
Abstract
We describe a patient with missed traumatic pneumothorax due to penetrating neck injury that was presumably caused by a stingray while diving. The barb can result in significant injuries to deep structures and organs despite a deceptively small entrance wound. This case underscores the importance of performing a thorough examination and having a high suspicion of distant injury in patients with penetrating neck injuries.
Introduction
The stinger or barb on the tail of a stingray can cause trauma and envenomation as well as injury to deep organs, even if the entry wound is small. Most stingray injuries occur on the lower extremities. Here we report an unusual case of traumatic pneumothorax after a penetrating neck injury presumably caused by a stingray barb. This injury was initially missed, underscoring the importance of performing thorough examination and considering the possibility of deep organ involvement in a patient with penetrating neck injury.
Case report
A 45-year-old previously healthy man was transported to our emergency department by ambulance. He was a professional abalone diver. He had suddenly felt pain in the neck while diving for abalone and stated that something bit him on the neck, but he only saw a large shadow swimming away. He complained of excruciating neck pain and numbness around the wound. On examination, he was alert and afebrile without dyspnea. The pulse rate was 105 beats/min, blood pressure was 149/115 mm Hg, and respiratory rate was 24 breaths/min. Pulse oximetry showed an oxygen saturation of 96% on room air. Breath sounds were normal bilaterally. He had a wound about 2 cm in diameter and apparently 1 cm deep in the right anterior cervical region (Figure 1). After intravenous fentanyl (0.05 mg) was administered, the wound was carefully cleaned by using a hot shower (about 40°C) under local anesthesia. There was no active bleeding, and no foreign bodies were detected. We concluded that he had a relatively superficial bite wound caused by an unknown marine creature. A Penrose drain was placed, the wound was sutured, and amoxicillin-clavulanate (500 mg/125 mg orally 3 times daily) was prescribed to prevent wound infection. We did not perform imaging studies because the injury seemed to be superficial. In addition, his vital signs were stable and there were no indications of any need for emergency management.

The stingray wound is located in the right anterior cervical region between the cricoid cartilage and clavicle.
At follow-up the next day, the patient had no dyspnea and his pain was improving. However, subcutaneous emphysema was detected in the cervical region, and breath sounds were decreased on the right side of the thorax. Chest radiography demonstrated right pneumothorax with subcutaneous and mediastinal emphysema (Figure 2). Both Dasyatis akajei (the whiptail ray) and Dasyatis matsubarai (the pitted stingray) are common in the sea where the patient was diving near Kamogawa city (Chiba, Japan), so we diagnosed zone 1 neck injury and traumatic pneumothorax due to possible stingray injury. Contrast-enhanced computed tomography of the neck revealed no findings suggestive of vascular injury. He was admitted to our hospital, and a chest tube was inserted. Because of concern about infection, we reopened the neck wound for irrigation and changed his antibacterial therapy to 12 g daily intravenous ampicillin-sulbactam (3 g every 6 hours). It was presumed that the wound was deep enough to reach the upper thorax and cause pneumothorax, corresponding to a stab injury in zone 1. 1
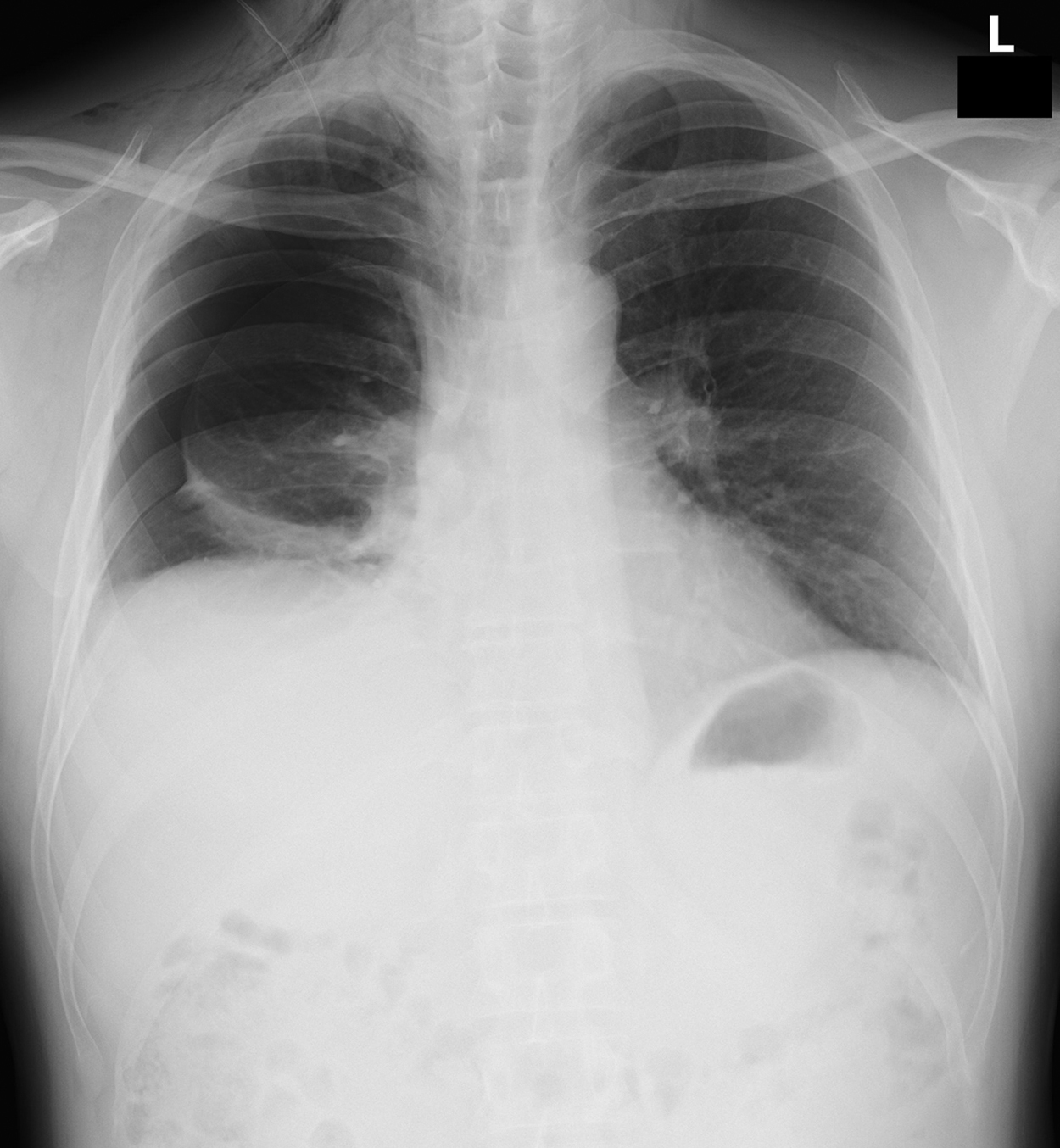
Chest radiograph showing right pneumothorax and subcutaneous emphysema. There is a Penrose drain in the neck.
