
Abstract
Objective
Many Americans sustain large animal-related injuries (LARIs) from blunt trauma. We compare the injuries and management of LARI in our region of the United States with those of motor vehicle crashes (MVCs).
Methods
A 15-year retrospective study of trauma patients with LARI matched to MVC controls by Injury Severity Score (ISS), age, and sex was conducted. Values were statistically compared, and differences were considered statistically significant at P < .05.
Results
There were 156 LARI cases, of which 87% were related to horses, 8% to bulls, and the remainder to deer, mules, bison, cows, and rams. In the LARI group, the age was 42±18 years (mean±SD), ISS was 7±4, and 61% were females. The MVC group had a significantly longer length of hospital stay (5±5 vs 4±3 days) and blood alcohol concentration (35±84 vs 3±20 g/L). There were no significant differences in injury patterns between LARI and MVC; however, additional radiological studies (RS) were performed on MVC (9±6 vs 7±5). LARI patients were more often transferred from rural locations (39% vs 25%) and traveled further to our trauma center (40±32 vs 24±29 km) than did MVC patients.
Conclusions
LARI has a similar pattern of injury to MVC, but fewer RS. LARI typically occurred further away, requiring transfer from rural areas to our institution. We recommend a similar approach for the evaluation of LARI and MVC.
Introduction
An estimated $60 million were spent in the United States on large animal-related injuries (LARIs) in 2001. 1 Most of these injuries are categorized as blunt force trauma, related to being thrown or kicked by an animal. Both domestic and wild animals have been implicated in large animal attacks throughout the United States. 2 –5 Many animal-related injuries inflicted on humans occur in the wilderness. Langley and Morrow reported an average of 157 deaths per year in the United States from animals. The study also found that this is an under-recognized public health hazard, as many patients do not seek medical attention in a timely fashion. 6 Horses and cattle cause the majority of occupational fatalities among animal-related events in the United States. 7 These animals were also responsible for the majority of animal-related deaths in New Mexico from 1993 through 2004. 8 The majority of these occurred in rural settings. Injuries from large animals can be under-triaged at rural hospitals due to their relative infrequency, and therefore may not receive the prompt medical attention they require.
About 30 million Americans ride horses every year, while many more work with or near horses and other large animals.1,9 In the United States, there were 205 riding fatalities reported from 1976 through 1987, and every year more than 100,000 emergency department visits are related to injuries sustained from horse-related activities. 10 It has been reported that 11.2% of horse-related injuries require hospitalization, as compared with 5.5% of all injuries. 11 Horse-related trauma can have a wide range of severity and injury patterns due to the strength, weight, speed, and unpredictable nature of these animals. 10
Another significant proportion of LARI is due to interactions with cattle. According to Langley et al, cattle were responsible for 40% of work-related fatalities in the United States. The same study reported that 12,000 professional rodeo riders compete throughout the United States and Canada each year, with an injury rate of 2.4 to 19.7 per 100 exposures. 7
Ours is a unique study as, to our knowledge, there is no literature comparing the injury type or severity of LARI with motor vehicle crashes (MVCs), which are a more common mechanism of blunt trauma. In addition, many previous studies have focused specifically on LARI in equestrians, but have not addressed injuries inflicted on nonriders from kicking and other mechanisms, which make up more than 25% of LARI. 12 We hypothesized that LARI involving a blunt trauma mechanism has similarities to MVC, and tested this by addressing 3 objectives. First, we determined the incidence and type of LARI seen at our institution. Second, we compared these injuries to those sustained in MVCs. Third, we determined whether there were any differences in the management of LARI as compared with that of MVC at our institution.
