
Abstract
Despite advances in outdoor clothing and medical management of frostbite, individuals still experience catastrophic amputations. This is a particular risk for those in austere environments, due to resource limitations and delayed definitive treatment. The emerging best therapies for severe frostbite are thrombolytics and iloprost. However, they must be started within 24 hours after rewarming for recombinant tissue plasminogen activator (rt-PA) and within 48 hours for iloprost. Evacuation of individuals experiencing frostbite from remote environments within 24 to 48 hours is often impossible. To date, use of these agents has been confined to hospitals, thus depriving most individuals in the austere environment of the best treatment. We propose that thrombolytics and iloprost be considered for field treatment to maximize chances for recovery and reduce amputations. Given the small but potentially serious risk of complications, rt-PA should only be used for grade 4 frostbite where amputation is inevitable, and within 24 hours of rewarming. Prostacyclin has less risk and can be used for grades 2 to 4 frostbite within 48 hours of rewarming. Until more field experience is reported with these agents, their use should probably be restricted to experienced physicians. Other modalities, such as local nerve blocks and improving oxygenation at high altitude may also be considered. We submit that it remains possible to improve frostbite outcomes despite delayed evacuation using resource-limited treatment strategies. We present 2 cases of frostbite treated with rt-PA at K2 basecamp to illustrate feasibility and important considerations.
Introduction
Even with today’s advances in improved outdoor clothing, preventive efforts, and medical management, severe frostbite still occurs, often resulting in catastrophic amputations. The risk of amputation is particularly high when injuries occur in the austere environment, where resources are limited. Groups at increased risk include winter recreationists such as alpinists, skiers, snowmobilers, and polar travelers, as well as those working or assigned to cold-weather operations, including the military. The main reason for poor outcome in this environment is usually delay in definitive care, which is often unavoidable. The emerging use of thrombolytics and iloprost offers the first major advances in the treatment of frostbite in decades and has reduced the rate of amputation. However, these therapies have been confined to hospital use. Given the remote locations in which many of these injuries occur, and the urgency of timely treatment, serious consideration should be given to employing these treatments in the prehospital setting under certain conditions. In this article, we discuss the field management of severe frostbite, and the indications, risks, and methods for use of thrombolytics or prostacyclin by a trained physician. We also suggest the possible adjunctive therapies of oxygenation at high altitude, and peripheral nerve block.
Field Management of Frostbite
Field treatment of frostbite remains challenging for several reasons. First is the difficulty of assessing the severity of injury, a crucial determination that dictates management and evacuation decisions. Second is determining the time of onset of injury, duration of freezing, and time since thawing in those who have spontaneously thawed. Other difficulties include the logistics of evacuation to an appropriate facility, and the presence of comorbid conditions such as hypothermia, trauma, or medical illness. In addition, treatment greatly depends on medical capabilities and available supplies, a factor that has not previously been adequately considered in treatment algorithms for field management of frostbite. Finally, the most promising therapies for severe frostbite have been confined to hospital use and are unavailable, impractical, or inappropriate for field use. Tragically, too many patients reach the hospital too late for successful use of medical therapy.
Evaluation of the severity of the injury and amputation risk
In both the field and hospital, evaluation of frostbite injury is based on presence or absence of perfusion after rewarming, combined with extent of nonperfused tissue. For assessing perfusion, careful examination includes skin color and temperature, sensation, pulses, and capillary refill. Expedition basecamps or field clinics as well as hospitals may have fast-response infrared thermometers, pulse oximeters, and even Doppler devices. The newer high-frequency Doppler devices offer marked improvement for assessing perfusion, and are used to assess microcirculation intraoperatively and in various grafts and flaps.1,2 Handheld battery-powered models are available. Level of nonperfusion or discoloration can be described with the usual hand/foot anatomy of joints: metacarpophalangeal, proximal interphalangeal, distal interphalangeal, or tuft. A number of classification systems may be used to evaluate severity.3,4 We offer a practical classification of frostbite injuries in the Figure, with details in a previous publication.
