
Abstract
Objective
The purpose of the study was to determine the effectiveness of Fluidotherapy rewarming through the distal extremities for mildly hypothermic, vigorously shivering subjects. Fluidotherapy is a dry heat modality in which cellulose particles are suspended by warm air circulation.
Methods
Seven subjects (2 female) were cooled on 3 occasions in 8˚C water for 60 minutes, or to a core temperature of 35°C. They were then dried and rewarmed in a seated position by 1) shivering only; 2) Fluidotherapy applied to the distal extremities (46 ± 1°C, mean ± SD); or 3) water immersion of the distal extremities (44 ± 1°C). The order of rewarming followed a balanced design. Esophageal temperature, skin temperature, heart rate, oxygen consumption, and heat flux were measured.
Results
The warm water produced the highest rewarming rate, 6.1°C·h−1, 95% CI: 5.3–6.9, compared with Fluidotherapy, 2.2°C·h−1, 95% CI: 1.4–3.0, and shivering only, 2.0°C·h−1, 95% CI: 1.2–2.8. The Fluidotherapy and warm water conditions increased skin temperature and inhibited shivering heat production, thus reducing metabolic heat production (166 ± 42 W and 181 ± 45 W, respectively), compared with shivering only (322 ± 142 W). Warm water provided a significantly higher net heat gain (398.0 ± 52 W) than shivering only (288.4 ± 115 W).
Conclusions
Fluidotherapy was not as effective as warm water for rewarming mildly hypothermic subjects. Although Fluidotherapy is more portable and technically simpler, it provides a lower rate of rewarming that is similar to shivering only. It does help decrease shivering heat production, lowering energy expenditure and cardiac work, and could be considered in a hospital setting, if convenient.
Introduction
Many wilderness and adventure activities present the risk of cold exposure and accidental hypothermia. In the United States, approximately 1500 hypothermic patients visit an emergency department (ED) each year. 1 Patients with mild to moderate hypothermia are generally warmed externally, namely, with warm water bottles “in the field” 2 or forced air warming “in the ED.” 3 These methods generally increase skin temperature and reduce shivering heat production, resulting in afterdrop and rewarming rates similar to those of shivering (control) protocols; shivering inhibition reduces metabolic energy use, cardiac work, and discomfort. 3
Whole body warm water immersion is contraindicated as it increases the risk of cardiovascular collapse. 4 However, immersing only the distal extremities in 45°C water safely decreased afterdrop and almost tripled the core rewarming rate to (9.9°C·h−1) compared with other external methods. 5 Limitations of this method include water spillage, specialized temperature control equipment, space requirements, and a fixed location.
Fluidotherapy, a common physiotherapy heating modality for distal extremities, is a potential alternate distal extremity rewarming method. This modality consists of a warming chamber with openings for distal arms and legs. 6 Cellulose particles, which form a fluidized bed, are circulated around the extremities by hot air. Fluidotherapy (48°C–49°C) provided three times greater heat transfer to copper bars, 6 and warmed muscle tissue by 20% to 50% more, 7 than warm water (39°C–41°C) or wax baths (52°C–55°C). This increased heat transfer may result from tolerance of higher temperatures of the fluidized bed compared with warm water, convective air movement, and high thermal conductance of cellulose particles.6,7 Higher temperature tolerance occurs because the cellulose particles overstimulate skin thermoreceptors and mechanoreceptors, consequently decreasing pain sensitivity. 6 Moreover, dry heat minimizes thermal irritation at high temperatures. 6 This method also provides more heat than traditional forced air warming 3 owing to a combination of higher air temperature (∼5°C) and thermal conductance of cellulose particles. Potential practical benefits of Fluidotherapy (compared with distal limb immersion) are that it is commercially available, technically simple, programmable, requires less space, is portable, and avoids water spillage.
The purpose of this study was to evaluate Fluidotherapy warming of all distal extremities in mildly hypothermic subjects. We hypothesized that Fluidotherapy (50°C) would provide more heat, reduce shivering and afterdrop, and increase core rewarming compared with extremity immersion in warm water (at 45°C) and shivering only.
