
Abstract
Intersection syndrome is an inflammatory condition located at the crossing point between the first and second dorsal compartments in the wrist. It is an uncommon presentation but has been recognized as an injury typical of rowers (when it is named oarsman’s wrist) and other sports such as racquet sports, baseball, cycling, hockey, golf, ice hockey, skiing, and softball. It has not been previously described in climbers. This report details 2 cases of intersection associated with the use of an ice axe. The first presentation was in a female climber who was using an ice axe for climbing in the Nepal Himalayas and the second was in a male climber using an ice axe for winter climbing training in the Alps. Both climbers presented with wrist pain, swelling, and crepitus over the dorsum of the wrist, about 5 cm proximal to Lister’s tubercle. Although well documented in other sporting populations, there seems to be limited reporting of intersection syndrome in the climbing population. It may be worth considering a diagnosis of “ice axe wrist” as a differential in patients who have been using ice axes in climbing or mountaineering.
Introduction
Intersection syndrome describes an inflammatory condition located at the point at which the abductor pollicis longus (APL) and extensor pollicis brevis (EPB) tendons cross the extensor carpi radialis brevis (ECRB) and extensor carpi radialis longus (ECRL) tendons in the forearm 1 (Figure 1). It is typically an overuse injury and is relatively uncommon, but has been recognized as an injury typical in rowing and other sports such as racquet sports, baseball, cycling, hockey, golf, ice hockey, skiing, and softball.2,3 It has also been noted in a hand cyclist. 4 There are various monikers for the condition including “oarsman’s wrist,” “bugaboo forearm,” “peritendinitis crepitans,” “crossover syndrome,” and “squeaker’s wrist.” A search of the literature has been carried out prior to the writing of this case, and there has been no report of intersection syndrome in climbers or mountaineers. Studies looking at ice climbing report the majority of injuries being penetrating injury, 5 injuries due to falling ice, 6 and more serious injury. 7 One study reports an overuse injury in the arm but does not specify the nature of the injury. 8 This case report details the presentation of 2 climbers with intersection syndrome where both had been using an ice axe.
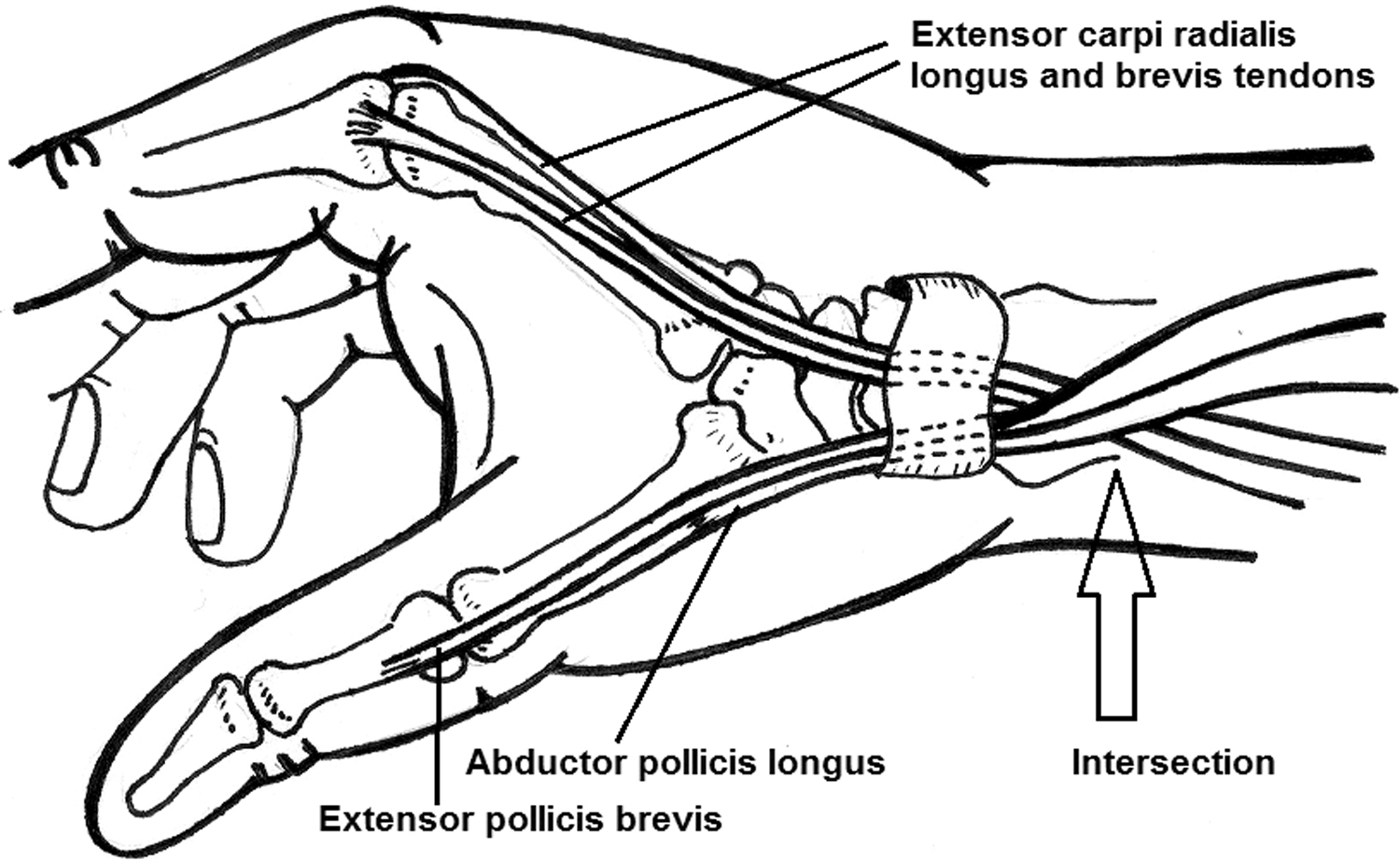
Diagram of anatomy of intersection point of APL and EPB tendons (first extensor compartment) with ECRL and ECRB tendons (second extensor compartment). Illustration by Kate Connolly, MD.
Case Report
Case 1
A 36-year-old female climber presented with gradual onset wrist pain over several days of climbing on mixed rock and ice at 5,000 m altitude in the Himalayas. She was otherwise fit and well with no relevant medical history, and had been using a technical ice axe (with a curved shaft) during the course of the day. The patient presented with unilateral wrist pain over the dorsum of the wrist on the radial side of the dominant hand, about 5 cm proximal to Lister’s tubercle (Figure 2). Pain was present on wrist movement in general, but in particular