
Abstract
Objective
Pre-exertion skeletal muscle glycogen content is an important physiological determinant of endurance exercise performance: low glycogen stores contribute to premature fatigue. In low-oxygen environments (hypoxia), the important contribution of carbohydrates to endurance performance is further enhanced as glucose and glycogen dependence is increased; however, the insulin sensitivity of healthy adult humans is decreased. In light of this insulin resistance, maintaining skeletal muscle glycogen in hypoxia becomes difficult, and subsequent endurance performance is impaired. Sympathetic inhibition promotes insulin sensitivity in hypoxia but may impair hypoxic exercise performance, in part due to suppression of cardiac output. Accordingly, we tested the hypothesis that hypoxic exercise performance after intravenous glucose feeding in a low-oxygen environment will be attenuated when feeding occurs during sympathetic inhibition.
Methods
On 2 separate occasions, while breathing a hypoxic gas mixture, 10 healthy men received 1 hour of parenteral carbohydrate infusion (20% glucose solution in saline; 75 g), after which they performed stationary cycle ergometer exercise (∼65% maximal oxygen uptake) until exhaustion. Forty-eight hours before 1 visit, chosen randomly, sympathetic inhibition via transdermal clonidine (0.2 mg/d) was initiated.
Results
The mean time to exhaustion after glucose feeding both with and without sympathetic inhibition was not different (22.7 ± 5.4 minutes vs 23.5 ± 5.1 minutes; P = .73).
Conclusions
Sympathetic inhibition protects against hypoxia-mediated insulin resistance without influencing subsequent hypoxic endurance performance.
Introduction
Pre-exertion skeletal muscle glycogen content is a determinant of endurance exercise performance 1 ; low glycogen stores contribute to premature fatigue, whereas high glycogen promotes and extends performance. In low-oxygen environments, the contribution of carbohydrates to endurance performance is further enhanced as glucose and glycogen dependence is increased. In hypoxia or hypobaria, insulin sensitivity is decreased markedly in healthy adult humans. 2 –4 In light of this insulin resistance, maintaining skeletal muscle glycogen in high altitudes becomes difficult; thus, subsequent endurance performance is impaired. Low-oxygen–mediated activation of the sympathetic nervous system may contribute to high-altitude insulin resistance, in part via glycogenolysis, lipolysis, and inhibition of hexokinase and insulin receptor substrate-1–associated phosphatidylinositol 3-kinase. We have demonstrated that sympathetic inhibition with the centrally acting α2-adrenergic receptor agonist, clonidine, attenuates hypoxia-mediated insulin resistance. 4 This implies that sympathetic inhibition may be an effective strategy to abrogate high-altitude insulin resistance and thus promote skeletal muscle glycogen maintenance and endurance performance in low oxygen. However, the sympathetic nervous system is also a powerful regulator of cardiopulmonary function, and sympathetic inhibition in hypoxia may actually impair endurance exercise performance via decreased cardiac output and oxygen delivery. The purpose of the current investigation was to examine the hypothesis that the metabolic benefits of sympathetic inhibition outweigh the cardiopulmonary decrement as they pertain to endurance exercise performance in hypoxia after carbohydrate feeding.
Methods
Ten men participated in this study. Inclusion criteria included age within the range of 18 to 40 years and body mass index ranging from 18.5 to 30 kg/m2; freedom from overt disease based on medical history, assessment of blood pressure, and 12-lead electrocardiogram at rest and during incremental exercise; and physician approval. Exclusion criteria included current use of tobacco or medications, history of acute mountain sickness, pulmonary dysfunction, and contraindications to vigorous exercise, as per the American College of Sports Medicine. The institutional review board at Colorado State University approved the protocol. The purpose and risks of the study were explained to research participants before written informed consent was obtained.
Overview
After screening, participants reported to the laboratory on 2 separate occasions; 48 hours before 1 of these visits, transdermal administration of clonidine was initiated. The study visits occurred in random order and began with 1 hour of parenteral carbohydrate feeding, after which participants performed moderate-intensity cycle ergometer exercise until exhaustion. Throughout the entirety of each visit, including the exercise component, participants breathed a hypoxic gas mixture.