5
Although bone amputation risk depends on lack of perfusion to the bone, which cannot be determined in the field, soft tissue ischemia and cyanosis are surrogate markers for amputation risk, although not at the same level. That is, the eventual level of bone amputation is always distal to the boundary between normal color and cyanotic discoloration of the digit. After rewarming, a digit with cyanosis that extends proximal to the proximal interphalangeal joint must be considered at high risk for amputation distal to that joint; the greater the extent of cyanosis, the greater the risk of amputation (Figure). At high altitude, the risk of poor outcome may increase due to hypoxemia (Sp
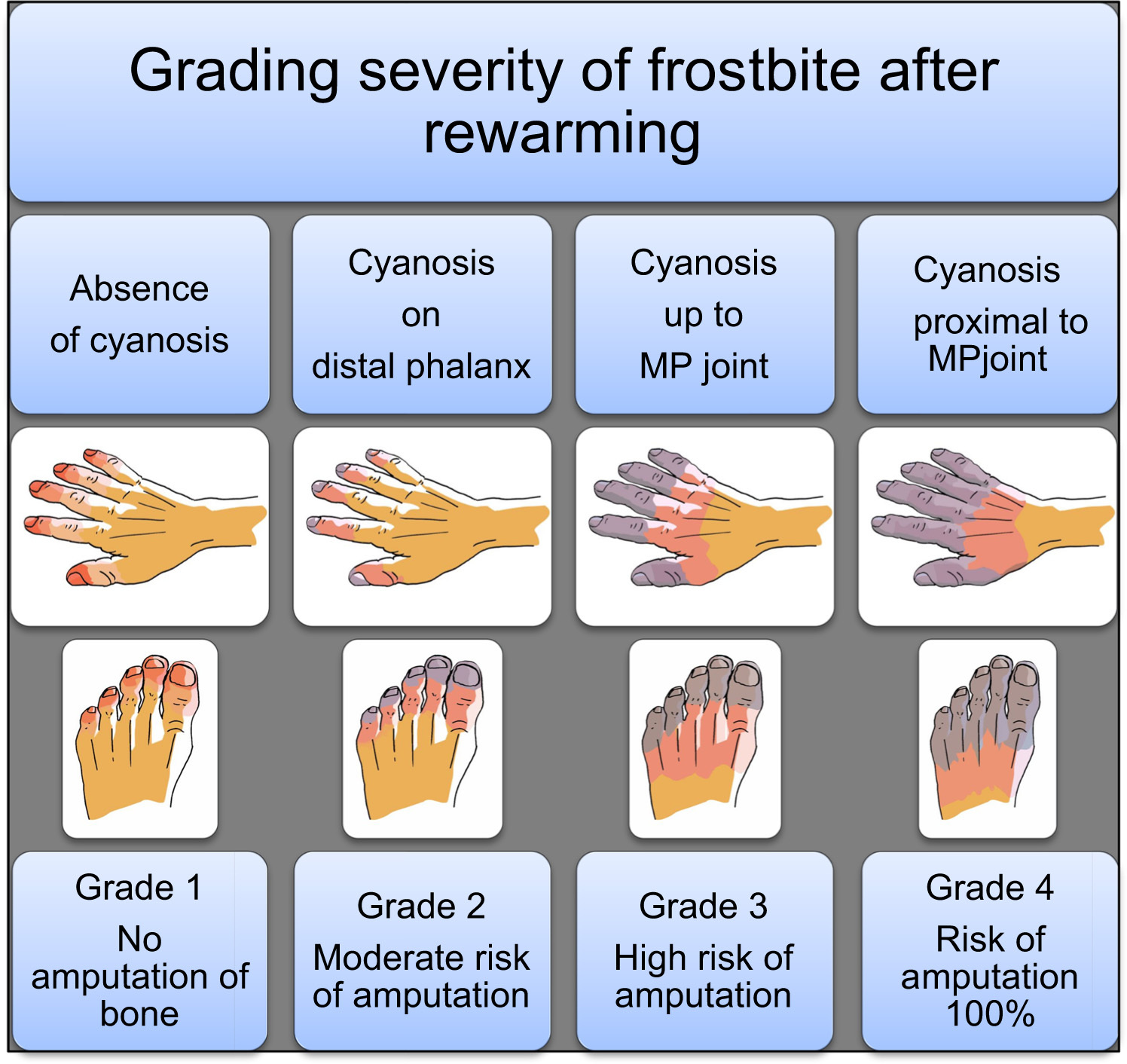
Grading severity of frostbite and bone amputation risk after rewarming.
