
Abstract
Objective
Several environmental factors including hypoxia have been reported to contribute to oxidative stress in individuals living in the highlands. However, little is known about the role of oxidized low-density lipoprotein (ox-LDL) among community-dwelling elderly in the Qinghai-Tibet plateau.
Methods
The study population comprised 168 community-dwelling elderly subjects aged 60 years or older (male to female ratio, 70:98; mean age, 65.8 years) living in Haiyan County, located 3000 to 3200 m above sea level, 30 km northwest of Xining, Qinghai. The subjects were volunteers who joined a Comprehensive Geriatric Assessment. Plasma ox-LDL was measured in 168 community-dwelling elderly subjects aged 60 years or older (23 Tibetans and 145 Hans) with a monoclonal antibody-based enzyme-linked immunosorbent assay.
Results
Mean ox-LDL level was higher among Tibetan elderly than Han elderly (Tibetan, 79.0 ± 29.6 U/L; Han, 62.8 ± 23.5 U/L; P = .003). Tibetan ethnicity was significantly associated with ox-LDL levels after adjusting for LDL cholesterol levels. In addition, high ox-LDL levels (≥70 U/L) were significantly associated with a homeostasis model assessment insulin resistance index of at least 1.6 (odds ratio [OR], 2.82; 95% confidence interval [95% CI], 1.11 to 7.15; P = .029) and ankle brachial pressure index of less than 1.0 (OR, 4.85; 95% CI, 1.14 to 10.00; P = .028), after adjusting for age, sex, and ethnicity.
Conclusions
Our findings support the hypothesis that ox-LDL levels are higher among Tibetan elderly highlanders compared with those among Han elderly. As ox-LDL levels can affect insulin resistance and arteriosclerosis, further research is needed to determine how oxidative stress influences the health situation among elderly individuals at high altitudes.
Introduction
Inspired oxygen pressure decreases with altitude. Compared with values at sea level, this pressure is roughly 89% at an altitude of 1000 m, 79% at 2000 m, 69% at 3000 m, 60% at 4000 m, and 52% at 5000 m. 1 Several environmental factors including hypoxia may contribute to oxidative stress in individuals living in the highlands.2,3 In general, ultraviolet radiation increases by approximately 4% per 300 m because of decreases in clouds, dust, and water vapour. 4 In addition, as much as 75% of ultraviolet radiation can be reflected back by snow. 4 Low temperature stress contributes significantly to oxidative stress, and temperature decreases with increasing altitude at a rate of approximately 6.5°C per 1000 m.4,5 Lower dietary intake of antioxidants such as fruits and vegetables could also result in higher levels of oxidative stress. 6 –8 Oxidative stress is widely recognized as being associated with various disorders including atherosclerosis, diabetes mellitus, hypertension, and hypercholesterolemia, to name a few. 9 –13 Many studies have pointed out the advantageous points of the Tibetan adaptation to high altitude. However, our previous study, which measured serum hydroperoxides with the Diacron reactive oxygen metabolites test (d-ROMs; Diacron, Parma, Italy), showed the Tibetan elderly had higher levels of reactive oxygen metabolites (ROM) than the Han elderly. 14 The present study aimed to investigate oxidized low-density lipoprotein (ox-LDL) level as a reliable measure of oxidative stress and its association with other cardiovascular and metabolic variables among community-dwelling elderly individuals living at high altitudes. 15 –19
Materials and methods
Subjects
Our study population comprised 168 community-dwelling elderly subjects aged 60 years or older (male/female ratio, 70:98; mean age, 65.8 years) living in Haiyan County (Qinghai, China). Haiyan County is located 3000 to 3200 m above sea level, 30 km northwest of Xining, which is the capital of Qinghai province in China. Our subjects were elderly volunteers who joined our medical and geriatric examination camp. The survey for community-dwelling elderly living in Haiyan County was conducted in August 2008.