Screening and Habituation
Body composition (dual-energy x-ray absorptiometry; Lunar Radiation Corp, Madison, WI; software v. 4.1) and maximal oxygen uptake (V
Experimental Procedures
After screening and protocol habituation, participants reported to the laboratory on 2 separate occasions, after an overnight fast and 48-hour abstention from vigorous physical activity. On arrival, participants were instrumented for measurement of heart rate (3-lead electrocardiogram), blood pressure, and oxyhemoglobin saturation (Cardiocap 5, GE Datex-Ohmeda, Madison, WI). Heart rate and systolic blood pressure were used to calculate the rate pressure product. After a brief period of semirecumbent rest, heart rate, blood pressure, and oxyhemoglobin saturation were recorded. Participants were then fitted with a face mask (7450 Series; Hans Rudolph, Inc, Shawnee, KS) attached to a 3-way, nonrebreathing valve (2730 Series; Hans Rudolph, Inc) and connected to a 100-L nondiffusing gas bag (6000 Series; Hans Rudolph, Inc) filled with precision mixed gases (15% O2, balance N; Airgas, Denver, CO). After 15 minutes, heart rate, blood pressure, and oxyhemoglobin saturation were recorded again. Glucose (20% glucose solution in saline; 75 g) was intravenously administered for 1 hour, after which the participants rested quietly for 3 hours before the time-to-exhaustion trial. Consistent with the habituation protocol, this entailed stationary cycle ergometer exercise at 65% of normoxic V
To determine the influence of sympathetic inhibition on exercise performance in hypoxia after parenteral carbohydrate feeding, during the 48 hours before 1 of the visits, transdermal clonidine (Catapres-TTS; 0.2 mg/d) was administered. Clonidine administration continued until initiation of the glucose infusion. Clonidine is an antihypertensive; the mechanism of action is via prejunctional α2-adrenergic receptor stimulation. Short-term clonidine use results in centrally mediated peripheral sympathetic inhibition, as reflected by attenuated skeletal muscle–sympathetic nerve activity, 6 decreased norepinephrine release,4,6 and increased heart rate variability. The plasma half-life of clonidine is 21 hours; therapeutic plasma concentrations are usually achieved within 48 hours of initiation of transdermal administration. 7
Statistical Analysis
One-way repeated measures analysis of variance was used to determine the influence of sympathetic inhibition on exercise time to exhaustion after carbohydrate feeding. Statistical significance was set at P < .05. Data are expressed as mean ± SE.
Results
As a group, the participants were of normal weight, based on body mass index, and of average aerobic fitness, based on V
Select characteristics of research participants a
Data are mean ± SE.
Resting hemodynamic responses to hypoxia with and without clonidine a
DBP, diastolic blood pressure; HR, heart rate; SBP, systolic blood pressure; Sp
Data are mean ± SE.
Different from normoxia (P < .01).
Different from control (P < .05).
Significant interaction between hypoxia and clonidine (P = .009).
Basal Response to Hypoxia
Compared with measurements made in normoxia, oxyhemoglobin saturation was decreased in hypoxia (P < .001), but heart rate was increased (P = .003). Hypoxia decreased systolic blood pressure (P = .041) but did not affect diastolic blood pressure (P = .741).
Basal Response to Clonidine—Evidence of Sympathetic Inhibition
Clonidine administration was associated with decreased systolic (P = .037), diastolic (P = .023), and mean arterial (P = .015) blood pressure in normoxia. Oxyhemoglobin saturation was unaffected.
Basal Response to Clonidine and Hypoxia—Evidence of Sympathetic Inhibition
Clonidine was associated with decreased systolic (P = .009) and diastolic blood pressure (P = .023). Clonidine was also associated with decreased mean arterial pressure (P = .015) and rate pressure product (P = .024) in hypoxia (Figure 1). Clonidine did not influence the effect of hypoxia on oxyhemoglobin saturation (P = .275).
