
Abstract
Introduction
We tested the hypothesis that individual susceptibility to freezing cold injury might be reflected in an attenuated cold-induced vasodilatation (CIVD) response by comparing the CIVD responses of an elite alpinist with a history of freezing cold injury in the feet (case alpinist) with those of an age- and ability- matched noninjured alpinists control group (controls). According to this hypothesis, the vasomotor responses to a CIVD test of the case alpinist would represent a pathophysiological response when compared with the normal physiological response of a noninjured cohort.
Methods
The case alpinist and the controls in the cohort group conducted a cold water immersion test comprising sequential immersion of a hand and foot for 5 min in 35°C water, followed by a 30-min immersion in 8°C water and a 10-min recovery period in room air. During this test we monitored the finger and toe skin temperatures.
Results
The case alpinist had a significantly attenuated CIVD response and a lower skin temperature in all injured and noninjured digits during immersion (∼2°C lower than in the control group) and an attenuated recovery of finger skin temperatures (∼6°C lower than in the control group).
Conclusions
The attenuated CIVD response of the case alpinist may reflect a previously unrecognized enhanced susceptibility to frostbite. In addition to the poor vasomotor response observed in the injured toes, he also exhibited a poor vasomotor response in his noninjured fingers. The results of the present study indicate that a test of vasomotor activity during thermal stress may identify individuals predisposed to cold injury.
Introduction
Freezing cold injury (FCI) is a common injury among explorers in cold regions.1,2 With the exception of military personnel, 3 workers, 4 and homeless people in cold areas, 5 frostbite currently occurs more often during leisure activities, with mountaineering being one of the most frequent.6,7 Epidemiological data demonstrate that FCI risk increases significantly with altitude 6 ,8,9 and general individual risk factors, such as pre-existing medical conditions (eg, Raynauds phenomenon), and behavioral factors, such as inappropriate protective clothing and inexperience. 10
Among the many factors contributing to frostbite incidence, genetic (individual) predisposition to cold injury is an important, 11 but the least investigated, factor. Despite a similar pattern of cold exposure in the members of an expedition (ie, same weather conditions, similar protective equipment), some members may experience FCI and others may not. The etiology of the individual variability in the incidence of FCI remains unresolved. 12 This variability or enhanced susceptibility to FCI might be reflected in an attenuated cold-induced vasodilatation (CIVD) response pattern to cold stress.13,14 CIVD is an acute increase in skin blood flow that develops mainly during cold exposure and is considered by some to be a cold protective mechanism, aimed at preventing cold injuries.14,15 It is suggested to be a locally and centrally mediated reaction of peripheral blood vessels, which may also play a role in heat loss during elevated body temperatures. 16
The present study compared the finger and toe skin temperature responses to a cold water immersion test in a 36-y-old elite alpinist (case alpinist) who experienced multiple FCIs to his toes during his climbing career with the responses observed in a cohort of ability- and age-matched alpinist controls who had never experienced FCI despite similar high altitude experience.
HYPOTHESIS
We tested the hypothesis that an individual with a history of digit FCIs may exhibit a predisposition to cold injury, which would likely be reflected in an attenuated digit vasomotor response to a cold stimulus, particularly when compared to an age- and experience-matched cohort of subjects. Confirmation of this hypothesis could warrant the development of a standardized cold stress test to identify individuals susceptible to FCI.
Methods
The study participants were all members of the Himalayan “Koroška 8000” expedition to Broad Peak (8051 m, Pakistan). The expedition leader was an experienced alpinist who frequently experienced FCI during his 14-year climbing career. These are presented in Figure 1 and Table 1.

Photograph of the case alpinist's feet indicating the FCI-amputated toes. The red dots represent placement sites for the skin temperature sensors.
History and characteristics of alpinist's cold injuries
RF, right foot; LF, left foot; ↓, partial length amputation of the digit.
The alpinist has never had any injury to his fingers.