Basic field care
A recent publication of frostbite management guidelines includes several important treatments for use in the field. 7 For example, the individual should rehydrate orally with warm fluids, and the injured extremity should be rewarmed by immersion in a 37 to 39°C water bath if there is low risk of refreezing. In order to treat hyperviscosity and inflammation, the guidelines recommend 12 mg/kg/day of ibuprofen, and others recommend aspirin. 8 In addition, low molecular weight dextran is a grade 2C recommendation for use when thrombolytics or iloprost are not going to be used. However, low molecular weight dextran is of questionable value and can cause anaphylaxis; we do not recommend it. If blisters appear, a dressing is suggested. Systemic antibiotics should be considered for severe frostbite (grades 3−4) in special circumstances. Others have suggested that for foot frostbite, anticoagulants should be considered to avoid the complications of thrombosis and phlebitis, especially if the individual is nonambulatory. 9
Recently, 2 new ideas for field treatment have been suggested but not yet studied: prehospital distal sympathetic nerve block, and increased oxygenation for frostbitten patients who are at high altitude, or hypoxic for any reason.10,11
Locoregional anesthesia (peripheral nerve blocks)
Extensive literature, primarily in hand surgery, confirms that upper extremity sympathetic nerve blocks cause vasodilation and increased skin temperature of the fingers. 12 Whether this would produce similar results in frostbitten hands or fingers is unknown but has been suggested. 13 –15 Cervical, axillary, and brachial nerve blocks and intra-arterial (IA) vasodilators have been used for frostbite treatment previously, but without controlled trials, and only in hospitals.16,17 The results have been mixed, and the Wilderness Medical Society guidelines do not recommend sympathectomy because of insufficient evidence. However, it is possible that very early intervention with sympathetic blockade in the field may be more effective. Pasquier et al recently described a simple technique that was used for field care of grade 2 bilateral hand frostbite in an alpinist. Bilateral nerve blocks were performed just proximal to the wrist with ropivacaine. 10 Pain in both hands was completely relieved in 10 minutes and recovery was excellent, without amputation. This technique deserves proper study and may be considered in the field treatment of grades 2 to 4 frostbite, for both pain control and vasodilation, by those competent in the procedure.
