
Abstract
A 47-y-old man was bitten by a reduviid bug from the Zelus Fabricius, 1803 genus, which was hidden inside a rubber-coated boot. The bite caused immediate and sharp pain, followed by local edema and constant pruritus for 15 d. Pain and fever within the first 24 h were managed with analgesics as needed, and resolution was complete and without sequelae after 21 d.
Introduction
Known as “bugs,” “kissing bugs,” or “assassin bugs,” insects from the Reduviidae family, one of the most numerous in the order Hemiptera, which includes about 7000 species, 1 –3 may have phytophagous, hematophagous, or predatory habits. Reduviidae can be distinguished from other bug families by their elongated head with a transverse groove behind the compound eyes and the short, prominent, segmented rostrum projecting outward from the head. A characteristic of the family is that the tip of the rostrum, in repose, fits into that groove. 4
The evolutionary aspects related to the different purposes of use of toxins in Hemiptera—phytophagia, predation, or defense—has resulted in a great variation of salivary gland secretions in these insects. As a consequence, there may be variation in the clinical effects of these toxins in vertebrate or invertebrate animals.5,6 Bites from hematophagous species are usually painless, but inoculated saliva can trigger allergic reactions of varying degrees. The intense pruritus resulting from these reactions may result in lesions that promote conditions for active trypomastigote penetration or indirect penetration as a result of local itching and subsequent scratching; serious diseases sometimes are established, such as Chagas disease.3,7–9 Although they do not transmit diseases, predatory reduviid bugs can also bite in a defensive manner, resulting in marked pain and local skin reactions that may last up to 6 mo, especially in allergic patients.5,7
There are limited reports of incidents caused by nonhematophagous Reduviidae insects in humans. The aim of this study was to report a bite caused by a Zelus spp (Hemiptera; Heteroptera: Reduviidae) and the clinical evolution of the intense erythematous local reaction associated with the bite.
Case Report
The case occurred in the Cerrado (Brazilian savannah)-Pantanal ecotone in the central-west region of Brazil, in the state of Mato Grosso (S 13°36.309’ W 054°52.913’; 501 m above sea level), at the end of the rainy season (May). A 47-y-old man was bitten while putting on a rubber-coated boot. The pair of boots had been left in the back part of a pickup truck, which was parked near a forest of eucalyptus trees. He felt an immediate and sharp pain on the dorsal surface of his right foot and found the insect partially crushed inside the boot (Figure 1). The insect fragments were collected, preserved in a bottle containing 70% alcohol solution, and sent to the Entomology Section of the Zoological Collection of the Federal University of Mato Grosso, Cuiabá, Brazil, for identification and deposit. The specimen was identified as Zelus spp, a reduviid.
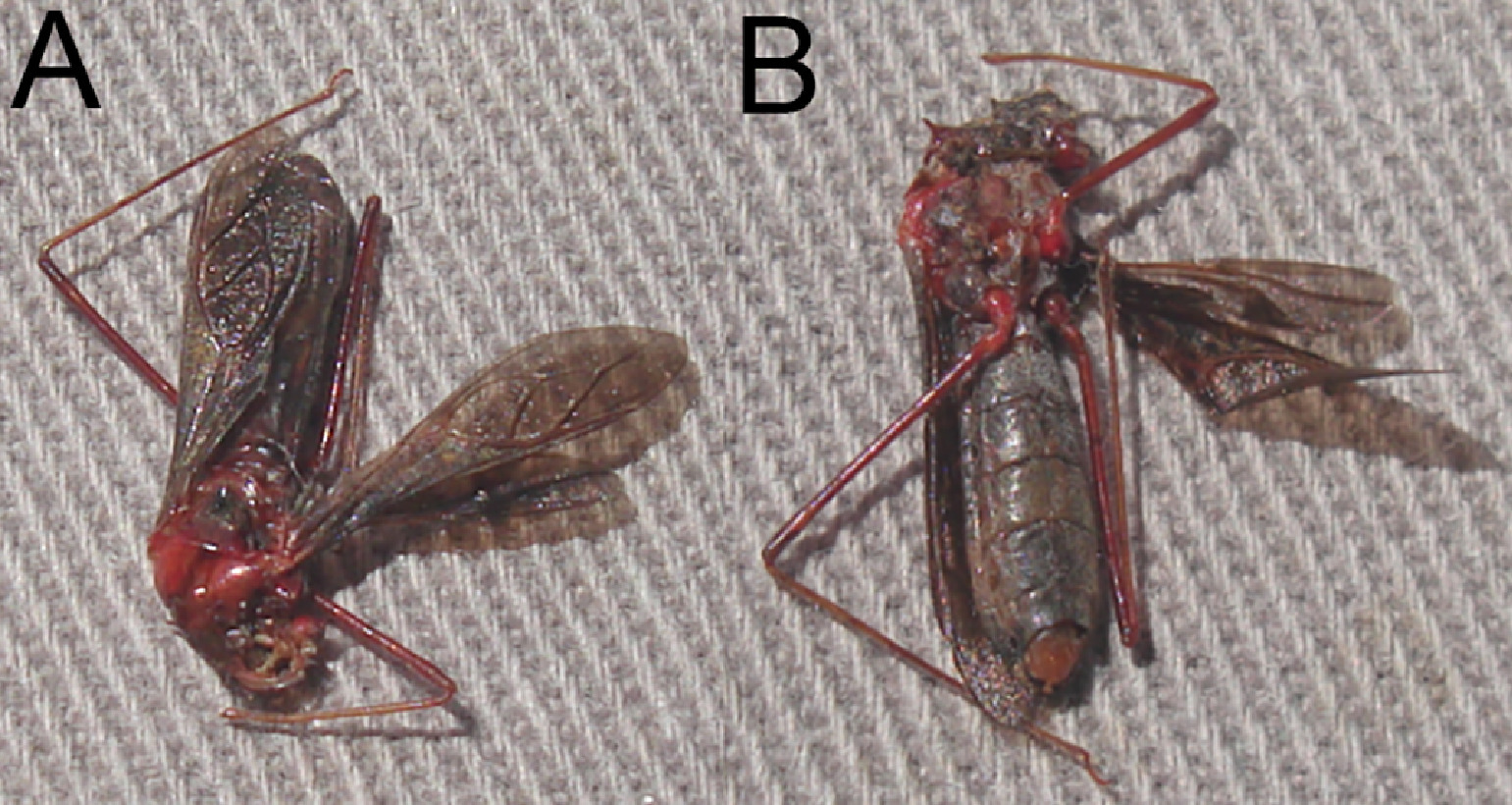
Zelus spp approximately 15 mm in length. The insect was hidden inside a boot and attacked when it was partially crushed, biting the dorsal area of the patient's foot.
