
Abstract
Wild mushroom poisoning is often reported to cause acute liver or renal failure. However, acute rhabdomyolysis caused by wild mushroom poisoning has rarely been reported. We describe 7 patients of 1 family with Russula subnigricans Hongo poisoning. Their clinical manifestations varied from gastrointestinal symptoms to rhabdomyolysis, with 1 fatality. Our report provides supporting evidence that rhabdomyolysis may result from ingestion of R subnigricans mushrooms. A key to survival for patients with rhabdomyolysis caused by R subnigricans poisoning may be early recognition and intensive supportive care.
Introduction
More than 2000 species of mushrooms found worldwide are safe for human consumption, but there are also many wild mushrooms that are toxic. 1 In China, edible mushrooms are readily available, inexpensive, and widely consumed. Wild poisonous mushrooms may closely resemble those that are edible and can be accidentally ingested. Thus, outbreaks of wild mushroom poisoning frequently occur in rural areas of China. From 1994 to 2012, the Chinese Center for Disease Control and Prevention (CDC) reported 311 mushroom poisoning events, with 1954 poisoning cases and 409 deaths. 2
Poisoning caused by the “death cap” mushroom Amanita phalloides has often been reported. 3 It is one of the most toxic wild mushrooms in the world and can cause acute liver failure and death in humans.4,5 Cortinarius species have also been reported to cause renal failure.6,7 However, wild mushroom poisoning as the cause of rhabdomyolysis has rarely been reported. We describe a family of 7 patients poisoned by Russula subnigricans Hongo wild mushrooms. Their clinical manifestations varied from gastrointestinal symptoms to rhabdomyolysis, with 1 fatality.
Case Reports
Seven people from 1 family, including 4 women (age range, 15–51 years) and 3 men (age range, 18–58 years), ingested wild mushrooms on July 19, 2013. They were hospitalized on July 20, 2013, with nausea, vomiting, diarrhea, and dizziness. One patient had picked wild mushrooms in the forests of Shiqian county, Guizhou province, China, and all 7 patients had consumed 10 to 100 g of the mushrooms after cooking them at home, 20 hours before admission. At admission, all patients had fatigue and muscle weakness and 5 patients had myalgia, mainly in the upper parts of the legs. No fever was noted. All patients had normal blood pressure. The findings on physical examination, which included cardiopulmonary auscultation and a neurologic assessment, were unremarkable.
On admission, initial screening tests showed serum creatine kinase (CK) levels were elevated in 6 patients (Table). The median levels of CK, aspartate aminotransferase (AST), and alanine aminotransferase (ALT) were 2063 U/L (range, 126–66,950 U/L; normal, 38–174 U/L), 151 U/L (range, 24–636 U/L; normal, <40 U/L), and 32 U/L (range, 12–178 U/L; normal, <50 U/L), respectively. Coagulation tests and serum creatinine (SCr) levels were normal. Three patients had hypokalemia (range, 3.02–3.41 mmol/L; normal, 3.50–5.30 mmol/L), and 2 patients had hypocalcemia (range, 2.06–2.16 mmol/L; normal, 2.20–2.65 mmol/L).
Background data and laboratory findings of 7 patients with Russula subnigricans poisoning at the time of admission
ALT, alanine aminotransferase; CK, creatine kinase; sCr, serum creatinine; Tbil, total bilirubin.
The only patient to die; all other patients recovered.
Above normal limits.
Because 6 patients had elevated serum CK levels, rhabdomyolysis and acute myocarditis were suspected. However, the absence of abnormalities on electrocardiogram and echocardiography ruled out a cardiac origin for the increased serum levels of CK. Initially, gastric lavage was performed in all patients, together with fluid replacement. The patients were also treated with penicillin G (400,000–500,000 U/kg per day, intravenous) and silybin (silibinin; 10–20 mg/kg per day, oral).
The serum CK values in 4 of the 6 patients who survived further increased on the day after admission (Figure 1), their weakness worsened, and production of dark urine was observed; and hypokalemia (range, 3.23–3.43 mmol/L) and hypocalcemia (range, 1.88–2.16 mmol/L) were found. These 4 patients were subsequently treated with hemodialysis to prevent acute kidney injury. From the third day, their serum CK levels gradually declined to the standard range, and they experienced progressive recovery of muscle strength.