With the exception of the Mount Everest expedition, after which amputations were required (partial amputations of 4 toes on the left foot and partial amputations of 2 toes on the right foot), injuries sustained on other expeditions did not result in any tissue loss. The remaining 5 participants in the study, and members of the same expedition, were all alpinists with experience in climbing peaks >8000 m. All 6 members of the expedition underwent a cold water immersion test before departure to Broad Peak. At the time of testing they were all actively climbing at high altitude (>4000 m) environments and participating in seasonal expeditions. Five alpinists successfully summited and descended to base camp. The expedition leader was the only previously frostbitten alpinist on the team. He reached 7000 m during the acclimatization procedure. On the summit push day, instead of continuing to the summit, he accompanied an exhausted team member from an altitude of 6600 m to base camp. He did not sustain any frostbite on this expedition.
Written informed consent was obtained from the participants before participation in the study. Alpinists (age: 38±6 y, height: 180±4 cm, weight: 79.4±5.4 kg) were requested to refrain from consuming alcohol or caffeine or engaging in physical activity on testing day. All tests were performed in a climate-controlled room maintained at 21°C with 52% relative humidity during the northern hemisphere spring (mid-June 2012) at the Olympic Sport Centre Planica (Rateče, Slovenia). The study was approved by the Ministry of Health of the Republic of Slovenia (National Committee for Medical Ethics) in accordance with the Declaration of Helsinki.
COLD WATER IMMERSION TEST PROTOCOL
The cold water immersion test was used to determine digit skin temperature responses before, during, and after the sequential immersion of a hand and foot in cold water. Participants were seated in a semirecumbent position for the duration of the test. They were dressed in a T-shirt and shorts, with shoes and socks removed. The subjects were instrumented with T-type thermocouples placed on the dorsal surface of 1 hand or foot and at the nail beds of the fingers and toes. The nail bed site was chosen rather than the finger pad because it provides better reproducibility of skin temperature responses during CIVD. 17 In injured digits (left foot of the injured alpinist), the thermocouples were placed on the dorsal and most distal part of the digits.12,18
On amputated digits, the skin temperature of the most distal part of the stump was used. The thermocouples were connected to a data acquisition system (Almemo, 5990-2; Ahlborn, Holzkirchen, Germany), which recorded values at 10-s intervals. Following a 5-min baseline period, participants placed their hand or foot in a thin plastic bag (to avoid wetting the skin) and immersed it in a water bath, first for 5 min at 35°C to normalize digit temperature (prewarming phase) and then for 30 min in 8°C water (cold water immersion phase). The temperature of the water was maintained with a cooling system (Alfa Laval, Stockholm, Sweden). After 30 min had elapsed, the hand or foot was removed from the water and allowed to passively warm in room air (∼21°C) for 10 min (spontaneous rewarming phase).
STATISTICAL ANALYSIS
Data in the tables are presented as median values (with interquartile ranges). The difference between digit skin temperatures of the alpinist vs the controls was tested with a Mann-Whitney test. The temporal response of digit skin temperature was integrated to obtain the area under the curve (AUC; arbitrary units) and was defined as the incremental AUC above 5°C and calculated from 10 to 30 min of cold water immersion because the first 10 min were deemed to be a transitional phase during which digit skin temperatures were decreasing rapidly. The P values were adjusted using the Benjamini–Hochberg method to limit the false discovery rate at 5%. 19 An adjusted P value of less than 5% was considered significant. The analysis was performed with the web-based R software (version 3.4.1) for statistical computing. 20
Results
FINGER RESPONSES TO COLD
The case alpinist had significantly lower minimum (Tmin) and average (Tavg) finger skin temperatures during the cold water immersion (COLD) and spontaneous rewarming (POST) phases of the test than the control group (COLD Tmin=7.6 [case alpinist] vs 9.6°C [control alpinists], P=0.0014; COLD Tavg=9.2 [case alpinist] vs 11.2°C [controls]; P=0.0001; POST Tavg=15.1 [case alpinist] vs 20.6°C [controls]; P=0.0014). The number of CIVD waves was significantly lower in the case alpinist than in the controls (0 vs 2, P=0.0486). CIVD waves were present only in the middle finger (5 waves) of the case alpinist. His AUC was also significantly lower (55.2 [case alpinist] vs 130.4 [controls], P=0.0001; Table 2).