Methods
Subjects
Physically active volunteers were studied after screening for any medical conditions and giving written informed consent. The Biomedical Research Ethics Board at the University of Manitoba approved the protocol.
Instrumentation
A single-channel electrocardiogram and heart rate were monitored continuously, and core temperature was measured by a thermocouple inserted into the esophagus (Tes) to the level of the heart.
8
Skin temperature (Tskin [°C]) and cutaneous heat flux (HF [W·m−2]) were measured at 12 sites with thermal flux transducers (Concept Engineering Old Saybrook, CT). Sites were forehead, anterior and posterior torso, upper arm, proximal and distal forearm, hand, anterior and posterior thigh, and proximal and distal lower leg and foot. Positive values indicate heat loss from the skin. Oxygen consumption (V
Rewarming Methods
Because subjects were seated in a head-down position during Fluidotherapy and water rewarming, they also assumed this position in the shivering condition to eliminate any possible effects of posture.
For the shivering only (control) rewarming method, after being seated, subjects leaned forward, resting their head on a head support, and were then covered with a sleeping bag. In this condition, the subject rewarmed spontaneously by endogenous shivering thermogenesis.
For the Fluidotherapy rewarming method, a chamber (model 115D, DJO Canada, Mississauga, Ontario) 86 cm long, 47 cm wide, and 84 cm high was used. New sleeves were created for the top portals of the chamber to allow insertion of all four distal extremities (ie, lower legs up to the knee and forearms up to the elbow). The unit was preheated to 45°C at 35% air speed. After limb insertion, the unit was then turned on at 45°C and 100% air speed. The subjects were then covered with a sleeping bag. Unit temperature was adjusted during the rewarming period based on the subject’s tolerance (maximum, 50°C) (Figure 1).

Distal extremity rewarming with Fluidotherapy (top panel) and warm water immersion (bottom panel). Distal extremities are exposed up to the elbows and knees. Note: the sleeping bag that is normally draped over the subject during Fluidotherapy was removed for easier visualization.
For the warm water method, the goal was to maintain water temperature at 45 ± 1°C; this would have the effect of decreasing the temperature advantage of Fluidotherapy, but we wanted to test both conditions at their maximum tolerable temperature and, therefore, rewarming effectiveness. After immersion, subjects were hoisted into the warm water tank and positioned with lower legs immersed to knee level. They then leaned forward resting their head on the front support, immersing their forearms up to the level of elbow (ie, same level as Fluidotherapy immersion), and were covered with a sleeping bag (Figure 1).
Protocol
Each subject was cooled on three different occasions separated by at least 48 hours, at the same time of day. Both female subjects were consistently studied in the follicular phase. After 10 minutes of baseline measurements, subjects were immersed up to the sternal notch in an approximately 21°C stirred water bath. Water temperature was then lowered to 8°C over 10 minutes by the addition of ice. Subjects remained in the water until either Tes reached 35°C or 60 minutes elapsed. Subjects were towel dried and then rewarmed by one of the three treatment methods. The order of rewarming methods was randomly chosen and followed a balanced design. Treatment continued for 60 minutes or until Tes rose to 37°C, followed by warm water immersion (40°C–42°C) until the Tes rose to 37°C (if necessary) or the subject wished to exit.
After their last trial, subjects were asked to compare the three rewarming methods based on warmth, comfort, and preference. They were also asked to provide any feedback related to discomfort associated with any of the methods.
Data Analysis
Rate of core cooling (°C·h−1) was calculated for the last 20 minutes of cold water immersion. Afterdrop (°C) was calculated as the difference between Tes on exit from the cold water and its nadir. Length of the afterdrop period (minutes) was calculated from the time of exit from the cold water until Tes returned to the original exit Tes. Rate of rewarming (°C·h−1) was calculated from the nadir to 35 minutes of rewarming. Distal extremity skin temperature (TskinDistExt [°C]) and distal extremity heat flux (HFDistExt [W]) were calculated from area-weighted average of temperatures and a sum of the absolute heat flux values (6 sites). Total skin temperature (TskTotal) and total heat flux (HFTotal) were calculated using all 12 sites.