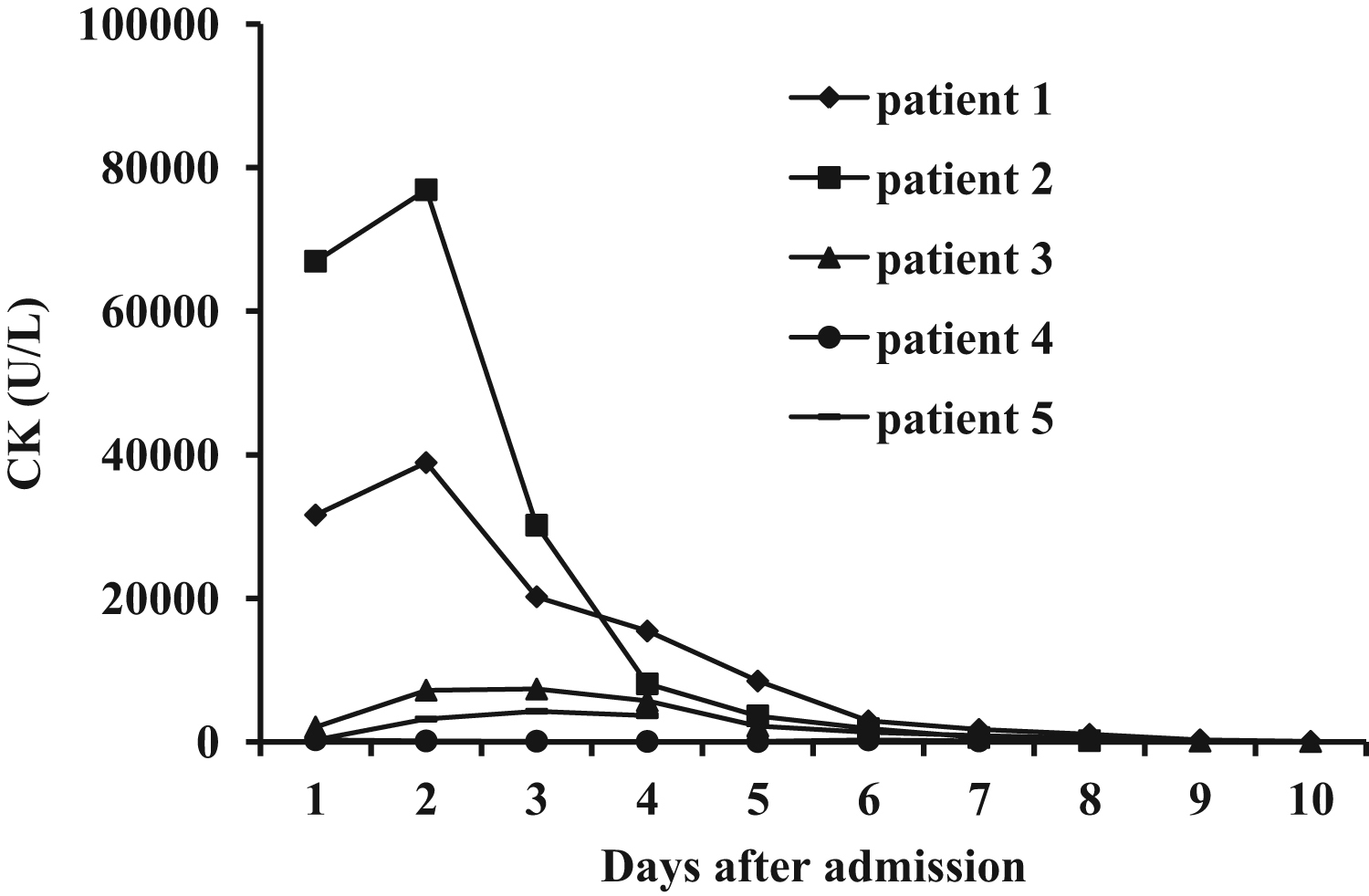
Serum creatine kinase (CK) levels in 5 patients who survived during hospitalization.
