
Abstract
Introduction
Apostle Islands National Lakeshore (APIS) lies at the northern tip of Wisconsin and is home to a network of 21 islands along Lake Superior. The goal of this report is to investigate search and rescue (SAR) and emergency medical services (EMS) trends at APIS in an effort to improve visitor safety and resource allocation.
Methods
This study is a retrospective analysis reviewing APIS SAR reports and annual EMS summary reports from January 1, 2006, to December 31, 2015. Information related to incident type, incident date, individual demographic characteristics and activities, injury/illness type, cost, and contributing factors were recorded and analyzed in frequency tables.
Results
From 2006 to 2015, APIS SAR conducted 133 total missions assisting 261 individuals—200 not injured/ill, 57 injured/ill, and 4 fatalities. Median cost per SAR incident involving aircraft totaled $21,695 (range: $2,993–141,849), whereas incidents not involving aircraft had a median cost of $363 (range: $35–8,830). Nonmotorized boating was the most common activity resulting in SAR incidents. All 4 fatalities were attributed to drowning while kayaking or swimming. Cold-related injury/illness accounted for nearly half of all injuries/illnesses (45%) with the most commonly reported contributing factor being high winds. EMS responded to a total of 134 incidents. Trauma and first aid accounted for 43% and 34% of EMS workload, respectively.
Conclusions
Overall, this study highlights the hazards associated with the frigid and rough conditions of Lake Superior. The reported results aim to help APIS personnel more saliently convey risks to visitors and plan appropriately in an effort to decrease the need for future rescues.
Keywords
Introduction
Apostle Islands National Lakeshore (APIS), established in 1970, lies along the remote shores of Lake Superior at the northern tip of Wisconsin. The Apostle Islands archipelago consists of 22 coastal islands (21 within park boundaries), spanning 28,076 hectares (69,377 acres) of diverse sandscapes, cliffs, and sea caves. 1 From 2006 to 2015, this small Midwestern park, operated by the National Park Service (NPS), received an average of 187,220 annual visitors. 2 During the warmer months, recreation at APIS is largely water based, involving motorized and nonmotorized boating, or backcountry hiking. In the wintertime, recreation involves backcountry hiking, often to explore APIS's ice caves.
Outdoor recreation has become increasingly popular, a trend reflected in national park visitation rates from 2014 to 2016, in which the NPS experienced 3 consecutive years of record visitation rates, surpassing 325 million visits in 2016. 3 –6 With this increase in interest and the natural hazards associated with wilderness recreation, national parks must operate fully functional emergency medical services (EMS) systems equipped to respond to a variety of emergency situations, often in rugged terrain and harsh conditions.
When discussing EMS response in wilderness recreation areas, EMS incidents can be further categorized into EMS and search and rescue (SAR) incidents. EMS incidents are rescue operations conducted in frontcountry regions, defined as areas accessible by automobile. 7 –9 SAR incidents are emergency operations initiated to render aid to individuals believed to be in distress, injured, ill, and/or lost in backcountry areas, which are defined as being inaccessible by automobile. 7 –9 The current APIS EMS system involves a frontcountry EMS response team and a multidisciplinary backcountry SAR system composed of park rangers and other APIS staff with EMT basic training.
National park EMS operations are critical to ensuring visitor safety but are costly, highlighting the importance of identifying and monitoring trends in an effort to improve both outcomes and resource allocation. Recognizing the significance of such analysis, a growing body of literature has investigated injury/illness trends in various wilderness recreation areas.5,7–26 However, the majority of these studies have focused on larger parks, mostly located in the western United States, with very little research focused on the Midwestern region and no previous analysis of recreation areas with a majority of water-based recreation. This study aims to contribute a novel perspective to the current literature: a retrospective analysis of EMS operations at APIS, a previously uninvestigated small Midwestern park with largely water-based recreation. As a remote park with limited funding, trend analysis is important because it can help provide APIS personnel with information targeted toward the reduction of future rescues. Thus, ultimately, the goal of this study is to equip APIS personnel with knowledge of SAR and EMS event trends in an effort to more saliently portray risks to visitors, reduce the need for future rescues, and most effectively apportion resources.