OX-LDL Levels
In February 2009, concentrations of ox-LDL in cryopreserved plasma samples at Affiliated Hospital of Qinghai University, China, were measured by a competitive enzyme-linked immunosorbent assay (ELISA) kit using a specific murine monoclonal antibody, mAb-4E6 (Mercodia, Uppsala, Sweden). The results were interpreted in accordance with the manufacturer’s instructions. The mAb-4E6 is directed against a conformational epitope in the apolipoprotein B-100 (apoB-100) moiety of low-density lipoprotein (LDL) that is generated as a consequence of the substitution of at least 60 lysine residues of apoB-100 with aldehydes. The substituting aldehydes can be produced by peroxidation of LDL lipids, which generates ox-LDL. The results were interpreted in accordance with the manufacturer’s instructions.
Comprehensive Geriatric Assessments
Blood pressure was measured twice with the subject in a sitting position using an autosphygmomanometer (HEM 757, Omron, Japan). Hypertension was defined as 140 mm Hg or greater for systolic pressure, 90 mm Hg or greater for diastolic pressure, or if the subject was taking antihypertensive medication. Blood chemical tests were conducted twice, at fasting and 2 hours after drinking 75 g of glucose, among subjects who provided informed consent. Diabetes mellitus and impaired glucose tolerance were defined according to World Health Organization criteria. Specifically, diabetes mellitus was defined as a fasting blood sugar (FBS) of 126 mg/dL or greater or 2-hour oral glucose tolerance test (OGTT) of 200 mg/dL or greater, or if the subject was taking diabetes medication, and impaired glucose tolerance was defined as an FBS from 110 mg/dL to 126 mg/dL or an OGTT from 140 to 200 mg/dL. Insulin resistance was assessed using the homeostasis model assessment insulin resistance index (HOMA-R) and was calculated as fasting plasma glucose × fasting serum insulin / 405. 20 Blood chemical analyses were conducted in the central laboratory of Qinghai University Hospital. Ankle brachial pressure index (ABI) and the cardio ankle vascular index (CAVI) were measured using a VaSera instrument (Fukuda Denshi, Tokyo, Japan). Carotid plaques were examined by carotid ultrasound. Plaques were defined as focal structures that encroached into the arterial lumen at least 0.5 mm, comprised 50% of the surrounding intima-media thickness value, or that for which the thickness was 1.5 mm from the media-adventitia interface to the intima-lumen interface.
Ethical Approval
These surveys were approved by the Ethics Committee of the Research Institute for Humanity and Nature (2007-02) and Medical Institute of Qinghai University. Written informed consent was obtained from each subject.
Statistical Analysis
Data were analyzed with SPSS 15.0 for Windows (IBM Corp, Armonk, NY). Baseline data are presented as mean ± SE or percentages. Stepwise multiple regression analyses (to P < .05) were used to assess associations between ox-LDL and other variables. Standardized β coefficients were used, as they allow for a direct comparison of the strength of associations between ox-LDL and other variables. Any factors significant in the univariate model were used in the multivariate analysis, and a probability value of less than 0.05 was considered statistically significant. Logistic regression analysis (to P < .05) was used to assess associations between ox-LDL and geriatric variables. The logistic regression analysis incorporated covariates of age, sex, and ethnicity.
Results
Comparison of Tibetan and Han Elderly Highlanders
Our elderly study population consisted of 23 Tibetans and 145 Hans. Table 1 compares basic characteristics of Tibetan and Han elderly highlanders in Haiyan County (Qinghai province). Mean age and sex ratios did not differ significantly, but dairy product intake was higher among Tibetans. Table 2 compares cardiovascular and metabolic variables of the 2 ethnic groups. No significant difference was found in mean systolic blood pressure, oxygen saturation, hemoglobin concentration, fasting blood glucose, HOMA-R, triglycerides, high-density lipoprotein (HDL) cholesterol, CAVI, and ABI levels between Tibetan and Han individuals. Mean diastolic blood pressure was lower in Tibetan elderly than in Han elderly, whereas LDL cholesterol was higher in Tibetan elderly than in Han elderly. The ox-LDL levels differed significantly between Tibetan and Han after adjustment for LDL levels (P = .025; Figure). The prevalence of dyslipidemia and ox-LDL of 70 U/L or greater was significantly higher in Tibetan elderly than in Han elderly.
Comparison of basic characteristics between Tibetan and Han elderly highlanders
Data are given as the number (percentage) or as mean (95% confidence interval).