In the 1 patient who died, weakness and myalgia worsened during the first 12 hours after admission, and dark urine was also observed. Arterial blood gas values while breathing 50% inspired oxygen were a pH of 7.26, P
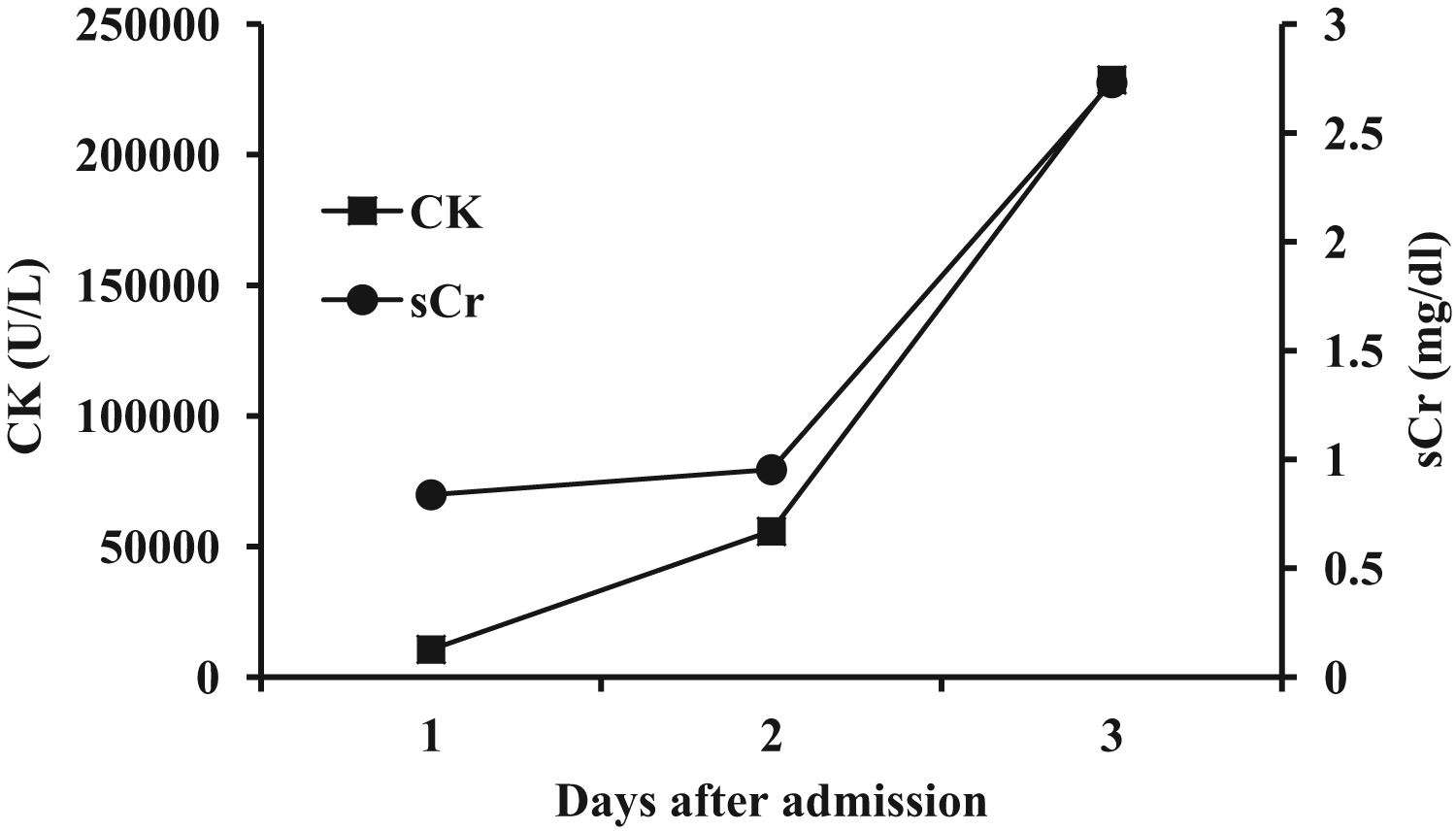
Serum creatine kinase (CK) and serum creatinine (sCr) levels in the patient who died during hospitalization.
MUSHROOM IDENTIFICATION
Mushroom samples (Figure 3) were sent to our hospital and identified as R subnigricans Hongo by a mycologist from the Mushroom Research Institute of Shanghai Academy of Agricultural Science.

Russula subnigricans mushrooms.