Temperature responses of fingers in control group of alpinists and the case study alpinist
PRE Tavg, average skin temperature in the prewarming phase; COLD Tmin, average minimal skin temperature during cold water immersion phase; COLD Tavg, average skin temperature during cold water immersion phase; RoC-slope, rate of cooling; POST Tmax, average maximal skin temperature during spontaneous rewarming phase; POST Tavg, average skin temperature during spontaneous rewarming phase; RoR-slope, rate of recovery; No. of waves, number of CIVD waves; AUC, area under the curve (a.u.=arbitrary units).
Bold values reflect statistical significance (P<0.05).
TOE RESPONSES TO COLD
Similar to the fingers, the case alpinist had significantly lower minimum and average skin temperatures of the amputated toes during cold water immersion compared to the control group. (COLD Tmin=5.9 [case alpinist] vs 7.8°C [controls], P=0.0014; COLD Tavg 7.8 [FCI alpinist] vs 10.6°C [controls], P=0.0007). Statistical comparison of the number of CIVD waves in toes was not performed because no CIVD waves occurred in the toes of the FCI alpinist. He had higher rates of recovery of toe skin temperature (RoR-slope) compared to controls (RoR-slope=1.21 [case alpinist] vs 0.69°C·min−1 [controls], P=0.0202). The AUC was also significantly smaller than in the control group (35.4 [case alpinist] vs 112.7 [controls], P=0.0003) (Table 3). Results are depicted in Figures 2 and 3.
Temperature responses of toes in control group of alpinists and the case alpinist