Methods
Data from our institution’s American College of Surgeons-verified level I trauma center, which serves both urban and rural populations, including a large number of Amish communities, were retrospectively analyzed. Such centers provide 24-hour trauma coverage with capabilities for treating all types of injuries and utilizing subspecialty teams. In addition, level I trauma centers are major teaching hospitals affiliated with universities with residency programs, research activities, and injury prevention and outreach programs. The data were collected from the center’s trauma registry from the years 2000 through 2015 to identify LARI. The LARI patients were then matched to MVC controls using Injury Severity Score (ISS), age, and sex. The injuries, workup, treatment, and outcomes in both groups were identified and compared. The data collected from the registry and each patient’s medical record included the following: the mechanism and type of injury; type and number of medical comorbidities (diabetes, heart disease, respiratory disease, and cancer); blood alcohol concentration (BAC); positive drug toxicology screen (TOXPOS); number and type of radiological studies (RSs), which included plain radiography and computed tomography (CT); surgical and orthopedic procedures; chest injuries (rib fractures and pneumothoraces); ventilator days; mortality; hospital length of stay (LOS) in days; discharge disposition; transfer from rural hospitals; and distance traveled to our trauma center (in kilometers).
The data were stratified into 2 groups (the LARI group and the matched MVC control group) for comparison. Statistical analysis was performed using the SPSS package (Armonk, NY). Values are reported as mean±SD, or raw percentage, as appropriate. Student’s t tests, χ2 tests, or nonparametric Mann-Whitney U tests were applied where appropriate. Differences were considered statistically significant at P < .05.
This study was approved by the trauma center’s Institutional Review Board and Human Subjects Review Committee.
Results
There were a total of 21,762 patient records, from which 5804 MVCs and 156 LARIs were identified. The most commonly encountered LARIs were horse-related (136, 87%), with 72% related to being thrown from a horse and 28% to being kicked by a horse. LARIs involving bull encounters occurred in 13 cases (8%). Of these, 10 individuals were thrown from bulls and 3 were struck by a bull. These injuries primarily occurred at a bucking bull ranch that features bull riding and is located 48 km from our hospital. The remaining 7 (5%) LARI cases were related to being attacked by a deer (2), thrown from a mule (2), gored by a bison (1), kicked by a cow (1), and struck by a ram (1).
