
Abstract
We report 2 cases of catastrophic ischemic stroke after Crotalidae polyvalent immune Fab (ovine)-treated rattlesnake envenomation, 1 fatal and the other resulting in significant permanent disability. It is possible these serious adverse events may have been related to venom factor(s), an interaction between venom and antivenom, occult patient blood dyscrasia, or to random unrelated events. We present the rationale for each possibility, and submit the experiences to elicit alternate postulation and communication of similar presentations.
Introduction
Ischemic stroke is extraordinarily rare after snakebite envenomation, particularly when compared with other serious yet uncommon complications, such as hemorrhagic stroke or other serious bleeding. Neurological complications after snakebite typically include paresthesias, paralysis, damage to local nerve structures, and myokymia. Many serious rattlesnake envenomings cause thrombocytopenia and hypofibrinogenemia that raise common concerns about easy bleeding, bruising, or even spontaneous bleeding. Ischemic stroke, although described for other snake envenomations (Bothrops lanceolatus, Daboia [Vipera] russelii, Echis carinatus [coloratus], Hypnale hypnale, and so forth), 1 –6 has only been reported once after a rattlesnake envenomation in the United States and one other time after a South American rattlesnake bite. We describe 2 additional cases of catastrophic ischemic stroke after rattlesnake envenomation.
Case Presentations
CASE 1
A 50-year-old man was bitten on his left anterolateral calf on May 16, 2003, at approximately 12:15
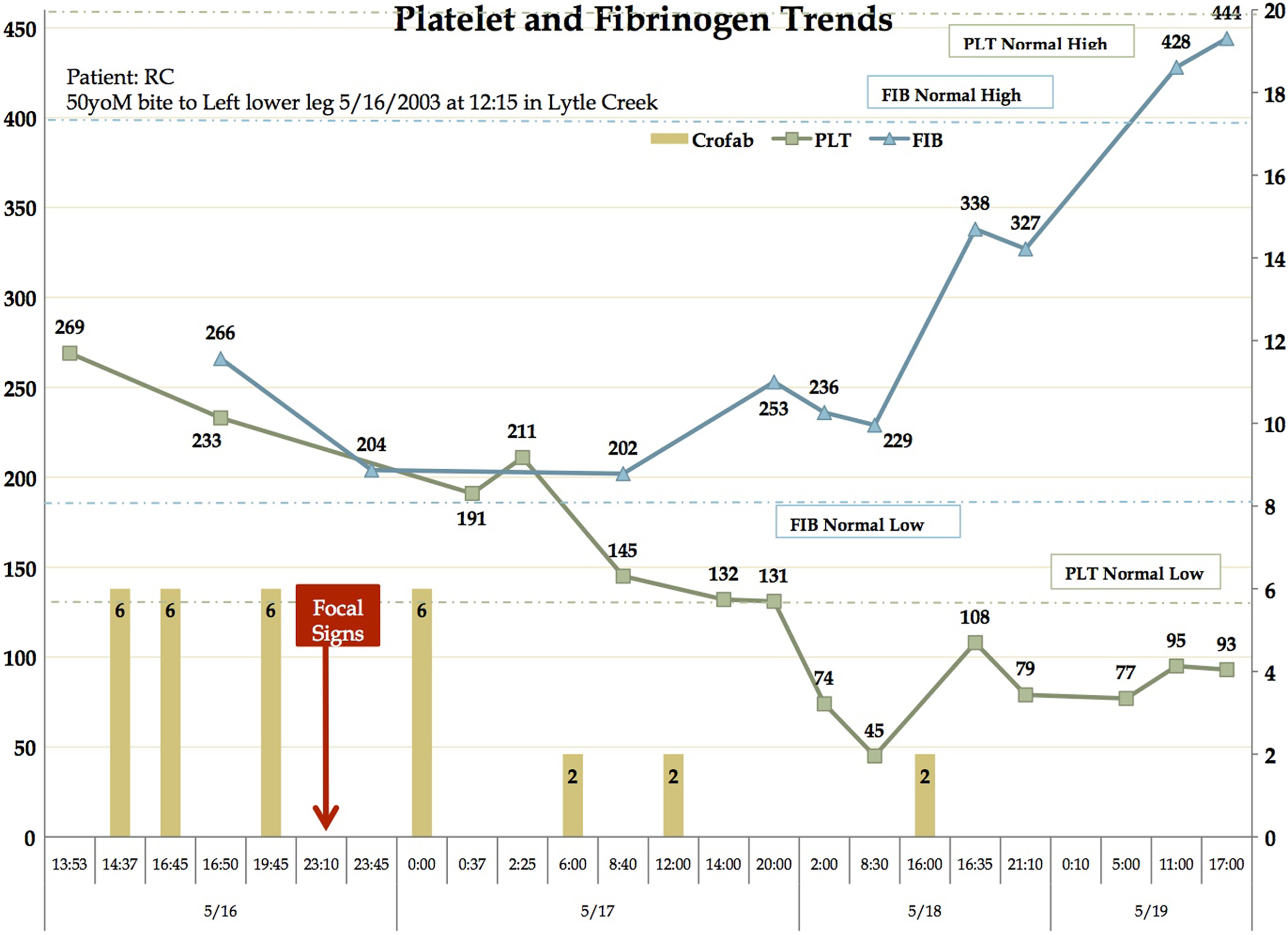
Platelet counts, fibrinogen levels, and fab antivenom dosing over time. Stroke symptoms onset approximately 11 hours after the snakebite.
At 11:10

Neurological exam revealed right facial paresis sparing the forehead. Patient consented to picture for educational use.
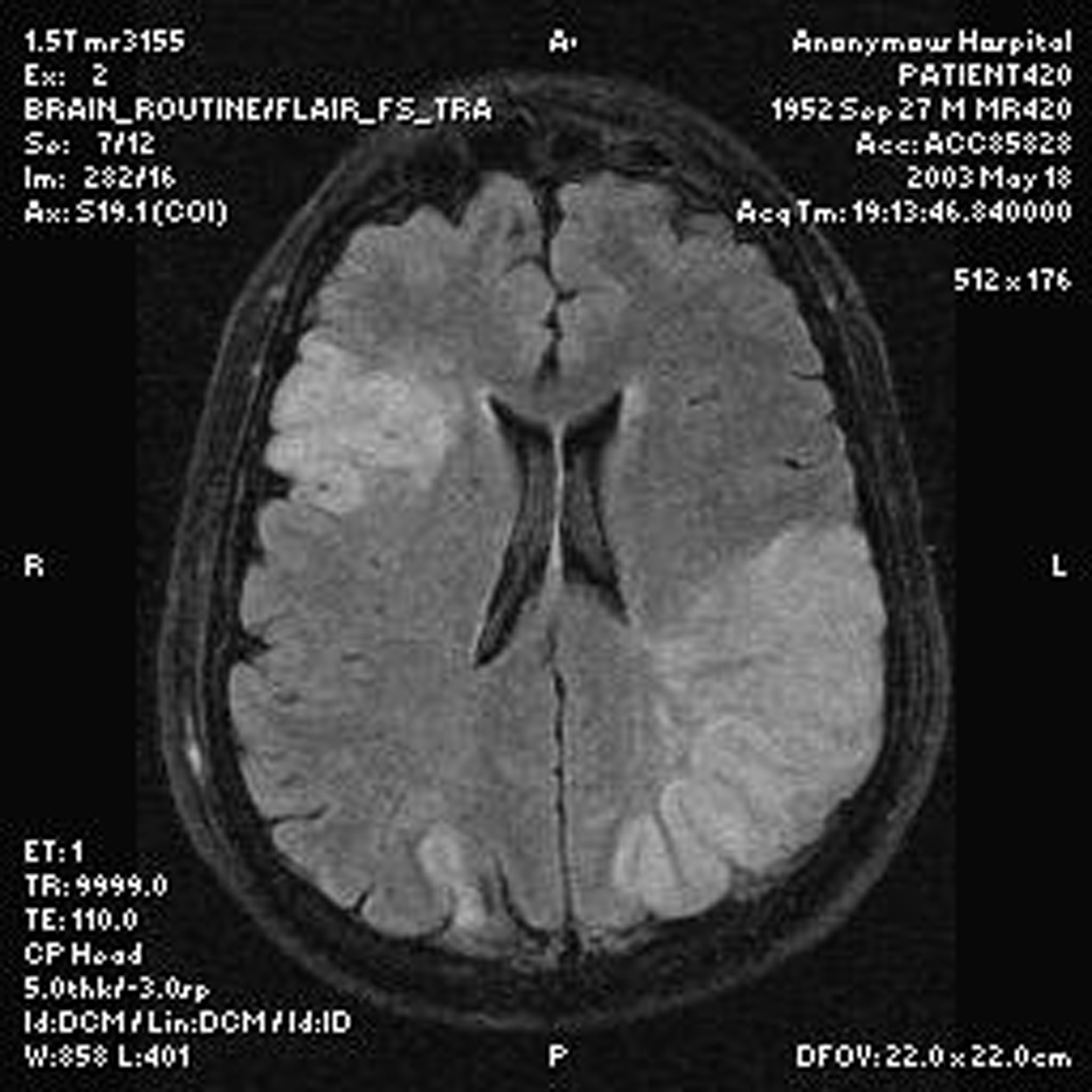
Brain MRI showed infarctions.
The patient began to have hematuria and coffee grounds emesis. Laboratory testing revealed coagulopathy at this point. An echocardiogram was obtained without evidence of