Methods
This study is a retrospective analysis that aims to identify trends associated with emergency events requiring activation of the APIS SAR and EMS systems between January 1, 2006, and December 31, 2015. The time frame was selected based on record availability. This study was granted exemption approval by the Rush University Medical Center institutional review board. APIS personnel deidentified all SAR and EMS incident reports. Rush University personnel conducted data extraction and analysis. SAR incident inclusion criteria required that 1) the incident resulted in production of an NPS SAR report form (10-16-2003, version 2.2); and 2) the report narrative specified that APIS staff responded to an event. The inclusion criteria resulted in 133 SAR reports. For each report, type of incident (injury/illness vs non–injury/illness), demographic information, subject affiliation (NPS employee, tour group member, unaffiliated visitor), subject activity, number of saves, incident cost, rescue method, contributing factors, search duration, and date were recorded. For personnel costs that were not specified, the average hourly cost as specified by APIS personnel was used. If values entered into the report form field contradicted the narrative report, the detailed narrative report data were considered more accurate.
Inclusion criteria for incidents classified as injury/illness were as follows: 1) the written narrative specified the initiation of the basic patient assessment; 2) the NPS form field specified the category of injury/illness and was supported in the narrative, but the nature of injury or illness was not explained; in these cases the category “not specified,” was used; or 3) a fatality was documented. For injury/illness data extraction, the narrative account was used as the primary source, and recorded categories were not limited to one chief complaint. False alarms were defined as an event in which initiation of SAR services did not involve subject contact, including self-rescue, false reports, and unattended vessels. For such events, the total event personnel hours and cost, as well as the incident date, were included in the data analysis. Saves were defined as incidents in which death would have occurred without NPS intervention, as determined by the documenting park ranger. With regard to total cost analysis, because aircraft costs proved to be significantly greater than other vessel/personnel support, data sets were separated into incidents requiring aircraft support and incidents not requiring aircraft support. These raw data sets were not normally distributed, and thus medians with ranges were calculated.
For EMS workload analysis, annual EMS workload summary sheets were used; data for the year 2008 were missing. Number of incidents requiring advanced life support, basic life support, and first aid were recorded.
A Wilcoxon rank sum test (Mann-Whitney U test) was used to compare total personnel hours and costs of injury/illness incidents vs non–injury/illness incidents as well as incidents that occurred in May to October vs November to April. These timeframes were chosen to capture recreational activity associated with the warm weather season (May–October) and cold weather season (November–April). Rates of SAR incidents and fatalities per 100,000 visitors were calculated using annual APIS visitation statistics. 2 Statistical analysis was conducted using Stata 2015; and P<0.05 was selected to signify statistical significance. Frequencies were calculated using Microsoft Excel 2016.
Results
During the study period, APIS SAR conducted 133 total SAR events assisting 261 individuals (Table 1). Two hundred individuals were not ill/injured, 57 were injured/ill, and 4 fatalities occurred. There were 25 documented saves. Out of the total 133 SAR incidents, 89 incidents (67%) involved uninjured individuals, whereas 44 (33%) incidents involved injured/ill individuals. All 4 fatalities occurred during the summer months (2 in June, 1 in August and September) and were attributed to incidents of drowning while swimming or kayaking. Thirteen incidents were categorized as false alarms. All SAR incidents were resolved within 24 hours of incident onset. During the 10-year study period, the average number of visitors per year was 187 220, with a total of 1,872,202 visitors. 2 Therefore the SAR incident rate was 7.1 per 100,000 visitors. From 2006 to 2015 (excluding the missing 2008 EMS data), there were 134 total EMS events. Because backcountry care requires frontcountry continuity, SAR injury/illness incidents are reflected in EMS workload summaries, and thus EMS data best capture total injury/illness statistics occurring in both frontcountry and backcountry. Adjusting for the absence of 2008 data by excluding its annual visitors yielded a rate of 7.8 injuries/illnesses per 100,000 visitors with an overall fatality rate of 0.5 per 100,000 visitors.