Net heat balance was calculated by subtracting the respiratory heat loss (RHL [W] = 0.09 * M) and total cutaneous heat flux from the metabolic heat production (M [W] = V
Data for the three conditions were compared using repeated measures analysis of variance for all the variables. A post hoc analysis for significant differences between treatments was accomplished using Tukey’s post hoc test. Results are reported as mean ± SD for absolute amounts, or mean (95% confidence interval) for rates; P < .05 identified statistically significant differences.
Results
Seven subjects (2 female) were studied, with a mean ±SD age of 29.3 ± 3 years, height 174.6 ± 12 cm, weight 80.9 ± 16 kg, body surface area 2.0 ± 0.2 m2, and fat percentage 23.6% ± 7%.
Core Temperature
Exit Tco was 35.9 ± 1°C. There were no significant between-condition differences in either core cooling rate or afterdrop amount or duration (Figure 2). The rewarming rate in the warm water (6.1°C·h−1, 95% CI: 5.3–6.9) was significantly higher than in the other two conditions (2.0°C·h−1, 95% CI: 1.2–2.8 for shivering only, and 2.2°C·h−1, 95% CI: 1.4–3.0 for Fluidotherapy; n = 7; P < .01).
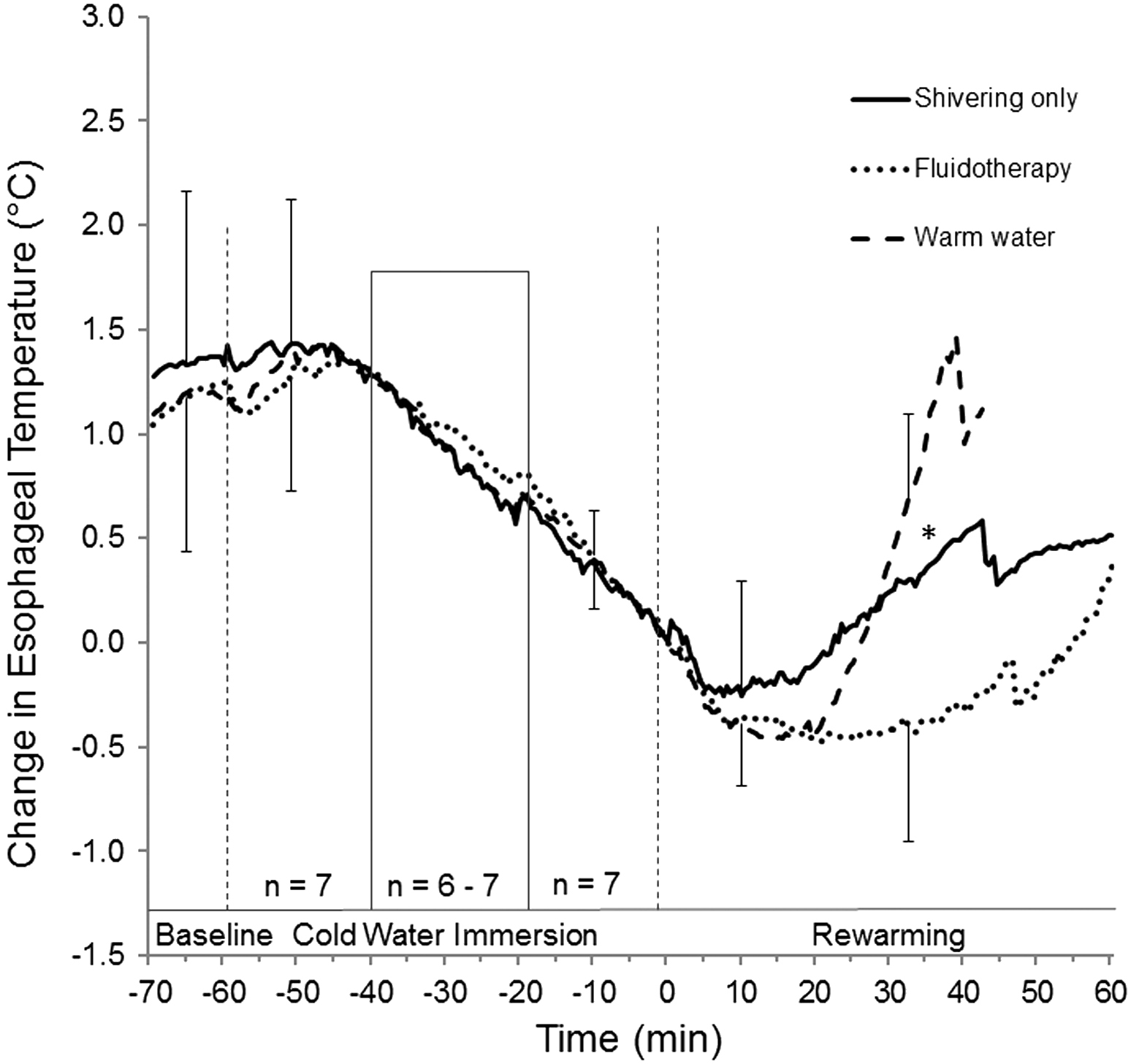
Mean change in esophageal temperature (°C) during baseline, as long as 60 minutes of immersion in 8˚C water, and as long as 60 minutes of rewarming in the shivering only condition (solid line), Fluidotherapy condition (dotted line), and warm water condition (dashed like). Time 0 minutes and temperature 0˚C indicate exit from cold water (bars, SD). Six of the 7 subjects were immersed for the entire 60-minute cold water period in all conditions. The other subject reached the target esophageal temperature of 35°C within 38 to 46 minutes in all three immersions. To show what the whole group did at beginning and end of immersion, data for trials less than 60 minutes are presented for the first 20 minutes, with the remainder adjusted so that the