After admission, the patient’s pneumothorax improved, and the chest tube was removed on hospital day 3. However, wound healing was delayed and necrotic tissue was identified, so debridement was performed under general anesthesia on hospital day 18. No foreign bodies were detected in the wound, which extended to at least the region between the anterior and middle scalene muscles. Pathologic examination of the resected tissue revealed extensive skeletal muscle necrosis with regenerative changes and infiltration of inflammatory cells. Postoperative recovery was uneventful, and the patient was discharged on hospital day 24. The patient’s written consent to publication of this report was obtained.
Discussion
Stingrays are flat cartilaginous fish with spiny tails. They are usually not aggressive and only attack when disturbed.2,3 Stingrays generally inhabit tropical and subtropical waters worldwide. 4 D akajei and D matsubarai of the Dasyatidae family are the most common stingray species in the sea where the patient was diving, with D akajei being the major species in this area and often sighted in shallow water.
Most injuries occur when an unsuspecting person steps on a stingray hidden in the sand, usually in shallow water3,5; therefore, more than 90% of stingray injuries affect the lower extremities. To our knowledge, only 2 cases of traumatic pneumothorax caused by stingrays have been reported.6,7 Jhamb et al 6 reported a patient with an abdominal stingray wound complicated by liver injury and pneumothorax, and Parra et al 7 reported a patient with a chest wound complicated by cardiac injury and pneumothorax. Thoracic stingray injury can occasionally cause death, as in the case of Steve Irwin (“The Crocodile Hunter”), who is probably the most famous victim of such injury. He was an Australian wildlife expert and television personality who was fatally stabbed in the chest by a stingray barb while filming an underwater documentary in 2006.
Penetrating neck injuries are potentially fatal and require emergency treatment. 8 The depth of the wound should be evaluated carefully along with possible damage to deep organs. However, estimating the depth of a penetrating injury is often difficult because it is influenced by the cause (type of weapon, dimensions, etc.), angle of insertion, force applied, skin elasticity, and other factors. A pointed weapon like an icepick can cause injury to deep organs despite only producing a minor skin wound. 9 Likewise, the sharp barb on the tail of a stingray can cause deep organ injury, even if the superficial wound is small. With penetrating injuries to the neck, detailed physical examination and imaging is essential to accurate and timely diagnosis. Shiroff et al stated that invasive screening strategies such as computed tomography angiography should be considered in patients with penetrating neck injuries, even if they are hemodynamically stable. 10
In addition to direct trauma, stingray injuries result in injection of venom that causes local inflammation and poor wound healing. 7 Stingray venom causes marked vasoconstriction that leads to severe pain, ischemia, and tissue necrosis. 11 The venom is reported to be heat labile, but it is not inactivated by immersion in hot water, although this alleviates pain through vasodilatation. Some experts have recommended immediate immersion of the wound site in hot water.3,12 However, evidence of a beneficial effect of hot water immersion on stingray stings is not strong and there have been no randomized controlled trials. 13 According to some reports, a temperature >50°C is required for inactivation of the venom, which could be too hot for patients to tolerate.5,6 Atkinson et al reported that showering after marine envenomation might have the benefit of washing off any remaining stinging cells, as well as alleviating pain as in hot water immersion. 13 Although it is easy to immerse an injured leg or arm in hot water, immersion is difficult when the patient has a trunk or neck injury. Although we did not suspect stingray injury, we irrigated our patient’s wound with hot water at about 40°C using a shower for cleansing and pain relief.
In conclusion, injury to deep organs/structures should be suspected if a patient has a stab wound caused by a stingray, despite the deceptively small entrance wound. When penetrating injury from a stingray encounter is evaluated, a thorough physical examination and low threshold for imaging is paramount given the potential for distant injury.
Author Contributions: Study concept and design (TS, TT); drafting of the manuscript (TS, TT, JF); critical revision of the manuscript (TS, TT); approval of final manuscript (TS, TT, JF).
Financial/Material Support: None.
Disclosures: None.
Footnotes
Submitted for publication September 2016.
Accepted for publication February 2017