
Abstract
We describe an illustrative case of pediatric snake envenomation presenting with a tightly wound tourniquet. A 10-year-old boy presented after a snake bite to the right calf. A tourniquet was in place just below the right knee. The species of snake was unknown. The patient was hemodynamically stable, but the entirety of the right leg distal to the tourniquet was discolored. Over concern for a potential venom bolus effect upon tourniquet removal, the decision was made to start a crotaline Fab antivenom infusion and gradually loosen the tourniquet. The patient tolerated the infusion and removal of the tourniquet without signs of anaphylaxis or decompensation. Dynamic improvements were observed in the right leg and wound site that appeared to be the result of vascular congestion. Tourniquets are generally not recommended for snakebites; however, if a tourniquet is already placed, we avoid removal until prepared to manage acute toxicity or immediate hypersensitivity.
Introduction
When a person is bitten by a snake, interventions by others at the time of the bite can influence the pathophysiology of the snakebite, the medical management when the patient arrives at the hospital, and the patient’s long-term prognosis. A common, often misguided, intervention utilized by the lay public after a snake bite is the application of a tourniquet, a material applied circumferentially to the involved extremity proximal to the site of injury that, depending on how tightly it is applied, impedes arterial, venous, and lymphatic drainage of the distal region of the extremity. 1
This report is of an illustrative case managed in our children’s emergency department and hospital at a teaching facility. The antivenom used in this case was Crotalidae Polyvalent Immune Fab (Ovine [CroFab, BTG International, West Conshohocken, PA, USA]) and will be referred to here as antivenom.
Case Presentation
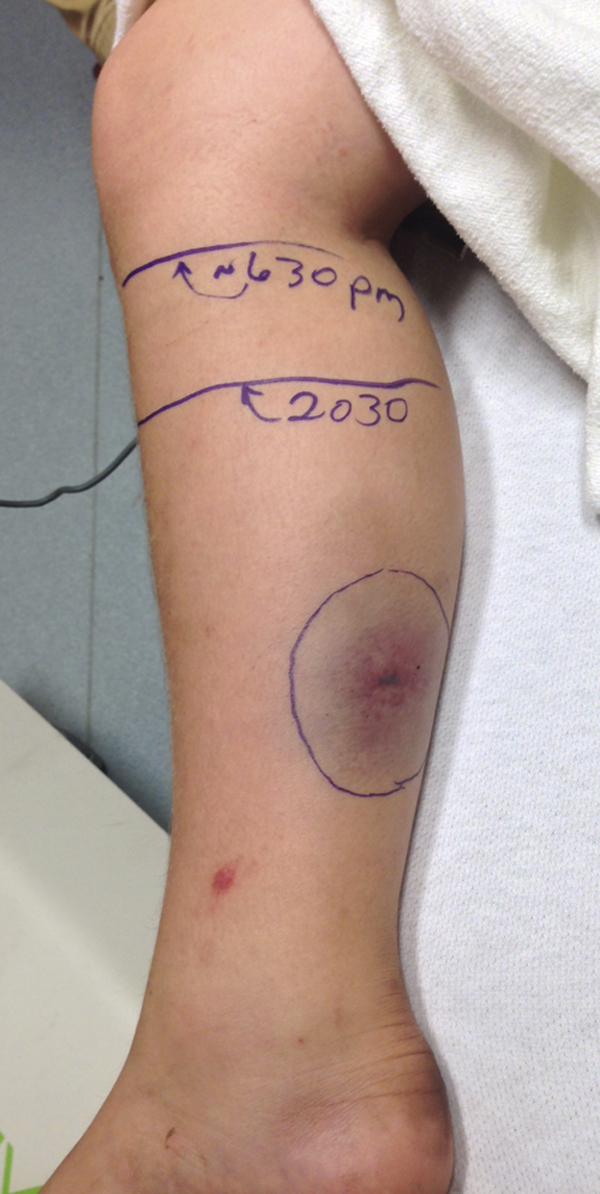
A 10-year-old, otherwise healthy boy was brought to the emergency department by private vehicle after a snakebite, which had occurred approximately 25 minutes earlier. No adult was present at the time of the snakebite, but the family reported sightings of copperhead snakes where they live in North Carolina. The snakebite was in the right calf, with two fang puncture sites located 18 mm apart. There was localized bruising and a small bulla at the bite site. A tight tourniquet was placed in the field by the patient’s brother. The tourniquet was a leather belt wrapped around the patient’s right leg to the knee joint. Dusky purple discoloration was observed distal to the tourniquet (Figure 1). Otherwise, the patient’s physical examination was unremarkable. He was alert and oriented, and in mild distress. Initial vital signs were blood pressure 126/89 mm Hg, heart rate 119 beats/min, respiratory rate 25 breaths/min, temperature 36.9°C, and 100% oxygen saturation on room air by pulse oximeter. Results of the initial set of laboratory tests as well as the subsequent laboratory analyses are available in the Table.

Before antivenom infusion.
Laboratory measurements
INR, international normalized ratio.
Six vials of antivenom were prepared as expeditiously as possible and in accordance with the manufacturer’s new prescribing information, and the infusion of antivenom was started approximately 1 hour after presentation at a rate of 50 mL per hour. That was tolerated well, with no signs of adverse drug or immune reaction. Ten minutes later, the infusion rate was increased to 250 mL per hour as the tourniquet was loosened over the next 10 minutes. No evidence of acute systemic toxicity or hypersensitivity was observed. The wound evolved in a dynamic manner, as demonstrated by serial images (Figures 2–4) with the most proximal region of tenderness to palpation marked on the patient’s leg. The region of swelling and tenderness to palpation receded over the course of the antivenom infusion.