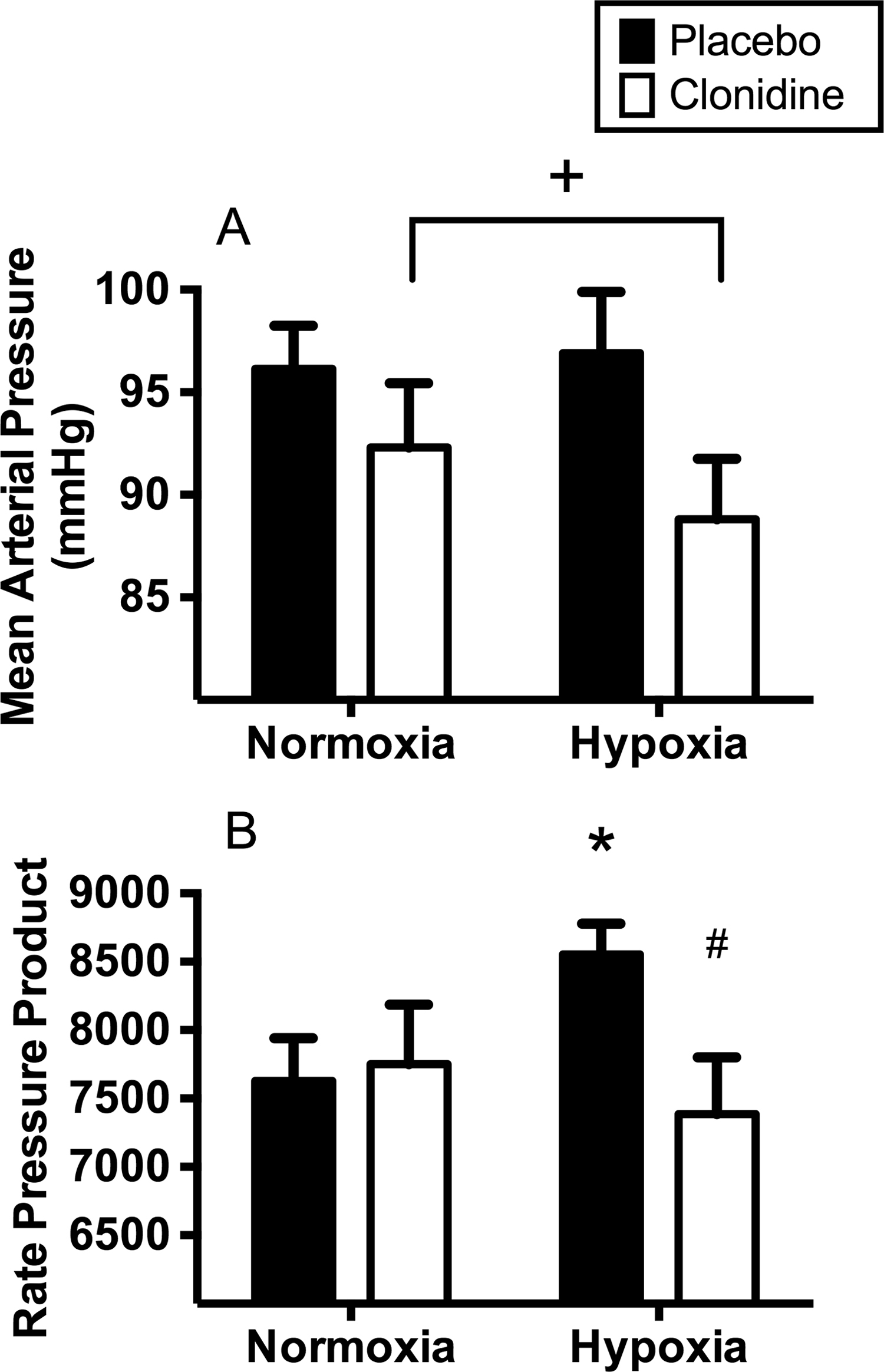
Mean arterial pressure (A) and rate pressure product (B) at rest with (white bars) and without (black bars) prior clonidine administration in normoxia and hypoxia. Data are mean ± SE. +Main effect of clonidine (P = .015). *Different from normoxia control (P = .028). #Different from hypoxia control (P = .024).
Endurance Exercise Performance
There was no difference in time to exhaustion with and without clonidine administration (Figure 2; P = .73). The difference between the conditions was 49.2 ± 2.3 seconds; the average work rate was 177 ± 8 W. Four of the 10 participants extended their time to exhaustion with clonidine use (magnitude of increase in time to reach volitional exhaustion was >1 minute), whereas an equal number of participants demonstrated fatigue earlier (magnitude of decrease in time to exhaustion was >1 minute). The magnitude of difference between conditions for the remaining 2 participants was <1 minute. During exercise there was no effect of clonidine on heart rate (control 165 ± 3 beats/min vs clonidine 163 ± 3 beats/min; P = .484) or oxyhemoglobin saturation (control 69% ± 3% vs clonidine 74% ± 2%; P = .145). There was no effect of clonidine on perceived effort during the time-to-exhaustion test (control 18 ± 0 vs clonidine 18 ± 3; P = .645).
