting.” Although this practice has not been scientifically demonstrated to be effective, it is unlikely to produce any negative effects.
If a severely hypothermic victim with signs of life is wearing wet clothing and transport to advanced medical facilities is greater than 30 min, clothing should be cut off and removed before placing the victim in a hypothermia wrap, otherwise the victim may be packaged wet.3,9
Organizational Preparation for Rescue
A remote base and its SAR personnel should have ready-to-go kits (for personal, technical, and medical gear) in place and establish a standard operating procedure to immediately activate the rescue response as soon as a serious event is reported.
Equipment
A medical kit for potentially severe injuries with basic resuscitation equipment (including intubation supplies, bag-valve-mask, oxygen, and an automated external defibrillator) should always be loaded. If the patient is potentially hypothermic, a hypothermia rescue bag (or hooded sleeping bag) and a warming product that can be activated on site should be included (eg, chemical or electric heat pad or blanket). A mechanical chest compression device would be a valuable asset as patients have survived longer periods of CPR (6–9 h) than can be reasonably sustained by a single responder.10,11 This would not only provide continuous CPR but also allow a single caregiver to provide other care such as bag-valve-mask ventilation or warming. Consideration could also be given to including IV saline and a fluid warmer.
Rescue equipment for crevassed areas could include a tripod and winch and rescue harnesses for victims who may not be wearing them. Finally, a faster, larger helicopter would have permitted a more rapid response and carriage of medical personnel and medical equipment.
Conclusions
SAR personnel should be trained to avoid the perceived choice to move quickly or have the victim die. In fact, acting too quickly may worsen the victim’s condition. Rather, moving slowly and deliberately following the principles described for care of a cold patient will likely improve patient outcome, even if it takes a few minutes longer.
Footnotes
Acknowledgements
Acknowledgments: The authors thank Brian Horner for the use of “Learn to Return” facilities in Anchorage, Alaska, for assistance in developing and demonstrating rescue techniques shown in Figures 3 and ![]() .
.
Author Contributions: Both authors participated in report conception, case review, manuscript preparation, and revision. Both authors approved the final version.
Financial/Material Support: None.
Disclosures: None.