After the bite, there was intense pain and marked edema, with formation of an elliptical-shaped erythematous plaque measuring 6 × 4 cm with the presence of small vesicles. Between 6 and 24 h after the bite, the patient experienced paresthesia, desensitization, and marked edema of the toes; it was not possible to completely flex them. Lymphadenopathy was not observed, but mild fever occurred in the first 24 h. Pain and fever were managed with dipyrone (an NSAID) as needed. The plaque persisted for 7 d and was marked by intense and constant pruritus followed by centrifugal regression and desquamation (Figure 2). After 15 d, the inoculation area underwent infiltration and subsequent detachment. Pruritus was constant and intense throughout the process, but resolution was complete and without sequelae after 21 d.

Clinical signs associated with the bite of Zelus spp. A, Immediate cutaneous reaction with formation of elliptical local erythema and diffuse edema around the bite on the dorsal surface of the right foot. B, Close view of the bite region showing erythema and formation of strophulus prurigo within the first 3 h. C, Improvement of the erythema 7 d after the incident but with the remaining presence of a hardened core. D, Discreet erythema and skin scaling at d 15. Arrow indicates the exact location of the bite.
Discussion
Zelus is endemic to and widely distributed throughout the Americas, ranging from southern Canada through central Argentina. This genus has been investigated and studied as natural predators of pests in cotton, corn, soybean, and alfalfa crops and in fruit trees. 2 The case here described occurred near a forest of eucalyptus trees. Despite shaking the boots vigorously before wearing them, the insect was not ejected, probably because of the presence of raptorial forelegs and/or adhesive pads. 10 Accidental cases involving hemipteran bites are sporadic and occur in a defensive context when these insects are predated or compressed, 10 –12 as occurred in this report. Nonetheless, hemipterans are natural insect predators that feed on the sap of plants but also are used for biological control of pests that parasitize plantations, 4 increasing the chance for incidents with humans.
Many of the reactions described after contact with hemipterans are related to the effects of toxins present in their saliva, with different clinical manifestations.5,8,10 Predatory insects require toxic saliva that can rapidly paralyze invertebrate prey and liquefy its tissues, whereas blood-sucking insects need a more benign saliva that will not stimulate adverse reactions from a vertebrate host. 6 Thus, a predatory reduviid, such as the one in this report, usually inflicts a very painful bite in humans, sometimes causing allergic reactions or infection. Characteristics of the victims, such as allergic tendency and weight, can also contribute to the severity of symptoms. In the present report, pathophysiological aspects and clinical evolution of the patient were similar to those described in incidents with Hemiptera and its variety of species. 11 –14 Numbness and tingling sensations in regions close to the bite, such as toes, extending to the ipsilateral limb may be related to the possible presence of neurotoxins in the saliva of the predator. In reviewing the pharmacological effects of the saliva of these insects, it has been argued that the immediate paralyzing effects seen in smaller vertebrates corroborates the hypothesis of the presence of currently unidentified neurotoxins. 7 There is compelling evidence that predatory bugs can inject not only digestive enzymes but also neurotoxins and other pharmacological modulators that are responsible for the extreme pain of the bite. The presence of these compounds may explain the variability, severity, and persistence of signs among bug-bitten patients.7,15
Local management of the bite includes appropriate washing and disinfection and application of an ice pack. Steroid creams or oral antihistamines may help reduce swelling or itching, and nonsteroidal anti-inflammatory drugs can be used for pain relief.13,16 Importantly, medical attention should be sought immediately if there is any sign of anaphylactic reaction, such as generalized swelling, itching, hives, or difficulty breathing. 17
Despite the severity of Reduviidae bug bites, the resolution in this case was complete, without the need of pharmaceutical intervention, except use of a systemic analgesic (dipyrone). It is advisable to carefully examine any stored articles of clothing or shoes in locations where these insects occur because if a concealed reduviid is contacted by an unsuspecting human while donning these, the bug may inflict a significant bite in self-defence.
Footnotes
Acknowledgments
The authors thank José Mario d'Almeida and Fernando Zagury Vaz-de-Mello for the insect identification and deposit at Coordena¸ão de Educa¸ão Mediada por Tecnologias da Informa¸ão e Comunica¸ão (CEMT)/Universidade Federal do Mato Grosso (UFMT). The authors also thank Luciano Barros and Vidal Haddad Junior for critical review of the article.
Author Contributions: Patient of the case (CEPS), manuscript drafting (CEPS, JRS, RAZ, FJS, CS), manuscript reviewing and formatting (CEPS, RAZ).
Financial/Material Support: None.
Disclosures: None.