Apostle Islands National Lakeshore, 2006–2015: total SAR costs, SAR operations, fatalities, number of individuals injured/ill, number of individuals not injured/ill
SAR, search and rescue.
With regard to SAR incident demographic characteristics, among the 191 individuals for whom sex was recorded, 130 (68%) were male and 61 (32%) were female. Trends involving age resulted in peaks for individuals aged 20 to 29 y (18%) and 50 to 59 y (16%) (Table 2).
Demographic characteristics of individuals requiring APIS SAR assistance
APIS, Apostle Islands National Lakeshore; NOLS, National Outdoor Leadership School; NPS, National Park Service; SAR, search and rescue.
Visitors with no affiliation are individuals visiting APIS on personal trips without any group affiliation.
Any person belonging to a tour group.
Youth/School/Church group includes individuals with YMCA, Boy Scouts, and church- or school-affiliated field trips.
Outdoor organizations include Sierra Club, Outward Bound, NOLS, and any other wilderness-based organized group.
Employees of the NPS on personal or work time.
From 2006 to 2015, the average number of SAR incidents per year totaled 13 (standard deviation: 5; range: 5–23), with a peak of 23 incidents in 2014 and a minimum of 5 in 2006. SARs most often occurred in August (37), and overall monthly trends yielded a bimodal distribution with a summer peak in August (37) and a smaller winter peak in February (14) (Figure 1). Incidents most often occurred on the weekend and in the afternoon: 45% of incidents occurred between 1200 and 1800, and 36% of incidents occurred on Saturdays and Sundays. Among all SAR incidents, the top 3 contributing factors were high winds, errors in judgment, and insufficient equipment or experience. The top 3 rescue methods were motorized watercraft, snow vehicle, and hiking.
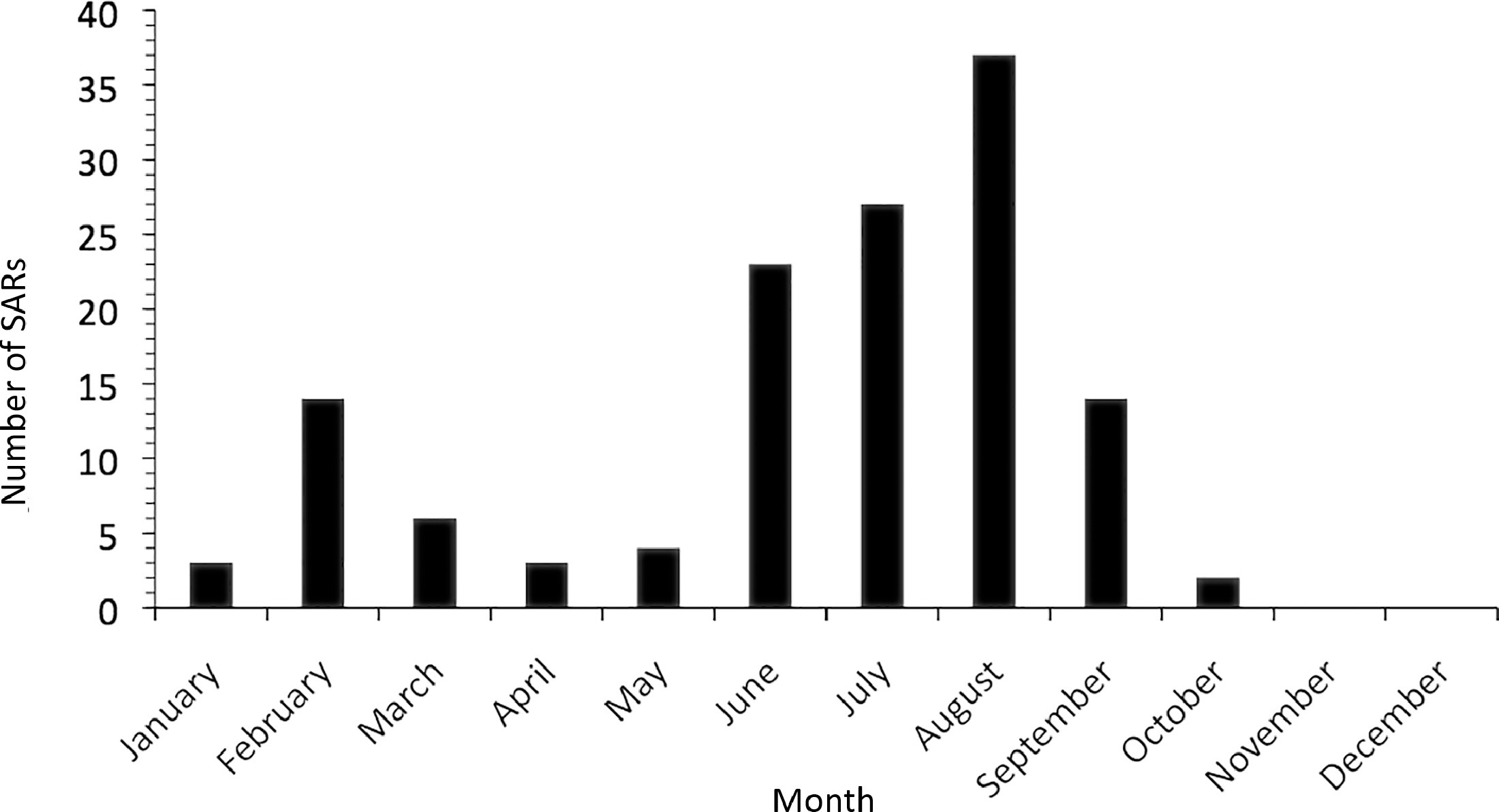
Number of search and rescue (SAR) incidents by month.
For injury/illness incidents, the most common activity was day hiking (47% of incidents), followed by nonmotorized boating (35%) (Table 3). Of the incidents that involved non–injured/ill individuals, the most common activity was nonmotorized boating (64%) followed by motorized boating (21%) (Table 3). With regard to specific injuries/illnesses identified, hypothermia/cold exposure accounted for 45% of all injuries and illnesses despite the season, followed by soft tissue injuries, fractures/dislocations, chest pain, and dehydration (Table 4).