thrombus or significant cardiac abnormality. The patient was also tested for protein C and S activity, lupus anticoagulant, factor V Leiden, antithrombin III activity, homocysteine levels, factor II assay, and factor V assay, which were found to be normal. Subsequent head computed tomography scan showed extensive bilateral ischemic infarcts and cerebral edema, with concern for herniation. The patient continued to deteriorate until the decision between family and the medical team was made to terminate life-sustaining measures as the patient was found to have a poor prognosis and was unlikely to regain meaningful neurological function. The patient ultimately died on May 19, 2003, at 10:10
CASE 2
A 17-year-old male was bitten on his right ring finger after attempting to pick up a snake on June 28, 2008, at approximately 6:40
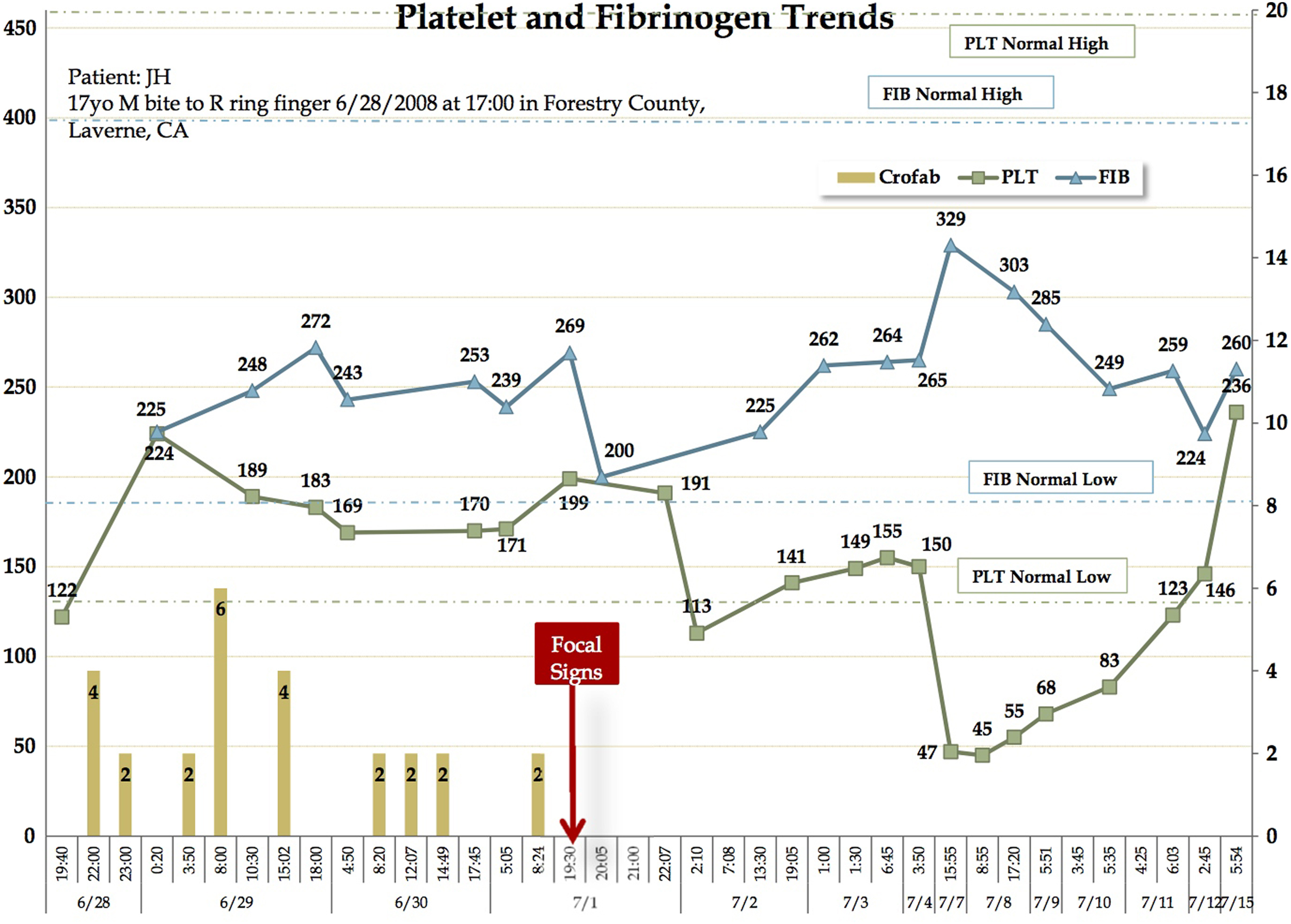
Platelet counts, fibrinogen levels, and fab antivenom dosing over time. Stroke symptoms onset approximately 3 days after the snakebite.
On July 1, 2008, at approximately 8:00