The most common operations performed were orthopedic surgeries. There were 14 patients with solid organ injuries, including 10 LARIs and 4 MVCs. In a subanalysis of LARI cases, there were more solid organ injuries in patients kicked by large animals (70%) than in those thrown from large animals (30%). Chest injuries were composed of rib fractures (18% LARI and 15% MVC) and pneumothoraces (8% LARI and 7% MVC) (Figure 1). There was 1 death in the study population. This occurred in the LARI group in a patient who was thrown from a horse and died from multisystem organ failure secondary to hemorrhagic shock.
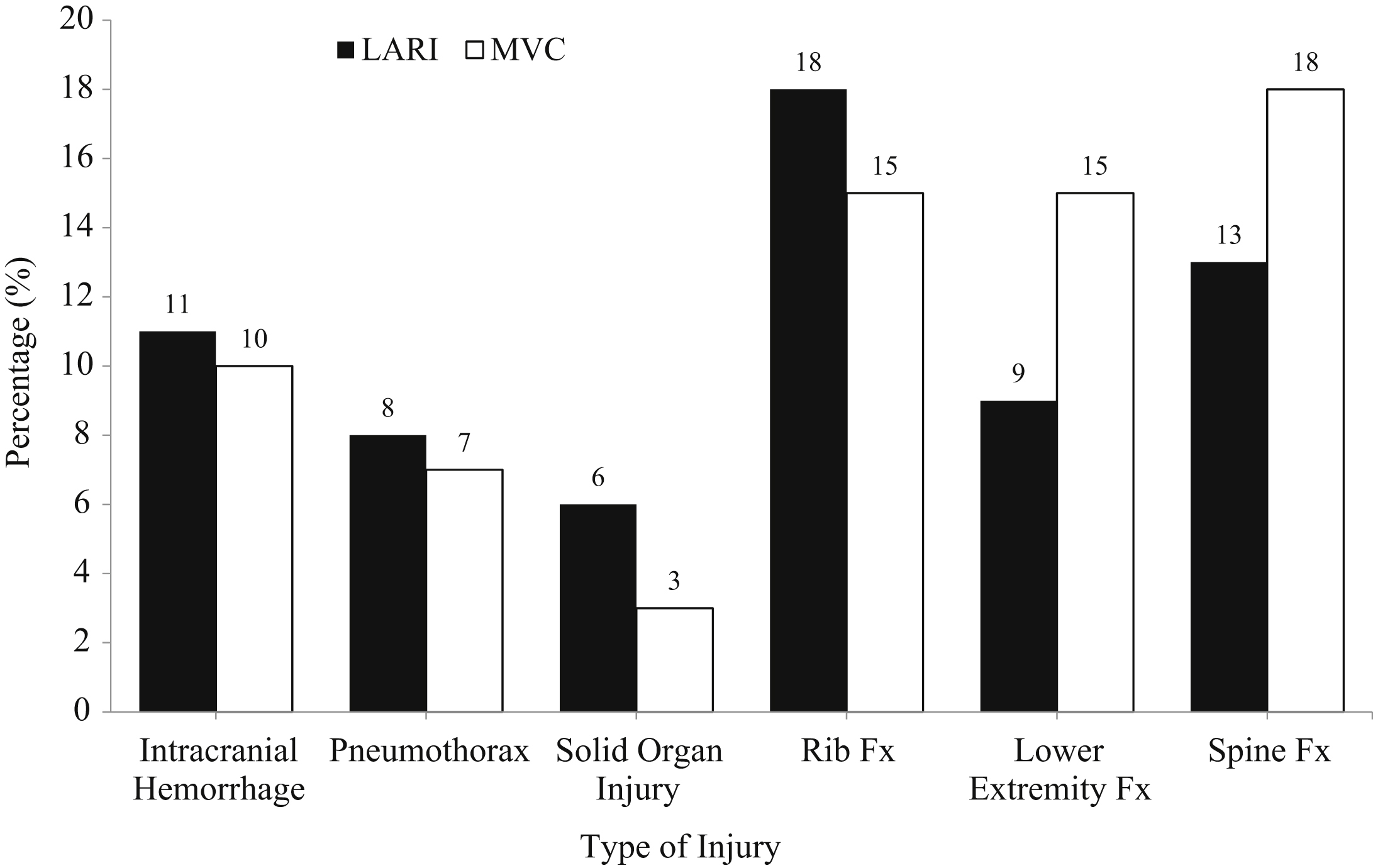
Type of injury (%)—LARI vs MVC matched controls. LARI, large animal-related injury; MVC, motor vehicle crash; and Fx, fracture.
There were 2 missed injuries in our study, both in the LARI group. One patient was thrown from a horse and was not found to have rib fractures until the tertiary trauma survey was completed the following day. The second injury was missed by a rural hospital. The patient was initially evaluated after being kicked in the chest by a horse and was diagnosed with a single rib fracture and discharged home. Four days later, the patient returned to the same hospital with worsening abdominal pain and shortness of breath, and was found to have 4 rib fractures and a grade 3 splenic injury. The patient was then transferred by helicopter to our institution for more definitive management.
There were no differences between LARI and MVC in terms of the number of comorbidities, TOXPOS, number of general surgery procedures (4 LARIs vs 5 MVCs), number of orthopedic procedures (34 LARIs vs 40 MVCs), ventilator use (4 LARIs vs 11 MVCs), and discharge disposition. The MVC group had a higher LOS and BAC. The LARI group was more frequently transferred from rural hospitals and traveled a greater distance to our trauma center (Table). No significant differences were found in the types of injuries between the LARI and MVC groups (Figure 1). MVC patients more often had RS performed than did LARI patients. Specifically, MVC patients underwent more head RS, lower extremity RS, pelvis RS, and spine RS (Figure 2).