Incidents requiring APIS SAR assistance by activity
APIS, Apostle Islands National Lakeshore; SAR, search and rescue.
Injuries and illnesses requiring SAR assistance
SAR, search and rescue.
From 2006 to 2015, SAR costs totaled $457,440 (Table 1). For events requiring aircraft support, the median cost per SAR amounted to $21,695 (range: $2993–141,849). For events not requiring aircraft support, the median cost per SAR amounted to $363 (range: $35–8830). The seven most costly SAR incidents involved aircraft support (Table 5). Comparisons of total personnel hours and costs for injury/illness incidents vs non–injury/illness incidents were not statistically significant (Table 6). Comparisons between warm and cold weather seasons had statistical significance with regard to cost (P = 0.005) but not with regard to personnel hours (Table 6). When analyzing the prevalence of injury/illness incidents, 28 out of 107 SAR incidents (26%) occurring in the warm weather months (May–October) involved injury/illness, whereas 16 out of 26 SAR incidents (62%) during the cold weather months (November–April) involved injury/illness. A comparison using a Fisher exact test was highly significant (P = 0.001).
APIS SAR incidents requiring aircraft support ranked by total cost
APIS, Apostle Islands National Lakeshore; NPS, National Park Service; SAR, search and rescue; USGS, United States Coast Guard.
Statistical comparison of personnel hours and total costs associated with SAR incidents involving injury/illness vs non–injury/illness and warm vs cold weather
Warm weather season: May–October; cold weather season: November–April.
M, median; R, range.
With respect to EMS incidents, APIS EMS responded to a total of 134 incidents, with 131 incidents requiring basic life support (BLS), 3 incidents requiring advanced life support, and 5 fatalities. Traumatic events requiring BLS (43%) and first aid (34%) accounted for the majority of the EMS workload, followed by BLS medical events (22%).