Oxygenation or portable recompression chamber
Whether increasing arterial oxygenation in hypoxic persons at high altitude (Sp
Thrombolytic and vasodilator pharmacological treatment
In the hospital, after rehydration, rewarming, and addressing tetanus status, several different therapeutic approaches may be considered. Thrombolytic protocols using streptokinase, urokinase, or more recently recombinant tissue plasminogen activator (rt-PA) by intravenous (IV) or IA route have been successfully implemented and published, although not yet validated by randomized controlled trials. 21 –26 Although IA rt-PA requires invasive angiography and is thus limited to certain facilities, thrombolysis with intravenous rt-PA is already used in prehospital care in many countries for myocardial infarction. The incidence of serious bleeding complications when used for acute myocardial infarction is less than 1%. 27 When given in cases of stroke mimics, the symptomatic intracranial hemorrhage rate is about 1%. There is no evidence that IV administration has greater risk compared with IA in treatment of peripheral arterial occlusion. 28 Limited data suggest that to be most efficacious in frostbite, rt-PA should be administered within 6 to 24 hours of rewarming. 21 ,22,24,29,30
Iloprost was used in 6 subjects in 2 case reports, and a recent randomized controlled trial with 47 subjects found that IV iloprost is effective in reducing amputations up to 48 hours after rewarming and has a much better safety profile than rt-PA. 31 –33 The patient receiving iloprost must be supine to avoid postural hypotension. Side effects include flushing, headaches, nausea, and occasionally vomiting; therefore, the fasting state is preferred. Serious adverse reactions are uncommon; in 81 treatments in Chamonix, infusion had to be stopped only 3 times, once for palpitations and twice for vomiting. To date, iloprost has not been used out of the hospital. Medical or surgical sympathectomy has yielded mixed results and seems to be more useful in managing long-term sequelae.34,35 Hyperbaric oxygen therapy has been used sporadically, has not yet been studied in controlled trials, and is not recommended in current guidelines for lack of sufficient data. 7
A key issue is proper patient selection for thrombolytics or prostacyclin treatment. Duration of injury and thawing may be critical. Although some authors have suggested that digits frozen for more than 24 hours precludes aggressive therapy, 27 we recommend using time from thawing rather than freezing duration for management decisions; we are in agreement with recent guidelines and other experts.5,22 In reality, the duration of freezing is often very difficult to determine. Patients may recall when their digits became numb, for example, but time of actual freezing is usually unclear. Given the terrible impact of amputations, and the chance of better results with aggressive treatment, we do not recommend duration of freezing beyond which treatment would be considered absolutely unnecessary or futile. The emerging data on use of thrombolytics suggest that there is little value when used more than 24 hours after thawing, while prostacyclin was useful up to 48 hours after thawing.5,31 Other factors in patient selection have to do with comorbidities and contraindications to thrombolytics or prostacyclin use (Tables 1 and 2).
Protocol for intravenous rt-PA
rt-PA, recombinant tissue plasminogen activator; IV, intravenous; BP, blood pressure; HAPE: high altitude pulmonary edema; HACE: high altitude cerebral edema.
Protocol for intravenous prostacyclin
HR, heart rate; BP, blood pressure.
Transitioning new therapies from the hospital to the field also must take into account the available resources and skills of the provider. These therapies require monitoring capabilities, familiarity with the medications and their possible complications, and the use of some specialized equipment, such as a syringe pump. They are thus more suited for large expedition basecamps and field clinics with medical expertise, rather than small groups with more limited resources. Although it would be impractical for rescue groups to start prostacyclin or rt-PA during rescue or evacuation, it may be possible for a well-equipped and staffed team that has reached a patient but then is faced with delayed evacuation.
Considering that rapid evacuation to hospitals remains impractical in many remote areas, we propose here a novel field treatment pathway that incorporates the recent advances in frostbite treatment. This pathway is dichotomized based on the medical training of the care providers.
Practical approach in the field
Treatment by persons with limited medical background
Basic care
All the traditional actions to correct or maintain core temperature and stabilize the individual should be taken, including obtaining shelter from the elements. Wet clothes and boots should be removed when practical. The individual should be given warm fluids and dry clothing or a sleeping bag if available. Rubbing the affected part is not recommended because of the potential for worsening direct tissue injury. See recent guidelines for details of basic care. 7
Warm water immersion
If the affected tissue is still frozen or partly frozen, if refreezing is not a risk, and the equipment is available, the affected extremities should be immersed in a 37 to 39°C water bath as soon as possible. Immersion should last 30 to 60 minutes or until a red/purple color appears on the skin, and distal flushing is maximal.
Other rewarming methods
If rapid rewarming in a water bath is not possible, digits can be rewarmed by placing them on another’s warm skin, such as in the axilla or groin, or with the use of hand warmers or heat packs. Although these devices are used commonly for prevention of cold injuries and to improve comfort of hands and feet, their use in frostbite has not been evaluated, and caution is warranted because of lack of temperature control and possible skin trauma. Other heat sources such as fire, electrical heaters, and ovens are discouraged because of risk of thermal injury. 7 There are often delays in diagnosis of frostbite and by the time of diagnosis, spontaneous thawing has often occurred. In such cases, rapid warming may not be as important, but it offers a chance to maximize vasodilatation and to clean the injured area; therefore, we recommend it.