PRE Tavg, average skin temperature in the prewarming phase; COLD Tmin, average minimal skin temperature during cold water immersion phase; COLD Tavg, average skin temperature during cold water immersion phase; RoC-slope, rate of cooling; POST Tmax, average maximal skin temperature during spontaneous rewarming phase; POST Tavg, average skin temperature during spontaneous rewarming phase; RoR-slope, rate of recovery; AUC, area under the curve (a.u.=arbitrary units).
Bold values reflect statistical significance (P<0.05).
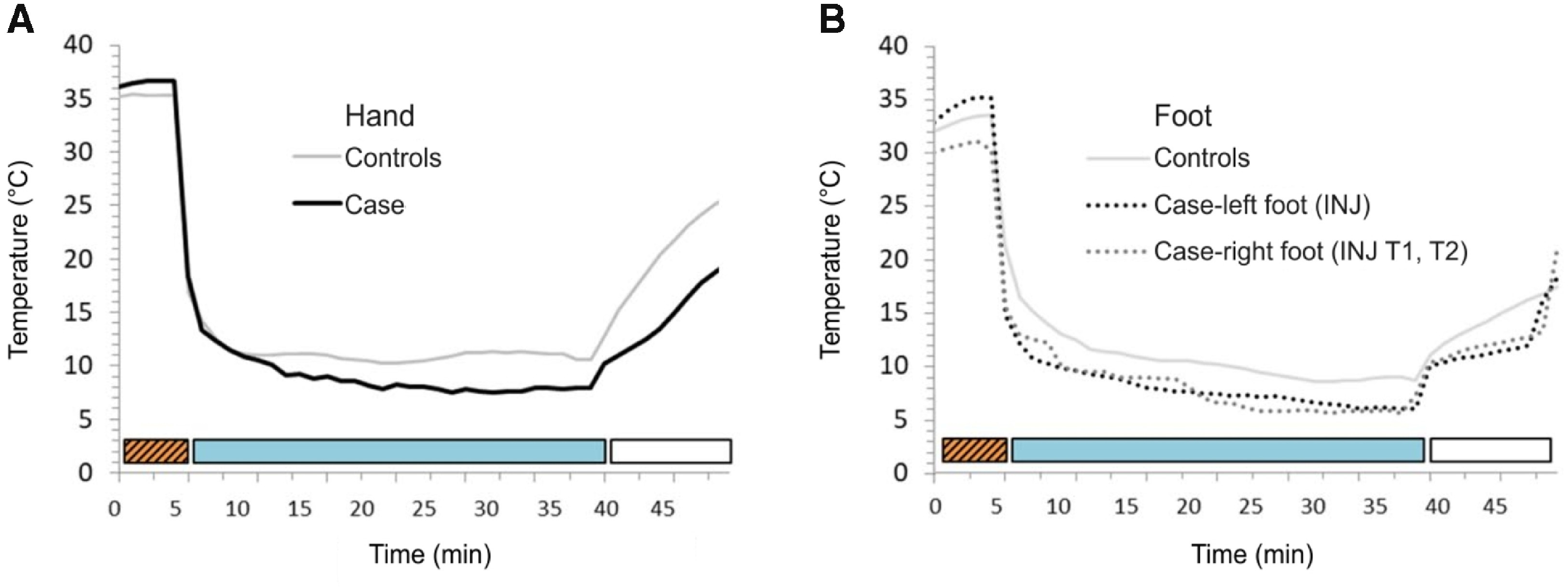
Finger (A) and toe (B) skin temperature (Tsk) responses during the cold stress test. The Tsk of the noninjured control subjects (gray line in A and B) are higher than that observed in the fingers (solid black line in A) and toes (left foot: black dotted line; right foot: gray dotted line; B) of the case study alpinist. The prewarming phase of the test is designated with a hatched box, the cold water immersion phase with a blue box, and the passive rewarming phase with an open box. The case study alpinist experienced freezing cold injuries requiring partial digit amputations (INJ) to 4 toes on his left foot and 2 toes on his right foot. Despite these injuries to the toes, it is his finger responses that are also significantly lower than the mean responses of the control group (A). SD bars of the control group are omitted for the purpose of clarity.
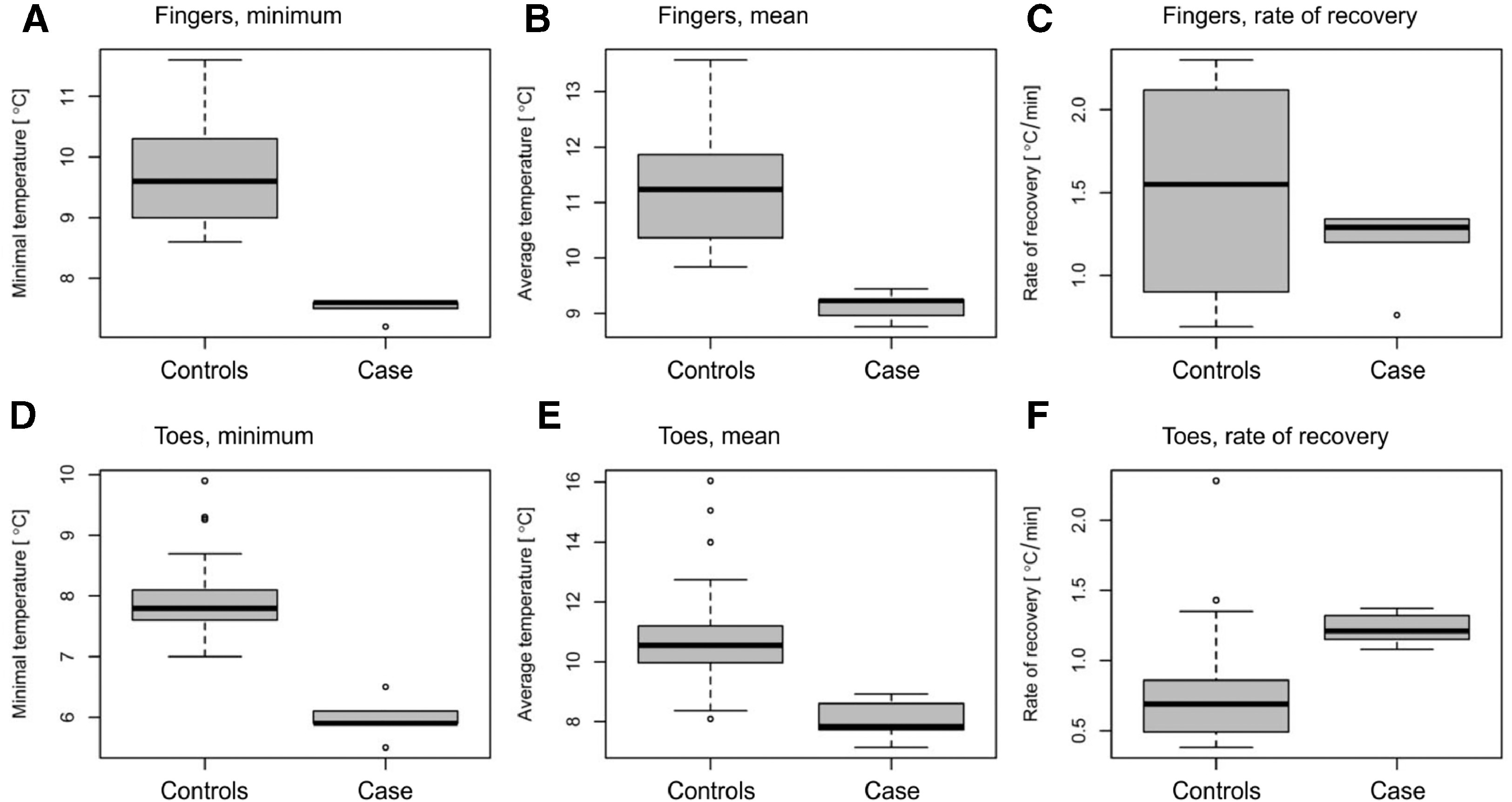