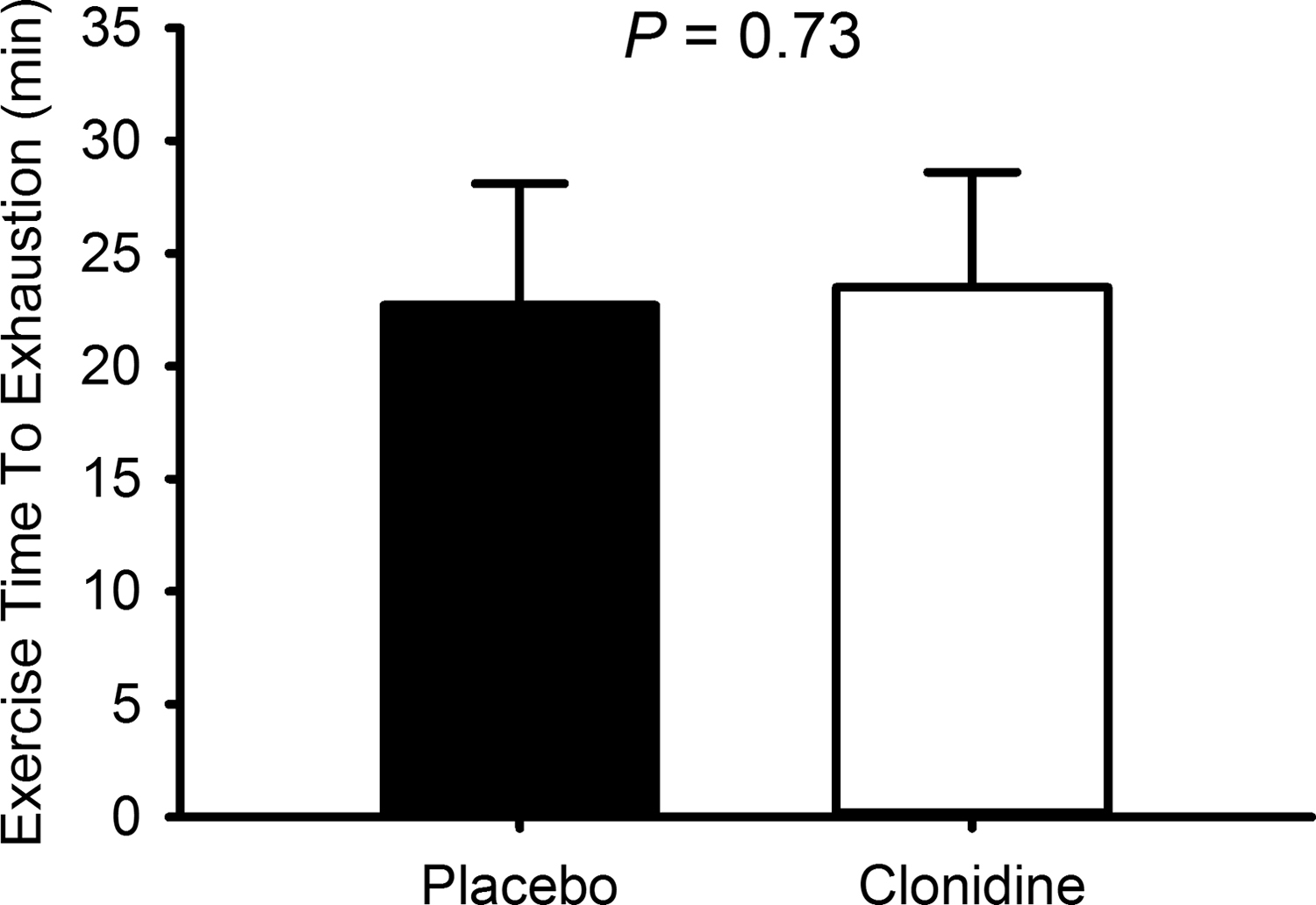
Cycle exercise time to exhaustion in hypoxia after the intravenous glucose infusion with (white bars) and without (black bars) prior clonidine administration. Data are mean ± SE.
Discussion
We have addressed the question of whether the metabolic benefits of sympathetic inhibition outweigh the cardiopulmonary decrement as they pertain to endurance exercise performance in hypoxia after carbohydrate feeding. The novel finding of our investigation was that sympathetic inhibition does not extend time to exhaustion during exercise in hypoxia, but importantly, it does not inhibit exercise performance either. We suggest that, although sympathetic inhibition may inhibit cardiopulmonary function, this may be offset by improved glucose regulation.