P values were calculated using Student’s t test or χ2 test.
Comparison of cardiovascular and metabolic items between Tibetan and Han elderly highlanders
SpO2, oxygen saturation of hemoglobin; IFG, impaired fasting glucose; IGT, impaired glucose tolerance; HOMA-R, homeostasis model assessment insulin resistance index; HDL, high-density lipoprotein; LDL, low-density lipoprotein; ox-LDL, oxidized low-density lipoprotein; CAVI, cardio ankle vascular index; ABI, ankle brachial pressure index.
Data are given as the number (percentage) or as mean (95% confidence interval).
P values were calculated using Student’s t test or χ2 test.
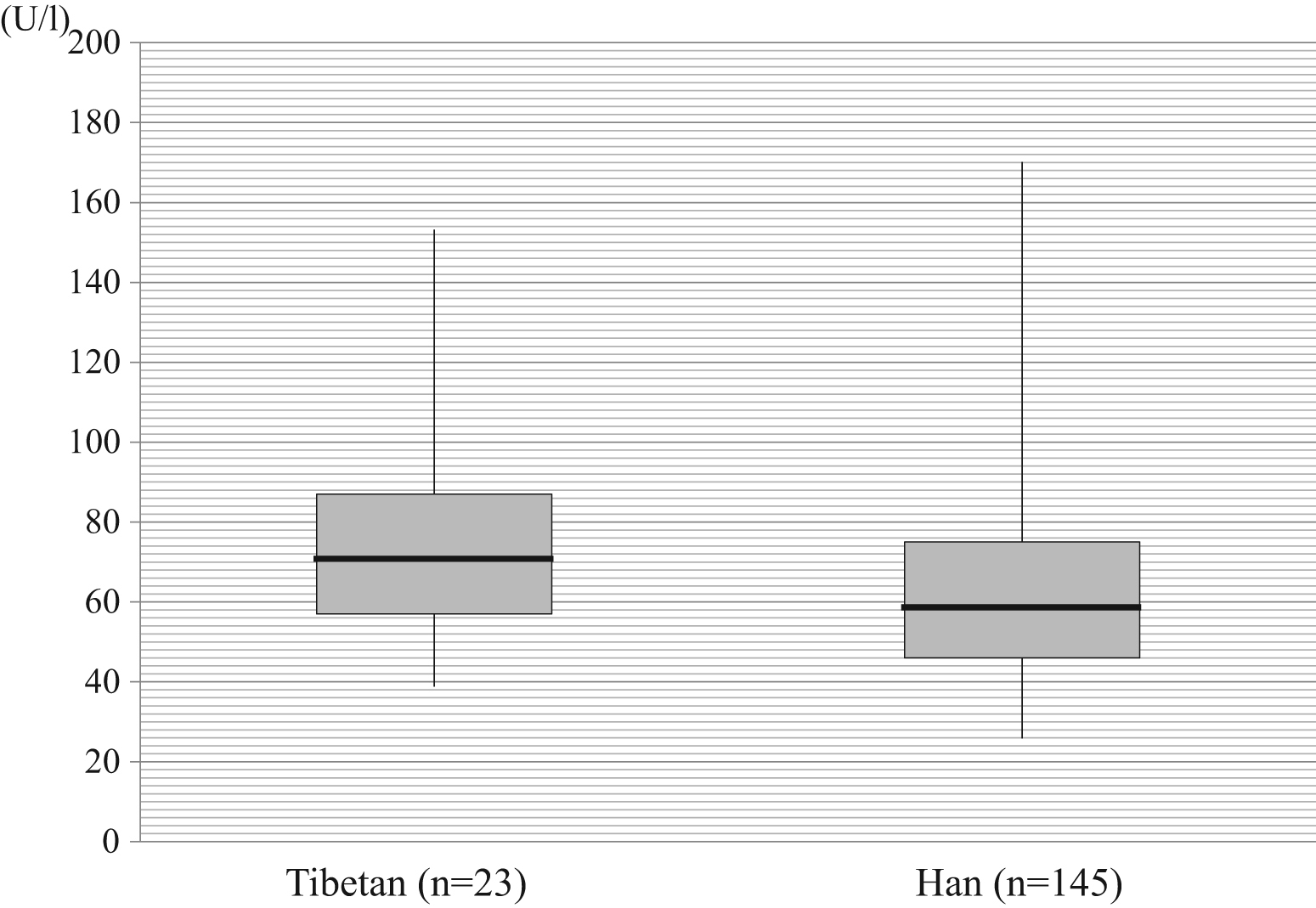
Level of oxidized low-density lipoprotein (LDL) in Tibetan and Han elderly highlanders. The thick horizontal lines represent medians, boxes represent interquartile ranges, and whiskers represent extreme values. The oxidized LDL levels differed significantly between Tibetan and Han after adjustment for LDL levels (P = .025).