exit time is lined up for everyone at time 0. As a result, n = 7 for data from −60 to −40 minutes and from −18 to 0 minutes. During the period between −40 and −18 minutes, n = 6 to 7. *Separates conditions that are significantly different from each other (P < .01). Abrupt decreases near the end of rewarming periods are an artifact caused by termination of subjects who completed warming earlier than the others.
Average Skin Temperature And Heat Flux
During rewarming, average total skin temperature was lower for the shivering only condition (24.6 ± 1°C) than for Fluidotherapy (30.6 ± 1°C) and warm water (29.5 ± 2°C; P < .01). However, there were no differences between the Fluidotherapy and warm water conditions. This corresponded to a mean total heat flux for the shivering only condition (loss of ∼5 W) that was significantly different than Fluidotherapy and warm water (gain of more than 200 W), with no difference between the latter two conditions (P < .01) (Table 1). Distal extremity skin temperatures and heat transfer were significantly different (P < .01) between all conditions, with highest values for warm water immersion and lowest values for shivering only (Table 1).
Results of afterdrop, rewarming rate as well as heat production and transfer values by condition during rewarming
Values are mean ± SD for amounts; mean (95% CI) for rate.
T, temperature; HF, heat flux (positive values indicate loss); skinDistExt, skin distal extremities; DistExt, distal extremities; AntTor, anterior torso; HB, heat balance (positive values indicate gain).
Different from shivering, P ≤ .05.
Different from shivering, P ≤ .01.
Different from Fluidotherapy, P ≤ .05.
Different from Fluidotherapy, P ≤ .01.
Metabolic Heat Production
During rewarming, the average metabolic heat production was significantly higher in the shivering only condition compared with the Fluidotherapy and warm water conditions (P < .05) (Table 1; Figure 3, top).