In light of the critical role of skeletal muscle glycogen during exercise and the increased reliance on carbohydrates during exercise in hypoxia and hypobaria, pre-exertional glucose regulation and glycogen synthesis in low-oxygen environments are of obvious interest, especially in the context of sympathetically mediated hypoxia-induced insulin resistance. 2 –4 In this regard, the influence of the carotid bodies on metabolic regulation has fallen under increased scrutiny. Traditionally considered from the sole perspective of cardiopulmonary regulation via chemoreceptors, recent studies have demonstrated that carotid bodies are sensitive to changes in circulating glucose and insulin, 8 and surgical resection or inhibition of carotid bodies prevents high-fat diet–induced insulin resistance 9 and lowers sympathetic activity while augmenting insulin sensitivity. 10 Collectively, these observations might support the use of supplemental oxygen to promote or maintain metabolic health at high altitude; however, this is often an impractical strategy. Alternatively, a pharmacological approach to inhibit the sympathetic nervous system and improve glucose regulation may have merit. We have previously shown that sympathetic inhibition with clonidine attenuates hypoxia-mediated insulin resistance. 4 Therefore, clonidine administration before prolonged hypoxic exposure could promote physiological function by augmenting insulin sensitivity and facilitating the maintenance of skeletal muscle glycogen stores.
Conversely, during exercise, the sympathetic nervous system plays a vital role in physiological regulation, contributing to cardiopulmonary function and substrate mobilization and delivery. Accordingly, sympathetic inhibition during exercise in hypoxia may seem counterintuitive. Previous studies have demonstrated impaired cardiac output and exercise performance with sympathetic inhibition. In the current study, we inhibited the sympathetic nervous system for 48 hours before hypoxic parenteral glucose feeding and subsequent hypoxic endurance exercise. When considered in the context of our previous study, our current data suggest that although 0.2 mg/d of clonidine for 48 hours is sufficient to attenuate hypoxia-mediated insulin resistance and promote glucose regulation, 4 this degree of inhibition may not be potent enough to inhibit endurance performance in hypoxia. That is, during hypoxic exercise, increased sympathetic drive may be sufficient to overcome the inhibitory actions of the administered clonidine dose. In support of this, during clonidine administration, resting blood pressure and rate pressure product were reduced; during exercise, heart rate and time to fatigue were unaffected. Future studies of an alternative sympathetic inhibitor would determine whether this response was specific to clonidine.
There are several potential limitations in the current study that warrant brief discussion. First, although we have indirect evidence to support a sympathoinhibitory effect of clonidine (eg, lower blood pressure), we did not confirm improved glucose regulation in hypoxia. However, based on consistent data from 3 laboratories,4,9 there is no reason to suspect that clonidine did not facilitate hypoxic glucose regulation. Second, participants did not complete an exercise trial in normoxia; thus, we were unable to compare our hypoxic data with a normoxic control. The detrimental effects of hypoxia on endurance performance are well established with more than 50 years of research. Accordingly, we did not believe burdening our participants with an additional exercise trial was warranted. Third, this was an open-label study; the research participants were not naïve as to clonidine vs control. This decision was based on our past experiences with clonidine. In 2 separate studies,4,6 all research participants correctly distinguished clonidine from placebo. Although it is plausible that participants’ expectations may have influenced the primary outcome, the research participants were not provided with a full explanation of the study rationale; that is, clonidine was presented as neither ergogenic nor ergolytic. Finally, all of the participants in the study were residents of Fort Collins, CO, situated at an altitude of approximately 1500 m. Thus, it is possible that, as a result of acclimatization, the influence of hypoxia on glucose regulation or exercise performance may have been less than that of a sea level–dwelling adult. We believe this is unlikely and that the exposure to hypoxia was physiologically significant based on the magnitude of the decrease in oxyhemoglobin saturation.
In conclusion, sympathetic inhibition via clonidine administration did not favorably or adversely impact endurance exercise performance in hypoxia after carbohydrate feeding. Our data may be interpreted to suggest that the metabolic benefits of sympathetic inhibition with respect to hypoxia-induced insulin resistance may outweigh the potential decrement to cardiopulmonary function. This exploratory study examined the potential of a metabolic rather than a traditional cardiopulmonary strategy to promote hypoxic exercise tolerance. The neutrality of our data does not rule out the need for future explorations of integrative, multisystem strategies for facilitating endurance performance in hypoxia.
Footnotes
Funding
The Defense Advanced Research Projects Agency provided support.