Box plot for median and interquartile ranges of the control group of 5 alpinists compared with the case study alpinist; A to C represent the fingers and D to F the toes; A,D—minimal temperature during cold phase; B,E—average temperature during cold phase; C,F—rate of recovery. The boxplot depicts median, interquartile range (25 and 75 percentiles by box, + and 1 1.5 IQR with bars), and outliers beyond bars.
Discussion
Vasomotor responses during the cold water immersion test should be examined from the perspective of different phases of the experimental protocol. The cold-induced vasoconstriction (decreasing Tsk) during the cold water immersion phase and heat-induced vasodilatation during the spontaneous rewarming phase (increasing Tsk) are responses initiated by changes in skin temperature, whereas in the part of the immersion phase during which skin temperature is constant, vasodilatation (CIVD) occurs in the presence of a constant cold stimulus. Thus, the mechanisms governing the vasomotor responses to cooling and rewarming are most likely different from those governing vasodilatation during a constant cold stimulus (CIVD). Because an attenuated vasodilatation (CIVD) response in the case alpinist was observed in both the uninjured fingers and the freezing cold injured toes, the attenuated CIVD in the toes was most likely also present before the injury. This would suggest that the attenuated CIVD response reflects a previously undiagnosed predisposition to cold injury, 14 whereas any enhanced vasomotor reactivity (ie, during the cooling and spontaneous rewarming phases) could represent a sequela of the FCI. The focus of the discussion will be the possibility that the attenuated CIVD observed in the case alpinist represents a predisposition to FCI.