On neurological exam, patient was found to have left facial paresis without forehead involvement.
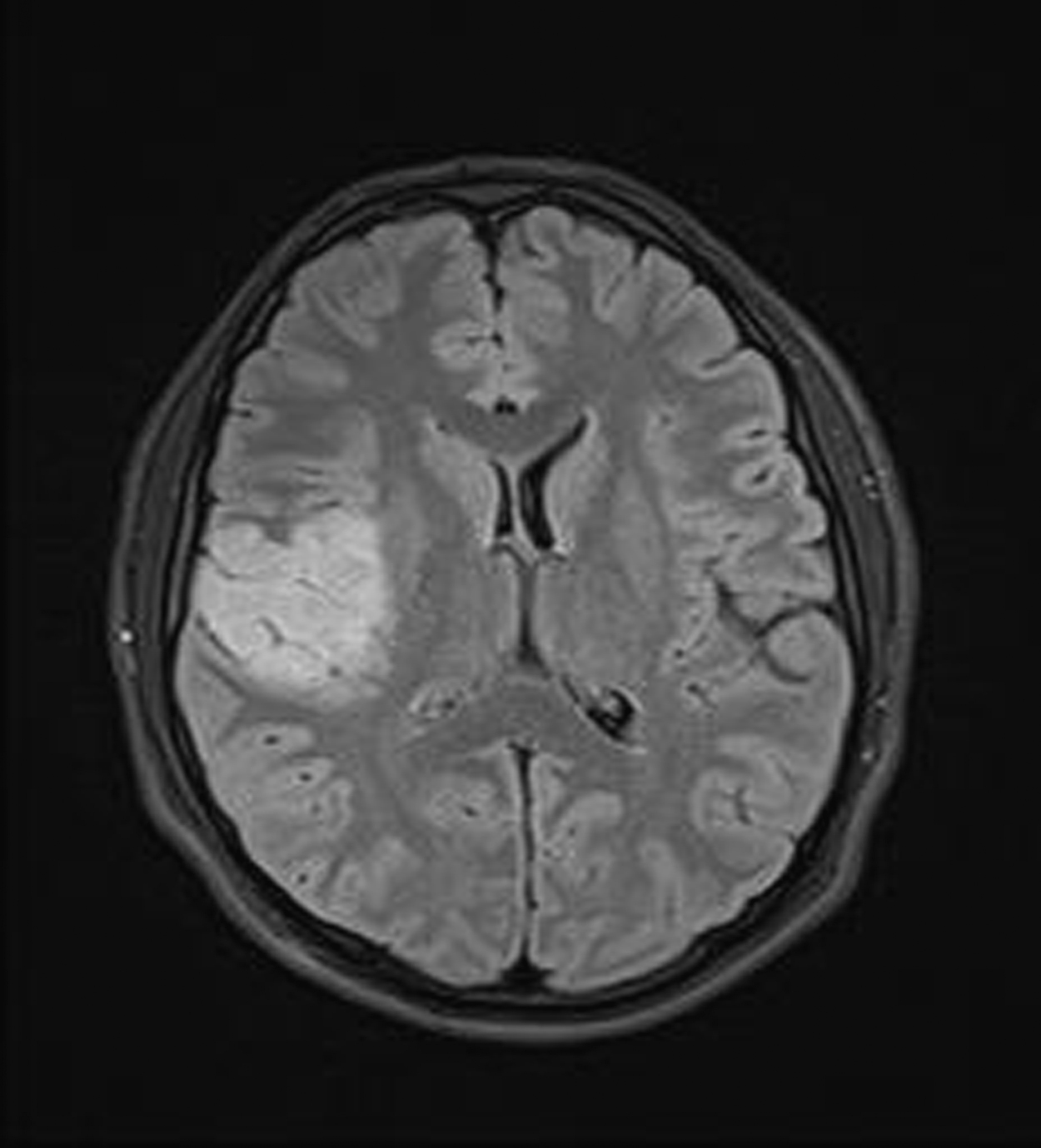
Brain MRI showed infarction.
Discussion
These 2 cases have clinical and radiographic evidence that an acute ischemic stroke event occurred. Both events are also temporally associated with acute rattlesnake envenoming, with at least 1 case being definitively identified as C oreganus helleri. Neither patient was at high risk for stroke, but especially not the case involving the 17-year-old patient. Specific etiology of acute ischemic strokes after envenomation are not fully understood, although various mechanisms have been proposed, 7 –11 and will be further discussed below as they relate to these cases.
It is possible that the venom from the snakes implicated in these 2 cases contained a procoagulant that is unique to this species or region, or even to these particular snakes, and is not found in other snakes. Snake venom is highly specialized, generally in a manner that optimizes the snake’s ability to capture the predominant prey in the area where the snake lives. This variability can be species distinct but there is considerable intraspecies variability. Individual snake venom composition may vary depending on the age of the snake, time of the year, and other things. Venoms of C oreganus helleri varied qualitatively and quantitatively in their activity (eg, hemorrhagic activity, amidolytic activity, coagulant activity, fibrinolytic activity, and so forth), even within a small geographical area in southern California. 12 In a recent study, procoagulant activity was discovered for the first time in a single C oreganus helleri specimen’s venom from Wrightwood, California. 13 In the same study, procoagulant activity was not found in other C oreganus helleri venoms, and in contrast, other venoms, such as Crotalus atrox, had just the opposite, namely, anticoagulant activity. The C oreganus helleri venom is among the most varied venom ever described.14,15 That may explain why thrombotic complications are so exceedingly rarely seen clinically. We believe that is the most likely explanation for these patients’ clinical presentations.