Summary of demographics, comorbidities, hospital length of stay, distance to level 1 trauma center (mean±SD), drug screen, transfers, and discharge disposition (%)
LARI, large animal-related injury; MVC, motor vehicle crash; BAC, blood alcohol content; TOXPOS, positive drug toxicology screen; LOS, length of stay.
P < .05 between LARI and MVC.
Transfer is a transfer from an outside rural hospital.
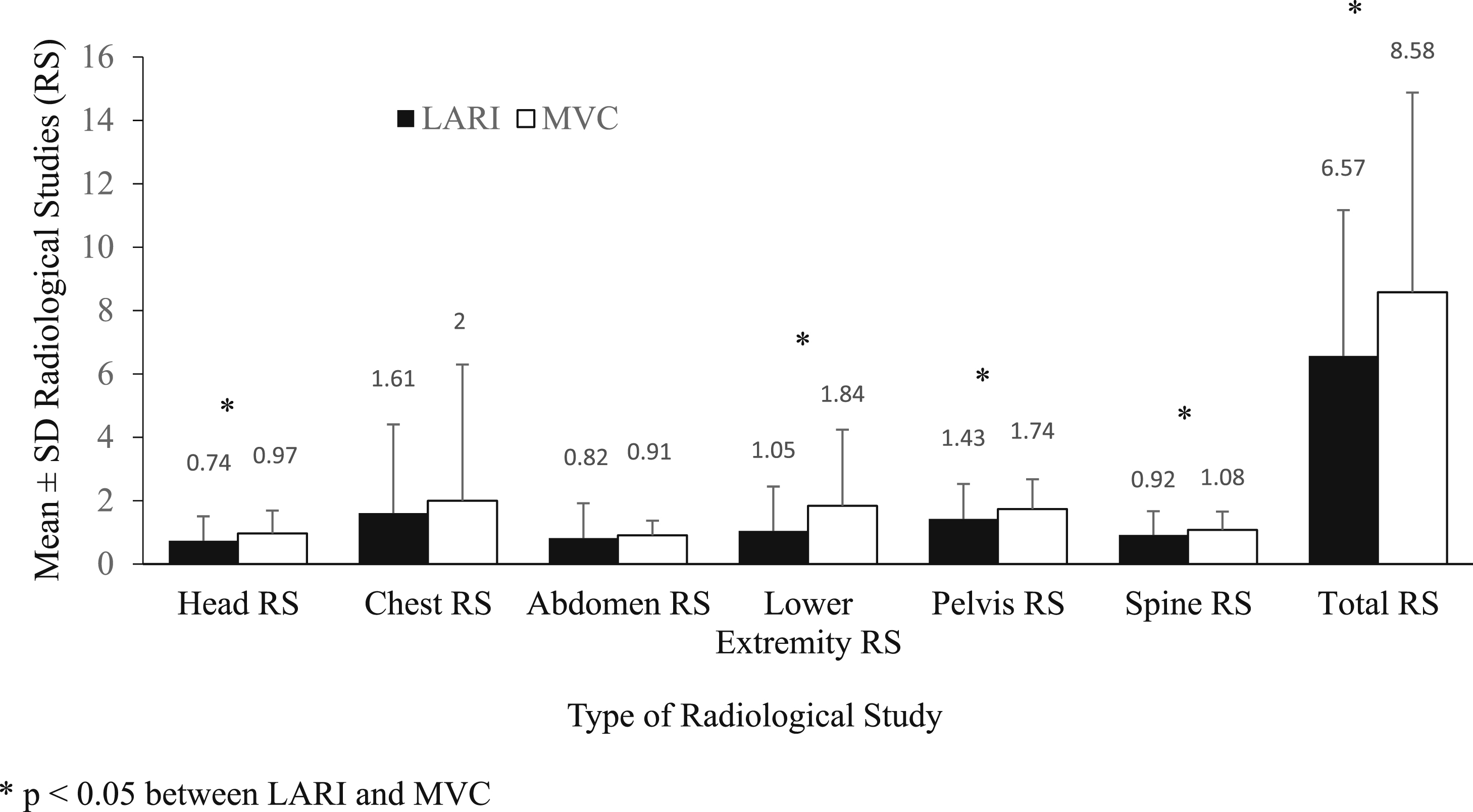
Type of RS performed (mean±SD)—LARI vs MVC matched controls. LARI, large animal-related injury; MVC, motor vehicle crash; and RS, radiological studies.