OX-LDL Levels, Associated Factors, and Problems
The univariate analysis demonstrated that being Tibetan, LDL cholesterol levels, and frequency of vegetable intake and meat intake were associated with ox-LDL levels. The stepwise multiple regression analysis found that being Tibetan and LDL cholesterol levels were independent predictors of increasing ox-LDL levels (Table 3).
Factors associated with levels of oxidized low-density lipoprotein by regression analysis
SpO2, oxygen saturation of hemoglobin; HDL, high-density lipoprotein; LDL, low-density lipoprotein.
Multiple regression analysis was used. Multivariate model considered factors with P < .05 in the univariate analysis.
High ox-LDL levels (≥70 U/L) were significantly associated with prevalence of dyslipidemia, HOMA-R of 1.6 or greater, impaired fasting glucose (IFG), impaired glucose tolerance (IGT), diabetes, carotid plaque, and ABI of less than 1.0 in Han elderly highlanders by χ 2 test (Table 4). High ox-LDL levels (≥70 U/L) were significantly associated not only with dyslipidemia but also with HOMA-R of 1.6 or greater, IFG, IGT, or diabetes, after adjusting for age, sex, and ethnicity by logistic regression analysis (Table 5). The cutoff level for ox-LDL was defined as the cutoff at the 70th percentile.
Relations of high oxidized LDL (≥70 U/L) to cardiovascular and metabolic problems in Tibetan and Han elderly highlanders
ox-LDL, oxidized low-density lipoprotein; HOMA-R, homeostasis model assessment insulin resistance index; IFG, impaired fasting glucose; IGT, impaired glucose tolerance; CAVI, cardio ankle vascular index; ABI, ankle brachial pressure index.
Data are given as the number (percentage).
P values were calculated using χ2 test.
Relations of high oxidized low-density lipoprotein (≥70 U/L) to cardiovascular and metabolic problems
HOMA-R, homeostasis model assessment insulin resistance index; IFG, impaired fasting glucose; IGT, impaired glucose tolerance; CAVI, cardio ankle vascular index; ABI, ankle brachial pressure index.
Logistic regression analysis (to P < .05) was used. Covariates considered were age, sex, and ethnicity.
Discussion
The present study showed that Tibetan elderly highlanders had higher ox-LDL levels than Han elderly highlanders. High ox-LDL levels were significantly associated with high HOMA-R (≥1.6) and low ABI (<1.0) levels, and are associated with insulin resistance and arteriosclerosis. Although the precise pathophysiologic mechanisms have not been established, we speculate that differences in lifestyles and evolutionary genetic backgrounds between Tibetans and Hans affected ox-LDL levels. Factors known to affect ox-LDL include living in hypoxic environments, ultraviolet light, smoking habits, vegetable or fruit intake, and coldness. 6 In addition, one that we find particularly interesting is the effect of the natural selection of endothelial Per-Arnt-Sim domain protein 1 (EPAS1). 21
Several ways by which Tibetans have adapted to high altitudes have been reported as advantageous. For example, Tibetans tend to have lower hemoglobin (Hb).22,23 A mild increase in Hb is advantageous for oxygen transport to tissues, but too much Hb increases the risk of morbidities from pulmonary hypertension, stroke, and intrauterine growth restriction. 24 A study of individuals in the Andes found that ideal Hb concentrations are actually not so high. 25 Compared with Andeans, Tibetans have been reported to have higher ventilation volume at rest, lower pulmonary vasoconstriction under low oxygen, fewer low-birth-weight babies, and lower Hb.26,27 One other way that Tibetans adapt to high altitude hypoxic environments is increased nitric oxide (NO) production. 28 –30 Tibetans has been reported to have higher forearm blood flow and higher plasma nitrite levels compared with residents at sea level in the United States. 30 Higher blood flow and circulating NO products can offset high altitude hypoxia, and serve as a type of adaptation to hypoxia. 30 However, nitroxides are known to have dual activities as pro-oxidants and antioxidants. 31 Increased reactive oxygen species (ROS) reduce the amount of bioactive NO by chemical inactivation to form toxic peroxynitrite. In turn, peroxynitrite can uncouple endothelial NO synthase to become a dysfunctional superoxide-generating enzyme that contributes to vascular oxidative stress. 32