MEASUREMENT OF DIGIT SKIN BLOOD FLOW
Essential to the interpretation of the observed digit skin temperature responses during the cold water immersion test is that they represent the response of skin blood flow. Measurement of peripheral blood flow can be achieved with a variety of methodologies (eg, ultrasound, plethysmography, near infrared spectroscopy), most of which are not ideally suited for field use and some of which do not provide a good measure of skin perfusion. In the present study we used the measurement of digit skin temperature, which reflects peripheral blood flow.21,22 Skin temperature has been shown to be well correlated with skin blood flow in the cold, 15 although it lags skin blood flow by an average of 112±72 s. 23 In our study we used a standardized protocol for CIVD to ensure good reproducibility of the results.17,24
FREEZING COLD INJURY (FROSTBITE)
FCI is classified as deep (most often resulting in tissue loss—ie, amputations) or superficial (most often with no visible sequelae). FCI sequelae are well documented25,26 and resemble those observed in patients after non–freezing cold injured tissue. 27 The majority of frostbitten patients demonstrate hypersensitivity to cold (53%), numbness of fingers (40%), and reduced sensitivity to touch (33%). 28 Surviving tissue after FCI may exhibit increased tendency for vasospasms, which may pose a greater frostbite risk. 28 In a study using cold air provocation, skin temperature of injured digits decreased more rapidly and reached lower values during cold exposure compared to noninjured digits, which was interpreted as a risk of further cold injury in the injured digits. 29 It has also been suggested that frostnip (a type of non-FCI) may result in sequelae and indicate a predisposition to frostbite. 30
TOE RESPONSES
In contrast to the control group, the case alpinist exhibited no CIVD responses in his toes. This lack of a CIVD response could have been present before the occurrence of any cold injury in his toes or it may reflect a consequence of a previous cold injury, one which also resulted in amputations of some toes. We have previously reported similar attenuation of CIVD responses in the FCI digits of alpinists when compared to the CIVD responses of a control group of alpinists who have never experienced FCI. 12 In this previous study 12 we were also able to compare the injured digit skin temperatures with the digit skin temperature response of the noninjured digits on the contralateral side of the FCI alpinists. During the cold water immersion test in this previous study, 12 the average toe skin temperature was 13% (n=26, P<0.001) lower (1.5°C) than the toe skin temperature of the corresponding noninjured digits on the contralateral side. We also observed that the injured toes cooled faster than their noninjured counterparts (n=26, P<0.001); a faster cooling was observed in all the toes of the injured limb compared with the toes of the noninjured limb (n=40, P<0.001). 12 CIVD in toes is less expressed than in fingers, and in general, toe skin temperatures are lower than finger skin temperatures, 12 ,31,32 which may contribute to the greater prevalence of FCI in toes compared with fingers.
It has been suggested 33 –35 that in addition to the rate of skin cooling observed during the cold water immersion test, the capability of the digits to spontaneously rewarm after the cold water immersion test also plays an important role in estimating resistance to cold injury. The results of the case alpinist in the present study do not support this suggestion because he had a higher rate of recovery of toe skin temperature compared with controls. We reported a similar response in the skin temperature of toes that had previously sustained FCI compared with uninjured toes. 12 The faster cooling and rewarming rates in toes could be a sign of enhanced vasoreactivity of injured areas to the different thermal stimuli, rather than a sign of greater tissue protection. 36 In contrast to the toes, the fingers of the case alpinist did not rewarm faster than the fingers of the control group. In contrast to previous studies, 33 –35 the subjects of the present study were all experienced alpinists. The digit skin temperature responses observed in the case alpinist were obtained on FCI-amputated digit stumps and thus may be a consequence of the severe FCI. Such severe injuries were not present in the subjects of the previous studies.