Discussion
The results from this 15-year retrospective study demonstrate a similar pattern of injuries between LARI and injuries related to MVC. Overall, LARI involved various types of injuries, including intracranial hemorrhage; solid organ injury; tissue contusions; fractures of the skull; injuries to the ribs, extremities, pelvis, and spine; and pneumothoraces. As demonstrated in previous studies, the most common animals involved in LARI in our study were horses, followed by cattle.
A study performed in Lexington, Kentucky, found a similar trend in the frequency of presentation to a level I trauma center due to injuries sustained from horse-related trauma. Out of 10,020 blunt trauma victims, 0.75% were admitted for injuries related to contact with horses, and of those, the majority of cases were from being thrown (53%), thrown and crushed (12%), kicked (12%), or crushed (12%) by horses. 10 Although the difference in lifestyle between Lexington and the area served by our institution could skew the demographic comparison, there is still a clear trend towards the majority of LARI primarily resulting from being thrown by a horse, and secondarily from being kicked by a horse. In our study, the incidence of horse-related injuries was 0.62%, which is comparable to that of the Lexington study above.
Bull riding was the second most common mechanism of LARI in our study. These injuries primarily occurred at a bucking bull ranch. Fortunately, an emergency medical service (EMS) team is on standby at these events to allow prompt medical treatment and transfer to a suitable center for more definitive care.
There were no significant differences in ventilator use and the number of general surgery or orthopedic procedures in the LARI and MVC groups. There were 2 patients with missed injuries, neither of whom experienced any complications or required interventions due to the missed injury. One injury was picked up during our tertiary trauma survey, while the other was missed by a rural hospital and not identified until the patient re-presented days later. This equates to a missed injury rate of 1% for LARI, which is less than the 1.5 to 4.3% reported in the literature. 13
There was a significant difference in transfer rates and distance traveled to our hospital in the LARI group compared with the MVC group. This demonstrates that LARI occurs more frequently in remote settings, further from the resources of a tertiary care center, such as our level I trauma center. One such transfer was a LARI that occurred 32 km from our trauma center. The patient was a 78-year-old man who was attacked by a deer in the late fall and lay in the field for 4 hours until he was discovered by a neighbor. By the time the EMS arrived, he was cold and mottled. As a result of his hypothermia and vasoconstriction, the EMS team was unable to obtain a temperature reading or pulse oximetry saturation. The patient did not arrive at our emergency department until 5 hours after the injury, by which time he had been rewarmed. Fortunately, his injuries consisted of complex lacerations and an abdominal wall hematoma, which were not life-threatening. Had this occurred in a colder, more austere environment, the patient may have suffered severe life-threatening complications from profound untreated hypothermia.
The only death encountered in our study was a LARI that had occurred in a rural area 72 km from our hospital. The patient was a 60-year-old man who was thrown from and crushed by a horse and lay in the field for 40 minutes until the EMS arrived. The patient was then transported to a rural hospital before being transferred by helicopter to our level I trauma center, 3 hours after the time of injury. Upon arrival, the patient was hypothermic and hypotensive due to hemorrhagic shock, and was actively being resuscitated with blood products. He was diagnosed with an open book pelvic fracture and retroperitoneal hematoma, and was taken to the operating room for application of a pelvic external fixator and exploratory laparotomy. He ultimately died 12 days later, due to multisystem organ failure. His remote location and subsequent delay in treatment of hemorrhagic shock were considered to be contributing factors in this patient’s death.