Discussion
The results of this study provide a unique new perspective as a report investigating SAR and EMS activities at an isolated National Park that sees a high proportion of water-based use. The APIS SAR incidents most often occurred during the summer months and on the weekend and most often involved men, with the most commonly reported age ranges being 20 to 29 and 50 to 59 y. These trends have been regularly reported in the existing literature. 9 –15
Though the majority of APIS SAR incidents occurred during the summer months, the winter season accounted for an increased likelihood of injury/illness incidents (Fisher exact test P = 0.001). The existing literature has identified hiking as the most commonly reported activity associated with SARs involving injury/illness.5,9,10,13,15–20 This trend was also found at APIS, with hiking being the most commonly reported activity associated with injury/illness (47%). During weather-permitting winter months at APIS, hiking out to view the ice caves is a popular activity, which likely explains the disproportionately high frequency of injury/illness incidents occurring between November and April. Specifically, the most common injury/illness encountered in the winter months were traumatic musculoskeletal injuries from falls during icy conditions.
With regard to cost analysis, previous studies investigating national park SAR cost averages have reported means, notably a 15-y review of NPS SAR incidents that reported a national mean of $895 per SAR incident. 9 Because APIS SAR incident costs were non-normally distributed and thus reported in medians, a comparative analysis is not appropriate. However, the significant difference in cost at APIS between incidents with and without aircraft support does warrant further discussion. Illustrating this large difference, a 2010 SAR operation involving a fatal drowning required 2 helicopters costing $114,591 for 10 h of aircraft time, which amounted to approximately 25% of the total APIS SAR costs over the 10-y study period (Table 5). Other types of support are significantly less expensive, with water vessels costing roughly $150 per h (depending on the vessel) and personnel hours averaging around $30 per h. These costly SAR incidents requiring aircraft support can be explained when considering APIS's geography. SAR incidents most often involved motorized and nonmotorized boating, necessitating water rescue using vessels and aircraft support in instances in which conditions limited vessel support or rapid assessment of large areas was needed.
Further delving into APIS SAR cost trends, although injury/illness incidents required approximately double the personnel hours, the median cost was similar between injury/illness and non–injury/illness incidents, without statistical significance for comparisons of either category (Table 6). Analysis of warm weather season and cold weather season SAR costs yielded a more than twofold increase in median cost during the warm weather season (P = 0.005) with similar median personnel hours (Table 6). As mentioned, in the warm weather season, recreation generally involved boating, often in larger groups, and thus tended to be multiperson rescues involving vessels and occasionally aircraft. In fact, 7 of the 8 instances requiring aircraft occurred as part of warm weather season SAR operations, most often rescuing kayakers or swimmers in rough conditions (Table 5).
Ideally, it would be most useful to compare APIS SAR and EMS activities to those of a similar park. Of the wilderness recreation areas studies published, Isle Royale National Park is remarkably similar to APIS because both are small, remote, Midwestern parks located along Lake Superior. Unfortunately a number of factors prevent a productive comparative analysis. Unlike APIS, Isle Royale is composed of one large central island more than 72 km (45 mi) long surrounded by a network of smaller islands (the largest island at APIS is less than 16 km (10 mi) long), resulting in the majority of recreation involving hiking. 12 Furthermore, the previously published Isle Royale investigation focused specifically on injury/illness trends, rather than more broad SAR activity. 12 From 2008 to 2012, Isle Royale reported 270 total injuries/illnesses and 77,039 total visitors, yielding a calculated injury/illness rate of 350 injury/illness events per 100,000 visitors, which is markedly higher than any of the previously reported rates in the literature.7,12,16,18,27 It is difficult to explain these differences because of the limited information regarding the authors’ inclusion criteria, and thus a comparison to Isle Royale is limited by these constraints. 12
More broadly, an exploration of injury/illness rates reported at other parks (and national averages) provides insight into the relative hazardousness of APIS. APIS's rate of 7.8 injuries/illnesses per 100,000 visitors is higher than rates reported at other wilderness recreation areas. An analysis of all NPS EMS incidents found an injury/illness rate of 4.6 events per 100,000 visitors. 7 Other previously published injury/illness event rates per 100,000 visitors included 4.7 at Mount Rainier National Park, 1.27 at Olympic National Park, and 2.7 at Shenandoah National Park.7,16,18 As described, APIS is a smaller, remotely located park, attracting mostly local visitors year-round. Recreation at APIS often involves unpredictable weather patterns, frequent storms, and risk of inclement weather. Additionally, APIS offers access to Lake Superior for most of the year; the surface water temperature generally does not exceed 10°C (50°F) until the end of July or early August. 28 Furthermore, wintertime can be especially dangerous, with slick and freezing conditions. These significant hazards may explain the increased reported injury/illness rate at APIS compared with other more developed and heavily visited parks.