FINGER RESPONSES
The case alpinist never sustained frostbite in his fingers. Nevertheless, he had significantly lower finger skin temperature values compared with the other alpinists during the cold water immersion test (∼2°C, significantly less CIVD waves and slower recovery during spontaneous rewarming). Protection of fingers is largely behavioral and easier to perform even in extreme conditions compared with toes (eg, changing wet footwear in extreme cold is difficult). 18 ,28,37 In many situations during his climbing career, the case alpinist avoided frostbite of the hands as a result of behavioral actions. Additionally, the frequency of CIVD in fingers is usually higher than in toes (both in terms of frequency and amplitudes), which results in higher overall Tsk compared with toes. 34 The lower finger skin temperatures of the case alpinist may, to a degree, also be a result of the fact that he exhibited fewer CIVD responses in the fingers and toes compared with the control alpinists. The case alpinist had colder hands than the control group, which suggests that he is among those individuals who may always be more prone to cold injury, yet his susceptibility had never been recognized or assessed in any systematic manner. However, the rewarming rates of fingers were not different from those of the control group.
FROSTBITE RISK AFTER PREVIOUS COLD INJURY: A CAUSE OR A CONSEQUENCE OF PRE-EXISTING INDIVIDUAL SUSCEPTIBILITY?
Many nonthermal factors are known to affect the response of the peripheral circulation (eg, diabetes, Raynauds phenomenon, past frostbite) to cold stress and may thus contribute to the increased predisposition of such patients to cold injury.11,38 Of the thermal factors that may reduce the risk of cold injury, it has been suggested that repeated daily exposure of the digits to cold may improve peripheral circulation and thus act as a protective mechanism.39,40 Alpinists, who spend a lot of time in a cold environment may, as a result of cold acclimatization, attenuate any predisposition to cold injury.35,41 In addition, repeated cold exposures result in a reduction in cold sensation, discomfort and pain. 42
Our study provides evidence that impaired toe Tsk during a cold water immersion test may be a consequence of either past FCI 25 ,28,43 or a pre-existing enhanced susceptibility to cold.14,44 According to our data of lower Tsk in the toes, either or both mechanisms (individual susceptibility and preinjured tissue) may be clinically relevant and contribute to increased risk of future cold injury in an alpinist. Identification of individuals predisposed to cold injury would be of practical benefit before departure on expeditions during which cold exposure cannot be avoided.
INDIVIDUAL SUSCEPTIBILITY TO FROSTBITE—RISK INDEX FOR FROSTBITE
A risk index for frostbite 44 was proposed as a method of defining individual susceptibility to cold injury, suggesting that cold-intolerant individuals with lower finger skin temperatures before cold exposure had an enhanced risk for FCI. In a recent study it was further suggested that the overall risk of FCI could be determined from the CIVD response of 1 finger. 14 Individuals with a weaker finger CIVD response before cold injury were defined as being at greater risk of FCI. In this study of 179 soldiers participating in a winter training course, 11 sustained deep frostbite, of which 22% were prospectively identified as being more susceptible to frostbite and 3% as being low in FCI susceptibility. Common to both studies was the assumption that susceptibility to FCI of all digits of the feet and hands may be determined on the basis of a CIVD test conducted on 1 finger. Such generalization of the results of the CIVD response of 1 finger to the CIVD responses of other digits has been demonstrated to be unwarranted. 31
Because our analysis included a single injured alpinist, the results are not necessarily representative of the responses of cold-injured individuals in general. However, because other studies on nonalpinist populations confirm the existence of frostbite risk,14,44 we believe that the CIVD response may be a potential predictor of frostbite risk also for the alpinist population.
Because frostbite amputations of the case alpinist were of his toes and we observed attenuated skin temperature responses also in the uninjured fingers, this could be interpreted as evidence of a greater susceptibility or predisposition to cold injury rather than a consequence of any cold injury per se considering the fingers never sustained cold injury.