Evaluation
After initial assessment and basic care, and after rapid rewarming if that was employed, we suggest grading the severity of frostbite according to the Figure.
Medication
If not contraindicated (allergy, active ulcer disease), 75 to 81 mg of aspirin or 400 to 600 mg of ibuprofen 2 to 3 times a day (or 12 mg/kg/day) should be given for its antiprostaglandin and analgesic effect. 30 Analgesics may be required on an individual basis (paracetamol, tramadol, opiates).
Oxygen or hyperbaric therapy
At high altitude when arterial oxygen saturation is less than 90% (usually ≥4000 meters) oxygen or a hyperbaric device might be considered if available.
36
Supplemental oxygen can be titrated to maintain Sp
Treatment by persons with medical capabilities
In addition to the basic treatment recommended for nonmedical personnel, several other medications can be considered. Although not proven effective for frostbite, calcium channel blockers and PDE-5 inhibitors are vasodilators that provide significant benefit in Raynaud’s phenomena and are often available in field medical kits, especially at high altitude. 37 –40 Authors recommended various regimens. A reasonable dosing schedule is sildenafil 50 to 100 mg twice a day, tadalafil 10 mg twice a day, or nifedipine 30 mg slow release twice a day; these medications should not be combined. Some patients may also require narcotic analgesics during or after rewarming. An injectable nonsteroidal anti-inflammatory drug, such as ketorolac, may provide quicker onset of action than oral ibuprofen, avoid nausea and vomiting, and may be especially useful if the individual’s digits are still frozen upon presentation, because nonsteroidal anti-inflammatory drugs have been shown in animal models to preserve frostbitten tissue if given before thawing.
rt-PA
Physicians can consider using intravenous rt-PA in the field when dealing with frostbite that will clearly result in amputation if untreated (grade 4), especially in the hands, and with multiple digits. The dose and considerations for its use are in Table 1.
Should any suspicion of severe trauma, intracranial or clinically significant hemorrhage occur in the field, the infusion should be discontinued. Managing a hemorrhagic thrombolysis-associated complication in the field would be challenging, as it is even in an in-hospital setting. Antifibrinolytic agents may be considered in this situation (eg, tranexamic acid 1 g). Angioedema, an occasional complication of rt-PA thrombolysis (1.3%−5%), should be treated with antihistamine and corticosteroid. 41
Iloprost infusion
Iloprost is a synthetic analogue of prostacyclin PGI2. It dilates systemic and pulmonary arterial vascular beds and also affects platelet aggregation
Iloprost is most commonly used for pulmonary arterial hypertension, scleroderma, and Raynaud’s phenomenon. It is available in inhaled and IV forms, but is not available in the IV form in many countries, including the United States. Whether the inhaled form may be useful for the peripheral circulation is unknown and requires investigation. Only the IV form has been used for frostbite to date. Because iloprost entails less risk than rt-PA, it should be considered for grades 2 to 4 frostbite, especially in the hands. In such cases, a trained medical practitioner with emergency skills can initiate field iloprost treatment if blood pressure monitoring and a portable syringe pump are available. Such equipment should be made available in expedition basecamps, field clinics for the military or commercial operations, and local health care clinics in remote areas where evacuation is likely to be delayed. In our study over 22 years there were no severe side effects, although a transitory drop of blood pressure, headaches, and vomiting are possible. 33 See Table 2 for details of administration. When diluted to 25 mL solution, an hourly rate of infusion is used (Table 2). An alternative is to start with 0.5 ng/kg/min and increase every 30 minutes by 0.5 ng/kg/min up to 2 ng/kg/min. If the patient develops unacceptable side effects, the rate is then reduced by 0.5 ng/kg/min. The infusion with either protocol is continued until the contents of 1 vial are consumed (50 mcg iloprost per vial). That is, all patients received a total of 50 mcg iloprost, regardless of weight, usually over 5 to 6 hours; the exact time depends on tolerance of infusion rate. The patient should be evacuated after this 1 dose. However, if the patient remains in the field, ideally the dose should be repeated each day for a total of 3 days Because the first dose seems to be the most important, it should be given even if further doses are not possible. In contrast to thrombolytics, iloprost can be used when there is a history of moderate trauma or when the thawing occurred over 24 hours ago (in our experience, up to 48 hours postthaw). Analgesic medication for headaches and antiemetics is sometimes necessary.