LIMITATIONS
There are several limitations to this study. The retrospective nature of the study introduces limitations in the interpretation of correlations. Furthermore, the rigor of detail and consistency in reporting evolved over the study period; early reports had missing or sparse data compared with later years, most notably the missing 2008 EMS data. Additionally, there were instances in which information entered into report form fields contradicted information included in the narrative. In an effort to achieve as much standardization as possible, we chose to use the narrative-free text as the primary source of information in instances of omitted or conflicting information. Data extraction of injuries/illnesses was limited to the description provided in the narratives and medical training of the first responders and park rangers. In this regard, the possibility of both individual park ranger bias and data extraction bias cannot be excluded. Our time series analysis separated May to October from November to April in an effort to best capture warm vs cold weather recreational habits; however, such a time series analysis incurs the possibility for variability. Lastly, the majority of the data presented are categorical and descriptive, limiting the strength of our interpretations.
Conclusions
Our investigation highlights several important trends. The most commonly encountered injury/illness during SAR incidents was cold exposure/hypothermia, largely because of nonmotorized boaters capsizing in Lake Superior's frigid temperatures. The most expensive SAR incidents also most often involved kayakers/swimmers caught in rough water, a circumstance that has an increased rate of air and water rescue. The APIS personnel can use the results of this study to more concretely and strikingly portray the risks for visitors who may underestimate the potential danger of Lake Superior and to explain to visitors the cost associated with water rescues and the data supporting the dangers of water recreation. Additionally, because the vast majority of aircraft rescue and overall incidents occurred in the summer months, APIS may benefit from increased water vessel patrols in the peak SAR incident summer months, specifically June to September. Winter seasons permitting travel across frozen sections of Lake Superior resulted in disproportionately higher injury/illness rates as a result of falls, likely from slick conditions. The APIS personnel may also benefit from increased signage educating visitors about preventative measures to reduce falls, such as advising the usage of footwear with appropriate traction (eg, microspikes). Lastly, APIS may benefit from moving toward an electronic recording system that can gather more specific information on the location and nature of incidents to create a more comprehensive understanding of trends and staff accordingly.
Footnotes
Acknowledgements
Acknowledgments: The authors thank Apostle Islands National Lakeshore for their cooperation, collaboration, and hard work in locating and providing data. They also thank Dr Rahul Patwari and Dr Aeron Small for their assistance and input with regard to statistical analysis.
Author Contributions: Study concept and design (ES, SB, DY, TE); acquisition of the data (KC, ES); analysis of the data (ES, SB, JL, KC); drafting of the manuscript: (ES, SB, JL, DY, KC, TE); critical revision of the manuscript: (ES, JL, SB, DY, TE, KC); approval of final manuscript (ES, JL, SB, DY, TE, KC).
Financial/Material Support: None.
Disclosures: None.
Appendix A. Supporting information
Supplementary data associated with this article can be found in the online version at
Poster and abstract presented at 34th Annual Rush University Research Forum for Research and Clinical Investigation on March 1 to 2, 2017, at Rush University Medical Center in Chicago, IL; and at the 34th Annual Meeting of the Wilderness Medical Society in Breckenridge, CO, on July 31, 2017.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.