Five minutes after start of antivenom infusion. Process of loosening tourniquet has begun, with subsequent decrease in signs of vascular congestion.

Fifteen minutes after start of antivenom infusion. Vascular congestion continues to improve, with tourniquet now fully removed.
Sixty minutes after start of antivenom infusion. Minimal signs of vascular congestion.
Before discharge the next morning, the small bulla had increased in size minimally. Mild edema was present in dependent regions. The patient was ambulatory with crutches. He was discharged with snakebite wound management and follow-up instructions. No further antivenom was administered. Seven weeks after the bite, the patient had recovered almost completely, and he was ambulating without crutches. He did report some residual, episodic pain in his right leg; that had resolved at the 3-month follow-up.
Discussion
Numerous different types of tourniquets have been described in the literature, both historically and in recent years, as techniques used by first-responders handling snakebites in the field. Arterial tourniquets result in a pressure gradient that is high enough to impede arterial blood flow distal to the device. 1 Venous tourniquets produce only enough pressure to prevent venous and lymphatic flow proximal to the tourniquet. 1 A more complex type of tourniquet is a pressure-immobilization bandage. The pressure-immobilization bandage includes an elastic bandage, which is applied to the entirety of the extremity, and a stabilizing splint. Currently, the use of a tourniquet after a snakebite is a controversial intervention, with some studies suggesting tourniquets will result in increased risk to the patient and other studies suggesting possible benefits to early application of certain types of tourniquets (eg, pressure immobilization) after certain types of snakebites. 1 –5 Although low-pressure lymphatic constriction wraps are generally condoned for bites by Australian and American Elapidae (such as coral snakes), arterial tourniquets are almost universally condemned.
Six species of venomous snakes are indigenous to North Carolina: the coral snake (Micrurus fulvius), the eastern diamondback rattlesnake (Crotalus adamanteus), the timber rattlesnake (Crotalus horridus), the cottonmouth (Agkistrodon piscivorus), the copperhead (Agkistrodon contortrix), and the pigmy rattlesnake (Sistrurus miliarius). 6 Of these 6 venomous species, copperheads are most frequently encountered. Other species, such as timber rattlesnakes, are seen with regularity in this region as well, and cause some of the most severe envenomations encountered in the United States. 6
Over concern for a possible venom bolus after release of the tourniquet, the decision was made in our case to initiate antivenom infusion before removing the tourniquet. The bolus effect is the acute progression of envenomation complications, such as neurotoxic effects of snake venom, upon removal of a tourniquet.1,2 This effect is thought to be due to a sudden increase in venom concentration upon tourniquet removal, given the dose-dependent relationship between snakebite venom and its subsequent toxicity. 2 The rationale behind starting the antivenom infusion before tourniquet removal was that venom effect could be minimized by both gradually loosening the tourniquet and ensuring that the antivenom was present. As described, the patient tolerated the process of antivenom infusion and tourniquet removal without any worsening of signs or symptoms. Indeed, the patient reported decreased pain after removal of the tourniquet. That suggests the pain was due more to ischemia than to envenomation.
A major complication that can arise from a snake envenomation is tissue necrosis secondary to vascular congestion. Viper venoms contain digestive enzymes, which break down the subcutaneous tissue, including blood vessels, leading to local hemorrhage. For example, metalloproteinases break down the proteins that surround and protect blood vessels. 7 Vascular congestion can result, and can lead to a disruption of orderly blood flow into and out of the region of leaking blood vessels. The region can become ischemic, and if orderly blood flow is not restored, tissue necrosis can occur. The dynamic nature of the appearance of our patient’s right leg and wound site from the time of presentation in the emergency department until 60 minutes after the start of the infusion (see Figures 1–4) appears to be a result of marked vascular congestion distal to the tourniquet, which progressively improved after tourniquet removal. It is possible the combination of tourniquet-generated vascular congestion and venom-mediated necrosis could compound wound complications and delay healing.
Although this discussion is largely focused on the bolus effect associated with tourniquets, it is appropriate to note that not all tourniquets are contraindicated, and in some situations, tourniquets can be helpful in treating bites from specific species of snakes. For example, there is evidence that a pressure-immobilization bandage applied immediately after a bite from the eastern coral snake (Micrurus fulvius fulvius) actually delays the onset of systemic toxicity in pigs. 3
Ultimately, the nature of the patient’s puncture wounds and the lack of abnormal coagulation parameters and neurotoxic symptoms suggested that this snakebite was most likely from a copperhead snake. Although bites by copperhead snakes may not in and of themselves necessitate administration of antivenom, the use of a tourniquet and the unknown snake species warranted its use in this case.
Conclusion
Healthcare providers need to be aware of the dangers associated with tourniquet application after a venomous snakebite, and applying a tourniquet after such a bite is not recommended. However, if a tourniquet has been applied, healthcare providers should be aware of the possibility of a bolus effect and should keep the tourniquet in place until they are prepared to handle the possible acute toxicity or anaphylaxis associated with its removal. Moreover, a tourniquet should be loosened gradually in an attempt to mitigate any bolus effect. Healthcare providers should strongly consider using antivenom in this situation, depending on the type of tourniquet applied and the species of snake responsible for the bite. If the decision is made to use antivenom, the infusion should be started before removing the tourniquet, and the tourniquet should be removed only after the patient is tolerating the full infusion rate without signs of anaphylaxis.