Discussion
The world geographic distribution of R subnigricans is not completely defined, although it has been identified in the United States, China, and Japan. In China, R subnigricans grows in several southern provinces. The mushrooms are often confused with those of the similar species Russula nigricans, which is less poisonous. The differentiating features of these 2 species are that the flesh of R subnigricans is white but turns red when damaged. The flesh of R nigricans is initially white, then red, and turns black when damaged. 8
Rhabdomyolysis is a clinical syndrome caused by severe injury to skeletal muscle, leading to the release of the intracellular muscle constituents into the circulation and extracellular fluid. The most common cause of rhabdomyolysis is muscular trauma; the other causes of rhabdomyolysis include medications, hyperthermia, toxins, infections, and endocrinopathies, 9 but neither muscle ischemia nor unconsciousness was noted before the onset of symptoms in our patients. Drug intoxication could also be ruled out because none of the patients had taken any drugs within 1 month before the onset of symptoms. The patients collected the mushrooms from the nearby mountain, and the mushrooms were carefully washed before cooking, so the possibility of contamination with pesticides as a cause of rhabdomyolysis was also ruled out. Therefore, we concluded that the rhabdomyolysis was caused by the wild mushroom R subnigricans. The individual differences in the clinical manifestations of poisoning among the patients may be related to the different amounts they ingested. The patient with normal CK level (patient 6; Table) had consumed the smallest amount of mushroom.
Examples of rhabdomyolysis caused by wild mushroom poisoning have been reported rarely worldwide. In France, large quantities of the wild mushroom Tricholoma equestre was reported to cause delayed rhabdomyolysis in 12 patients, 3 of whom died. 10 In Taiwan, an outbreak of R subnigricans poisoning was reported, in which 2 patients progressed to rhabdomyolysis, and 7 patients recovered in 1 day with supportive care at home. 8 In a recent report of 183 patients who died of mushroom poisoning from 1994 to 2012 in southern China, 24.59% of the deaths were caused by R subnigricans. However, whether rhabdomyolysis was the main cause of death in patients with R subnigricans poisoning is not known. 2 Herein, we provide further evidence that fatal rhabdomyolysis may result from wild mushroom R subnigricans poisoning. Physicians should be aware of the possibility of severe rhabdomyolysis after large quantities of R subnigricans have been consumed.
Several toxins have been found in R subnigricans. Six chlorinated phenyl ethers, designated russuphelins A, B, C, D, E, and F, were isolated from R subnigricans by Takahashi et al.11,12 Russuphelin A was cytotoxic to various solid tumor cells, and russuphelins B, C, and D were cytotoxic to P388 leukemia cells in vitro. Recently, Matsuura et al. 13 isolated the small, highly strained cycloprop-2-ene carboxylic acid from Asian R subnigricans. This compound was associated with fatal rhabdomyolysis in mice. However, whether this carboxylic acid is also responsible for fatal rhabdomyolysis in humans remains unknown.
A phalloides is the most toxic mushroom and the major cause of mortality caused by mushroom ingestion worldwide. In China, most patients with wild mushroom poisoning cannot identify the wild mushrooms they consumed. It is important for physicians to judge quickly and correctly the potential toxicity of wild mushrooms from clinical manifestations and initial laboratory examinations to give reasonable and timely treatment. However, most patients with wild mushroom poisoning have only gastrointestinal symptoms during the first 24 to 48 hours. 14 Therefore, it is currently difficult to distinguish A phalloides from R subnigricans poisoning. In the present case study, most of the 7 patients presented with obvious myalgia and elevated CK on admission, and their CK levels further increased after admission. Moreover, although their serum ALT levels increased after admission, coagulation tests remained normal. All these clinical features distinguish R subnigricans from A phalloides poisoning. However, because some patients with A phalloides poisoning may also have elevated CK levels, 15 serum CK levels cannot be used as a definitive way to differentiate R subnigricans from A phalloides poisoning.
In conclusion, the experience of this group of patients suggests that clinical presentations of patients with R subnigricans poisoning can vary from gastrointestinal symptoms to fatal rhabdomyolysis. Most of the patients with rhabdomyolysis caused by R subnigricans poisoning presented early with myalgia, accompanied by sustained increase of serum CK. A key to survival for patients with rhabdomyolysis caused by R subnigricans poisoning may be early recognition and intensive supportive care.