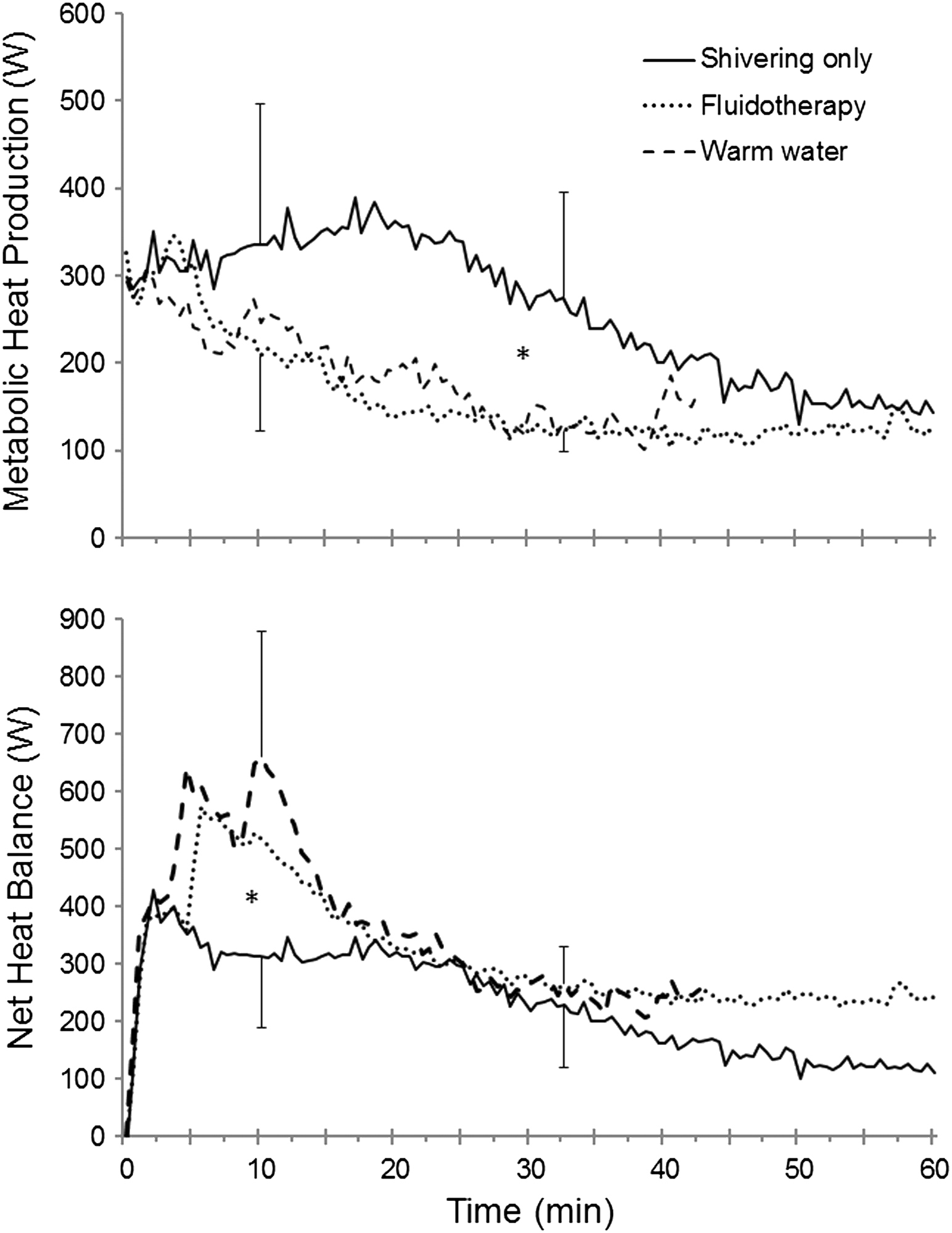
(Top panel) Metabolic heat production (W) and (bottom panel) net heat balance (W) during 60 minutes of rewarming (bars, SD). *Separates conditions that are significantly different from each other (P < .05). Solid lines, shivering only; dotted lines, Fluidotherapy; dashed lines, warm water.