on active extension and radial deviation. Swelling in this area was evident and crepitus was present on active and passive wrist flexion, extension, radial, and ulnar deviation. Finkelstein’s test was positive but the main area of tenderness was further from the wrist, rather than over the first dorsal compartment. Neurovascular examination was normal and there was no pain or restriction to movement in the elbow, shoulder, or neck. Treatment consisted of icing the injury initially, and then the wrist and thumb were taped using zinc oxide tape. The technique used was similar to a thumb spica with tension on the tape from the radial aspect of the hand to the ulnar side, starting from the dorsal aspect and wrapping around the palmar aspect of the wrist, and with extension of the taping proximally to cover the area of tenderness (Figures 3 and 4). The aim of the taping was to reduce thumb and wrist extension and radial deviation, and to give a compression element to reduce the swelling. The patient was due to climb again the following day, which followed without significant problems with the taping in situ. Over the course of the next couple of days the symptoms settled with repeated ice and continued taping. Treatment and further follow-up were limited due to the location of the climber.

Image of ice axe in hand with area of intersection highlighted.

Taping method used as treatment: thumb part of taping. Actual taping was more substantial; these images are for reference.

Taping method used as treatment: wrist part of taping added. Actual taping was more substantial; these images are for reference.
Case 2
A 32-year-old male climber presented with gradual onset wrist pain over a week of climbing on mixed rock and ice in the Alps. He had been using a technical ice axe during the week. He was otherwise fit and well with no relevant medical history. The patient presented with unilateral wrist pain over the dorsum of the wrist on the radial side of the dominant hand, about 5 cm proximal to Lister’s tubercle on wrist movement in general, but in particular on active extension and radial deviation. Swelling in this area was evident and crepitus was present on active and passive wrist flexion, extension, radial, and ulnar deviation. Finkelstein’s test was positive, but the main area of tenderness was further from the wrist, rather than over the first dorsal compartment. Neurovascular examination was normal and there was no pain or restriction to movement in the elbow, shoulder, or neck. As in case 1, the treatment consisted of icing the injury initially and then the wrist and thumb were taped using zinc oxide tape. The technique used was again as for a thumb spica, with tension on the tape from the radial aspect of the hand to the ulnar side, starting from the dorsal aspect and wrapping around the palmar aspect of the wrist, with extension of the taping proximally to cover the area of tenderness. The aim of the taping was to reduce thumb and wrist extension and radial deviation, and to give a compression element to reduce swelling. The climber did not climb over the next couple of weeks, and, again, the symptoms settled quickly over a few days with little intervention.