Griffen et al found head injuries to be the second most common injury in patients thrown by horses, and these accounted for all 5 deaths in their study. 10 This was in contrast to our findings of intracranial hemorrhages as the third and fourth most common injuries in LARI and MVC, respectively; in our study, these did not result in any mortalities. Head injuries have been repeatedly shown to be the most common cause of death from LARI. 1 ,8,10 Although we did not have data about helmet use, other studies have supported that death from large animal-related trauma is quite rare in individuals wearing properly fitted helmets. 14 Given that the use of riding helmets has been shown to decrease the number of head injuries by at least 5-fold, 15 efforts to increase helmet use are an important part of prevention of LARI and LARI-related deaths.
The majority of cattle-related fatalities are caused by blunt force trauma to the chest and abdomen. 8 In our study, the majority of solid organ injuries occurred in patients who were kicked by large animals. Given these findings, people working closely with large animals would likely benefit from wearing protective gear over the torso, as this may reduce morbidity and mortality from LARI. This is an area for further study, as there is limited data on this matter in the literature.
In our study, fewer RS were performed for LARI patients than for MVC patients. This is important, as the 2 groups showed no differences in the pattern or severity of injury, yet their initial imaging evaluation was different. At our institution, we are more liberal in the use of RS in patients involved in MVC. This may be due to our physicians’ interpretation of recent literature discussing the utilization of CTs in rapid deceleration mechanisms and of pan-CTs in blunt trauma.16,17 Another reason for this is the number of patients with positive BAC among the MVC controls, which makes their physical examination less reliable and our threshold for using RS higher.
This study has several potential limitations. First, the study suffers from limitations that are inherent to any retrospective review from a single center with a relatively small sample size. Second, we did not actually identify whether protective equipment was used by any of our patients. It would be interesting to compare the frequency and severity of injuries sustained with and without the use of protective equipment, but, unfortunately, we had insufficient data available to study this aspect. Third, the number of LARI in our region may be underrepresented at our institution for a number of reasons. First, there are other verified trauma centers within our region that serve the same population. Second, we are an adult-only institution and injured children would have been transported to the local children’s trauma center. Finally, many LARI were likely treated at rural hospitals or never sought treatment if they sustained injuries that did not require the resources of a level 1 trauma center.
In conclusion, our study appears to support that of others on large animal-related trauma, as injuries were more common in women and the most common mechanism of injury was being thrown from a horse, followed by being kicked by a horse. 11 Our study is unique in that we compared LARI to another mechanism of blunt trauma (ie, MVC). Since MVCs are a much more prevalent mechanism of injury than LARIs, we can incorporate concepts from managing patients involved in MVC to those involved in LARI. Emergency room physicians and trauma surgeons must be cognizant that LARI is a significant mechanism of injury and needs to be evaluated in a similar manner to MVC injury. In addition, healthcare providers in rural settings should counsel their patients on safety around large animals and injury prevention—including the use of protective equipment—and seeking prompt medical attention after LARI, as large animal-related trauma can result in more significant injuries than may be perceived at first. Our finding that the blunt trauma mechanism of LARI is similar to that of MVC is particularly important for centers that do not frequently encounter LARI. We recommend that the evaluation of LARI patients be similar to that used for MVC patients.
Ethics Approval and Consent to Participate: This study was approved by the Cleveland Clinic Akron General Institutional Review Board and Human Subjects Review Committee (IRRB number 10041).
Availability of Data and Supporting Materials: Data is available upon request.
Acknowledgments: We would like to thank Editage (
Authors Contributions: Study concept and design (RM, AS, FM); acquisition of data (AT, MM, CW, CD, AS); analysis of data (AT, RM, AS, FM); drafting of manuscript (AT, MM, CW, AS); critical review of manuscript (AT, RM, AS, FM); and approval of final manuscript (AT, RM, AS, FM).
Footnotes
☆
Abstract presented at the American College of Surgeons Clinical Congress, September 30 to October 2, 2012, Chicago, IL.
☆☆
Abstract presented at the American Medical Association Resident and Fellow Section, 12th annual AMA Research Symposium, November 7, 2014, Dallas, TX.