Alternatively, some venom components are not well neutralized by antivenom, likely because they are not immunogenic enough (too small, too rare) for antibodies to be formed. For example, myokymia is unfazed by megadoses of FabAV, probably because it is the result of small basic peptides similar to crotamine that do not generate much if any immune response. The procoagulant described above may be so rare that there are insufficient quantities or none in the venoms used to derive FabAV. FabAV has differential cross protectivity for C oreganus helleri venom.15,16 That may, in part, be due to toxins such as Mohave toxin that are well-neutralized versus others that are not like components that cause myokymia. It is also possible that, under certain circumstances, antivenom better neutralizes anticoagulant properties versus procoagulant properties so that there can be a phase when hypercoagulation dominates over hypocoagulability. We believe it is a highly significant observation that the patients had both been treated with antivenom before the onset of stroke symptoms, and that this is the first time a temporal relationship of this nature has been clearly documented. We suggest that these be considered a “serious adverse event” and that the possibility of a relationship to this antivenom be considered. Specific data regarding Southern Pacific rattlesnake (C oreganus helleri) and ischemic stroke events are limited, and further investigation is needed to evaluate toxic vasculitis or endothelial injury as a cause of ischemic stroke after envenomation. Further investigation may aid in future treatment as no current guidelines or recommendations exist that illustrate appropriate actions to avoid, or treat, thrombotic events associated with rattlesnake envenomations.
Patient-specific risk factors for hypercoagulability were also considered; however, both patients had normal complete blood count, prothrombin time, partial thromboplastin time, international normalized ratio, and fibrinogen, and tested negative for hypercoagulable risk factors (eg, factor V Leiden, protein C and S deficiency, lupus anticoagulant, antithrombin III activity, and homocysteine levels). True disseminated intravascular coagulation is generally not associated with rattlesnake envenomation but was a possibility we considered in these cases.
Hypotension due to hypovolemia, third spacing of intravascular fluid secondary to venom effect and systemic response, vasodilator effects of venom and systemic response, vomiting, sweating, and ultimately, hypotensive shock have been proposed as a possible etiology of acute ischemic stroke after envenomation.8,11 In the cases presented, neither patient sustained significant or prolonged episodes of hypotension before the onset of their neurological symptoms. The ischemic strokes that occurred in these cases are also similar to those described in other case reports in the literature in that the infarcts did not appear in traditional watershed areas that are more indicative of hypotensive shock. Therefore, hypotension seems less likely as the etiology of acute ischemic stroke in the context of these cases.
Endothelial injury or toxic vasculitis from venom components resulting in increased susceptibility for thrombus formation has also been proposed as potential mechanisms. 8 –11,17 In the case of Daboia russelli envenomations associated with ischemic stroke events, Gawarammana et al 18 report the vasculitis was a less likely mechanism, as many patients presented with neurological symptoms within minutes to hours of envenomation. In the cases presented in this article there was a delay in onset of neurological symptoms, providing increased time for potential vascular damage. However, each patient received timely administration of appropriate FabAV therapy before the onset of their ischemic stroke symptoms. Therefore, this mechanism seems less likely as well.
Finally, it is possible that these sequelae are multifactorial or that they are the result of a yet-to-be-described mechanism. It is for this reason that we have published these case reports—so that other experts may offer hypotheses.
Conclusions
Ischemic stroke after snakebite is a rare but devastating complication after rattlesnake envenomation. The exact cause of these events are unknown but may be related to venom components and their effect on vascular endothelial cells causing local damage and inflammation combined with venom-induced effects on coagulation, resulting in an increased susceptibility to thrombus formation. Currently, no guidelines exist regarding specific treatment of rattlesnake envenomings with complications of ischemic stroke. Further investigation is needed to better understand the exact pathophysiological mechanism and appropriate treatment as current treatments (ie, thrombolytic medications) may be contraindicated secondary to the risks of intracranial bleeding associated with these medications, particularly in the context of concomitant rattlesnake envenoming.