Individual variability in tissue volume and surface area-to-mass ratio may also contribute to the individual susceptibility to FCI. Namely, a greater mass will be capable of storing more heat, but a greater surface area will provide a greater area for heat loss. The results of a study 45 comparing foot volumes of a group of alpinists who had experienced frostbite and had amputated toes with a group of noninjured alpinists and a control group found no significant difference in foot volumes among the 3 groups, although some of the frostbitten alpinists had as many as 3 amputated toes. In such a population, foot volume is therefore a factor unlikely to contribute significantly to FCI. Tissue volume may become a significant factor in cases of multiple digit or hand/foot amputations.
Finger morphology might contribute to individual susceptibility to FCI. Namely, populations indigenous to the North Polar regions have been shown to have shorter and thicker fingers.46,47 As a consequence, the surface area for heat exchange is reduced. 48 By analogy, stumps are sometimes extremely short and may mimic the heat-loss effect of short and thick digits. Despite the reduction of surface area, the uninjured short and thick fingers are able to lose more heat to the environment when exposed to severe cold. 15 The reason is most likely functional and may be explained by the location of arteriovenous anastomoses.49,50 A greater heat loss would result in higher skin temperatures and in a reduced risk of FCI.
LIMITATIONS AND PRACTICAL IMPLICATIONS
The main limitation of the present study is the low number of subjects: The response of 1 case alpinist was compared to the responses of the noninjured alpinists. Although the comparison of the CIVD response between the case alpinist and control group yielded statistical significance, the physiological relevance of the difference, particularly in assigning the case alpinist's response as reflecting a predisposition to FCI, remains to be resolved. Without doubt, the FCI sustained by the case alpinist to his feet during his 14-y career can be termed severe. Despite the recorded evidence of his injuries, whether these were sustained because of a predisposition to FCI at the onset of his career or were the cumulative sequelae of his injuries over the course of his 14-y career cannot be resolved on the basis of his toe CIVD response. However, the case alpinist never sustained any FCI to his hands. The reason for that may partly be due to behavioral mechanisms; FCI of the fingers is more easily preventable in harsh high altitude environments than FCI of the feet (eg, heating, changes of gloves/mittens). Despite this, the finger CIVD response was significantly lower than that of the noninjured alpinists. This would support the notion that the attenuated finger CIVD response reflects a predisposition evident in the sequelae of the previous FCI sustained in the toes. It may be plausible to consider deriving a nomogram based on the responses of noninjured digits to a cold exposure, with the purpose of identifying individuals with attenuated responses. Inclusion of the results of a population with previous FCI would provide a range of responses, from normal to inappropriate, thus providing feedback regarding the predisposition of individuals to FCI.
The present study included few participants. Similar comparison of a greater number of alpinists after FCI with control alpinists could be considered a prelude to the development of an FCI risk index based on the characteristics of the CIVD response. The results lend support to the notion that a set of nomograms could be constructed that would allow cold-intolerant individuals to be identified on the basis of a simple cold water immersion test. Because a similar test has been established for the diagnosis of nonFCI, 51 it would seem worthwhile to pursue the development of a test of FCI susceptibility/risk.
Conclusions
Based on the comparison of the results of the cold water immersion tests, the present single-case data speak in favor of the hypothesis and indicate that the case alpinist had a significantly attenuated digit skin temperature response to cold water immersion, reflecting an attenuated digit skin perfusion, compared to the cohort of uninjured alpinists. Whether this is indicative of a general predisposition to cold injury cannot be concluded unequivocally.
Footnotes
Acknowledgements
Acknowledgments: The authors are thankful to the dedicated alpinists who generously took part in this study.
Author Contributions: Conception and design of the work (JG, IBM); performed frostbite treatment in the alpinist in the past (PJM, IBM, JG), contributed to data acquisition (SAM, ACM); contributed to the analysis and interpretation of the work (JG, SAM, ACM, RB, IBM); drafted the manuscript (JG, IBM); revised manuscript critically (JG, SAM, ACM, PJM, RB, IBM); approved the final submitted manuscript (JG, SAM, ACM, PJM, RB, IBM).
Financial/Material Support: None.
Disclosures: None.