We present 2 case histories of climbers treated for frostbite at K2 basecamp by one of the authors (EFM).
Patient 1
A 42-year-old man made an open bivouac at 7400 meters after summiting K2. During the night, he awoke to find there was no glove on his left hand. He descended to base camp wearing a glove and was evaluated approximately 14 hours after the start of his bivouac. Exact time of freezing and thawing was unknown; the hand had spontaneously thawed by the time he reached basecamp. Examination revealed grade 3 frostbite with purplish discoloration of the fingers of the left hand, to between the metacarpophalangeal and proximal interphalangeal joints. All the fingers were moderately swollen. No sensation and no capillary refill were detected in any of the digits. Although it was already thawed, the physician warmed the hand in water at 39°C for 3 hours. Between 30 and 60 minutes of warming, the physician established an IV and administered 5 mg IV morphine sulfate, 5 mg IV diazepam (for agitation), and 800 mg ibuprofen orally. At 90 minutes of warming, he administered intravenous rt-PA, 1.4 mg/kg over 15 minutes, followed by intravenous heparin 1000 units per hour for 4 hours. No topical medications were applied. There were no immediate or late complications, and recovery was excellent. At follow-up in Europe, he had only sloughing of superficial skin.
Patient 2
A 40-year-old male climber sustained frostbite of both feet after reaching the summit of K2. He presented at basecamp 2.5 days later, 60 to 66 hours after freezing; the feet had thawed during descent, exact timing unknown. Examination showed grade 4 frostbite, with discoloration and swelling of all toes into the midmetatarsals of both feet, with no capillary refill or sensation to the ankles. He was treated exactly the same as Patient 1. Several days later, he returned to Europe and all toes were eventually amputated. No complications of thrombolytic therapy were observed either immediately or late.
Comment
Thrombolytic therapy was utilized safely at K2 basecamp. Although the dosage of rt-PA was slightly different from current recommendations, these cases demonstrate that its use is feasible in this extreme environment. Although only 2 patients were treated, it is reassuring that there were no complications. The therapy likely prevented amputations for Patient 1, while Patient 2 was probably outside the therapeutic window of 24 hours after thawing and there was no benefit of thrombolytic therapy. These case examples should help encourage the use of thrombolytics therapy in the field, when the risk of amputation is high, no contraindications are present, and the physician is familiar with the therapy. We hope there will soon be a report of frostbite injury in the field with prostacyclin.
Conclusion
In cases of severe frostbite with delayed evacuation, the choice of treatment depends on 3 parameters: the severity of frostbite, the resources available, and the medical experience of the provider. Basic care including rewarming and ibuprofen or aspirin administration can be dispensed in the field. Oxygen or portable recompression chamber may be useful at very high altitudes by any rescuer. Other management options for experienced or trained physicians include thrombolytics or prostacyclin infusion, and locoregional anesthesia. Because of the risk of complications, rt-PA should only be used for severe and extended frostbite (grade 4) rewarmed within 24 hours, while prostacyclin, being safer, can be used for up to 48 hours postthawing in grades 2 to 4 frostbite. Introduction of these new therapies for field use will likely result in fewer amputations, and studies assessing these treatments will hopefully be forthcoming.
Footnotes
Presented at the 19th International Hypoxia Symposium, March 4, 2015, Lake Louise, Canada.