Our study found that Tibetan elderly highlanders have higher ox-LDL levels compared with those of Han elderly highlanders, but pathophysiological mechanisms in convincing detail remain to be identified. Several interesting reports have been published with regard to natural selection of EPAS1, egl nine homolog 1 (EGLN1), and peroxisome proliferator-activated receptor alpha (PPARA), identified as being involved in the adaptational process to hypoxia that has occurred in Tibetans over generations. 21 ,33,34 They are highly involved in gene regulation with regard to angiogenesis and metabolism of carbohydrates and fat. One study found that after exposure to hypoxic conditions, heterozygous EPAS1-deficient mice were protected against pulmonary hypertension and right ventricular hypertrophy. 35 Yet another study found that in such mice, oxidative stress was increased. 36 Indeed, as mentioned above, compared with Andeans, Tibetans have lower pulmonary hypertension under low oxygen. According to the results of the present study, Tibetan elderly individuals had higher levels of ox-LDL, an indicator of oxidative stress, relative to their Han counterparts. In Yushu County located at 3700 m above sea level, we detected increased weight, hypertension, and impaired glucose tolerance in relatively high prevalence among the Tibetan elderly. 37 We should be more concerned about the relationships among hypoxia, selected genes, oxidative stress, and metabolic problems. Although the data remain somewhat inconclusive, it is certainly possible that selected genes of Tibetans may partially contribute to the levels of ox-LDL. 21 ,30,35,36,38,39 It should be noted that advantages under certain conditions may become disadvantageous from different aspects.
Limitations
This cross-sectional study may suggest an association between ox-LDL levels and cardiovascular and metabolic indicators, but a cause-and-effect relationship cannot be concluded here. This study focused only on ox-LDL levels as an indicator of oxidative stress, but multilateral methods were needed to examine the consequences of ROS generation, which can be detected by formation of biomolecules altered by oxidation, including DNA, lipids, and proteins. To determine ethnicity, we used identification cards that included a description of ethnicity, but were unable to determine the precise duration for which an individual and his or her ancestors had resided at high altitude. The population-genetic mixture between Tibetans and Hans could not be determined by our data. The single-county location limits the generalizability. In addition, the study has a small and unequal sample size. The statistical power to detect the difference of ox-LDL between Tibetan and Han was approximately 0.83.
Conclusions
Our findings support the hypothesis that ox-LDL levels are higher among Tibetan elderly highlanders relative to those among Han elderly. As ox-LDL levels can affect insulin resistance and arteriosclerosis, further research is needed to determine how oxidative stress occurs among elderly individuals at high altitudes.
Footnotes
Acknowledgments
We thank all elderly highlanders who participated in the community-based geriatric examination in Haiyan County in Qinghai province. We also express our gratitude to Dr Masayuki Ishine, MD, Ms Airong Yang, Dr Jidong Gao, MD, Dr Zhanquan Li, PhD, Dr Yongshou Zhang, PhD, the young staff members of Affiliated Hospital of Qinghai University, and all staff members of Haiyan Hospital for their assistance.
This research was supported by a Grant-in-Aid from the Ministry of Education, Culture, Sports, Science and Technology for the Research Institute for Humanity and Nature (3-4 FR): Human Life, Aging, and Disease in High-Altitude Environments: Physio-medical, Ecological and Cultural Adaptation in “Highland Civilizations.”