Discussion
Intersection syndrome is a noninfectious, overuse disorder of the distal forearm located at the site of communication between the first and second dorsal compartments of the wrist. The first dorsal compartment contains the APL and EPB tendons, and the second dorsal compartment contains ECRB and ECRL tendons. The presenting symptoms are of pain, swelling and, in severe cases, crepitus on the dorsum of the wrist approximately 4 to 8 cm proximally to the radial styloid. These symptoms are the result of a tenosynovitis or peritenosynovitis, an inflammation of and around the tendon sheath. 4 ,9,10 There is some debate in the literature that the cause may either be from friction between the muscle bellies of the first compartment and the tendon sheath of the second, 11 or by a stenosis type injury from tightness of the second compartment’s tendon sheath. 12 It would seem reasonable to consider that there could be elements of both involved in these cases, given the acute nature of the onset of symptoms following a repetitive, unaccustomed activity.
In these 2 particular cases the other main diagnosis to consider was De Quervain’s tenosynovitis, an inflammatory condition of the first extensor compartment alone. It can be differentiated from intersection syndrome as the area of tenderness is typically along the course of the tendon sheath, distally from the radial styloid towards the thumb, rather than more proximally. 10 Other diagnoses to consider were a blunt trauma to the wrist or entrapment of the dorsal radial sensory nerve. Intersection syndrome was diagnosed in both cases after consideration of the mechanism of injury, repetitive use of the wrist rather than the thumb, and, in particular, the location of the pain and swelling. There was no imaging available to confirm the diagnosis. Both cases resolved with conservative management, and in 1 case, the aggravating activity was continued with the aid of strapping and without significant limitations. Indeed the literature confirms that the majority of cases should resolve with conservative management. 3 ,4,10
Intersection syndrome is typically associated with repetitive flexion and extension of the wrist, 2 but it has also been reported in skiers on repetitive withdrawal of the planted ski pole in deep snow. 13 It is hypothesised that the forceful, repetitive wrist extension and radial deviation associated with removing the pick of the ice axe from the ice, the same type of action as removing a planted ski pole, precipitated the onset of symptoms in both these cases. Other causes of injury have been considered, such as using ice screws or rope work, and it is a limitation of these cases that the author cannot completely exclude another causative or contributing factor. However, the action of removing an ice axe from the ice correlates most closely with the mechanism required to cause these symptoms. It is also possible in this type of injury that a tightly constricted axe leash could cause compression at the wrist and contribute to the friction or stenosis at the intersection point. In both cases, leashes were used but both climbers deny that they were excessively tight.
Both climbers were engaged in expedition-type climbing which incorporated sections of steep ice and snow ascent, rather than vertical ice climbing (for example on waterfalls). It would be interesting to gauge the level of incidence in both these populations. Neither climber used ice axes on a regular basis, and so the potential for developing an overuse injury was higher than if they were accustomed to the activity. They may have had poor technique or have fatigued over the course of the activity. It would be useful to ascertain whether ice axe technique and/or ice axe handle type has a role to play in development or prevention and treatment of the symptoms.
Conclusion
Although well-documented in other sporting populations, there seems to be limited reporting of intersection syndrome in the climbing population. It is worth considering this diagnosis of “ice axe wrist” as a differential in patients who have been using ice axes in climbing or mountaineering.
Acknowledgments: With thanks to the 2 climbers for allowing me to use their injury presentations in this case report and to the International Porter Protection Group (IPPG UK) for allowing me to work at their rescue post in Machermo, Nepal.
Ethical statement: Written informed consent was obtained from both patients for this report. Within the report I have not utilized any identifiable factors.
No formal ethical approval required.
Financial/Material Support: None.
Disclosures: None.
Footnotes
Submitted for publication October 2016.Accepted for publication March 2017.