Net Heat Balance
During rewarming, the mean net heat gain during warm water immersion was significantly higher compared with shivering only (P < .05) (Table 1; Figure 3, bottom) but not Fluidotherapy.
Subjective Evaluation
Two subjects said that the warm water was too hot to get into initially, and another reported a feeling of “pins and needles”; the latter subject also felt Fluidotherapy was too warm. However, apart from the initial discomfort, warm water was the treatment of choice by 6 of the 7 subjects, whereas 1 preferred Fluidotherapy. Two subjects reported either back pain or that they did not like the forward-leaning position for Fluidotherapy; another subject made similar reports for all conditions.
Discussion
There was no significant difference in Tco afterdrop among the three conditions. These values (0.6–0.7°C) are consistent with other rewarming conditions in which the shivering mechanism was intact. 3 ,5,8 Fluidotherapy provided a rewarming rate similar to that of shivering only, and was consistent with other external rewarming modalities.3,8
Consistent with previous studies, heat production and respiratory heat loss were increased in the shivering only condition.5,9 Shivering only provided a rewarming rate of 2.0°C·h−1, and in previous studies conducted, 3 ,5,8 shivering by itself provided rewarming rates ranging from 2.4°C·h−1 to 3.5°C·h−1. However, it is important to note that the mean exit Tco in the present study (35.9°C) was higher than that in previous studies. 3 ,5,8,9 As Tco decreases, shivering heat production and rewarming rates increase.
When exit Tco was lower, the rewarming curve was steeper initially, with high rewarming rates (3.0–3.5°C·h−1), with an inflection to a lower rewarming rate (1.5–2.0°C·h−1) at Tco approximately 36°C. In the present study, there was no inflection during rewarming for shivering, similar to later rewarming (>Tco of 36°C) in previous studies. In the present study, the highest rewarming rate and heat transfer with water immersion was consistent with previous studies. 5
Fluidotherapy actually donated less heat than warm water for several reasons. First, the temperature difference between Fluidotherapy and warm water was only approximately 2°C because none of the subjects tolerated Fluidotherapy at 50°C (maximum was 46.1°C). Second, the thermal conductivity of the fluidized cellulose bed is higher than air alone, but lower than water. Thus, the small temperature increase with Fluidotherapy (46°C vs 44°C) was not enough to transfer more heat than the water. Third, although heat transfer was consistent over all immersed skin in warm water, it decreased proximally in immersed skin in Fluidotherapy (as indicated by skin redness). Finally, our warm water rewarming rate was lower than previously reported. 5 This finding is consistent with the higher end cooling Tco in this study (35.9°C vs 34.3°C).
We do not consider that our sample size (n = 7) was a limitation of this study; this sample size provides enough power to reveal any clinically significant differences. Five subjects had high body fat, and exit Tco did not reach the clinical threshold for hypothermia (35°C). That did not limit our conclusions, as we have previously shown that in high-fat groups (with similar exit Tco), any intercondition differences are actually accentuated. 10
Conclusion
Although Fluidotherapy did not rewarm subjects as quickly as warm water, it had the advantage over passive rewarming (shivering) of decreasing shivering metabolism, and presumably cardiovascular work. Because Fluidotherapy is more portable and technically simpler than warm water, it could be used for mild hypothermia. Neither extremity warming technique is advised for moderate to severe hypothermia owing to the patient’s decreased physical capacity and potential loss of consciousness.
Footnotes
Acknowledgments
We would like to thank the Natural Sciences and Engineering Research Council of Canada for financially supporting this project, and the Faculty of Kinesiology and Recreation Management, University of Manitoba, for their financial support by FKRM Stipend and Graduate Research Assistantship. We would also like to thank our subjects for participating in the study. Finally, a special thanks to Jimmy Gazetis from DJO Global for lending the Fluidotherapy equipment to conduct the study.