
Abstract
Background
Minimal data exist regarding the activity, membership, training, and medical oversight of search and rescue (SAR) teams.
Objective
Our objective was to describe these characteristics in the Intermountain West SAR organizations.
Methods
A contact list was generated and electronic surveys were sent to SAR officials in each Intermountain West county. Results were descriptively analyzed.
Results
Of the contacted jurisdictions, 56% (156) responded to the survey. The annual average call volume was 29 missions (range, 5 to 152). Multiple levels of medical training were represented on SAR teams, ranging from first aid/cardiopulmonary resuscitation providers to the physician level, and 79% of teams provided some medical training to their membership. Of the SAR medical professionals, 23% had formal wilderness medical training. Local emergency medical services provided 60% of the medical care on SAR missions rather than SAR personnel. Formal physician medical oversight was present in 41% of the SAR teams. These physicians participated in a range of SAR activities including medical protocol drafting (including expanded scope of practice), medical trainings, mission participation, medical consultation, and prescribing medications for field use. The majority (69%) of those physicians were trained in emergency medicine, and 45% of the active medical directors had protocols allowing for an expanded scope of practice due to the remote nature of SAR medical care.
Conclusions
Intermountain West SAR teams vary in their activity, composition, training, and level of medical oversight. This study confirms that opportunities exist for physician integration with SAR teams in the studied states and likely throughout the United States.
Introduction
Search and rescue (SAR) teams are utilized to assist lost and injured backcountry travelers or to retrieve the deceased. The SAR teams of the Intermountain West states (Arizona, Colorado, Idaho, Montana, Nevada, New Mexico, Utah, and Wyoming) are likely some of the most active in the country (Figure 1). Currently, minimal data exist regarding these teams. This study sought to describe these SAR organizations, including call volume, membership, training for team members, and the level of field medical care that was provided to the ill and injured (Figure 2). Additionally, the involvement of physician medical direction and authorized expanded scopes of practice were investigated.
States comprising the Intermountain West region.
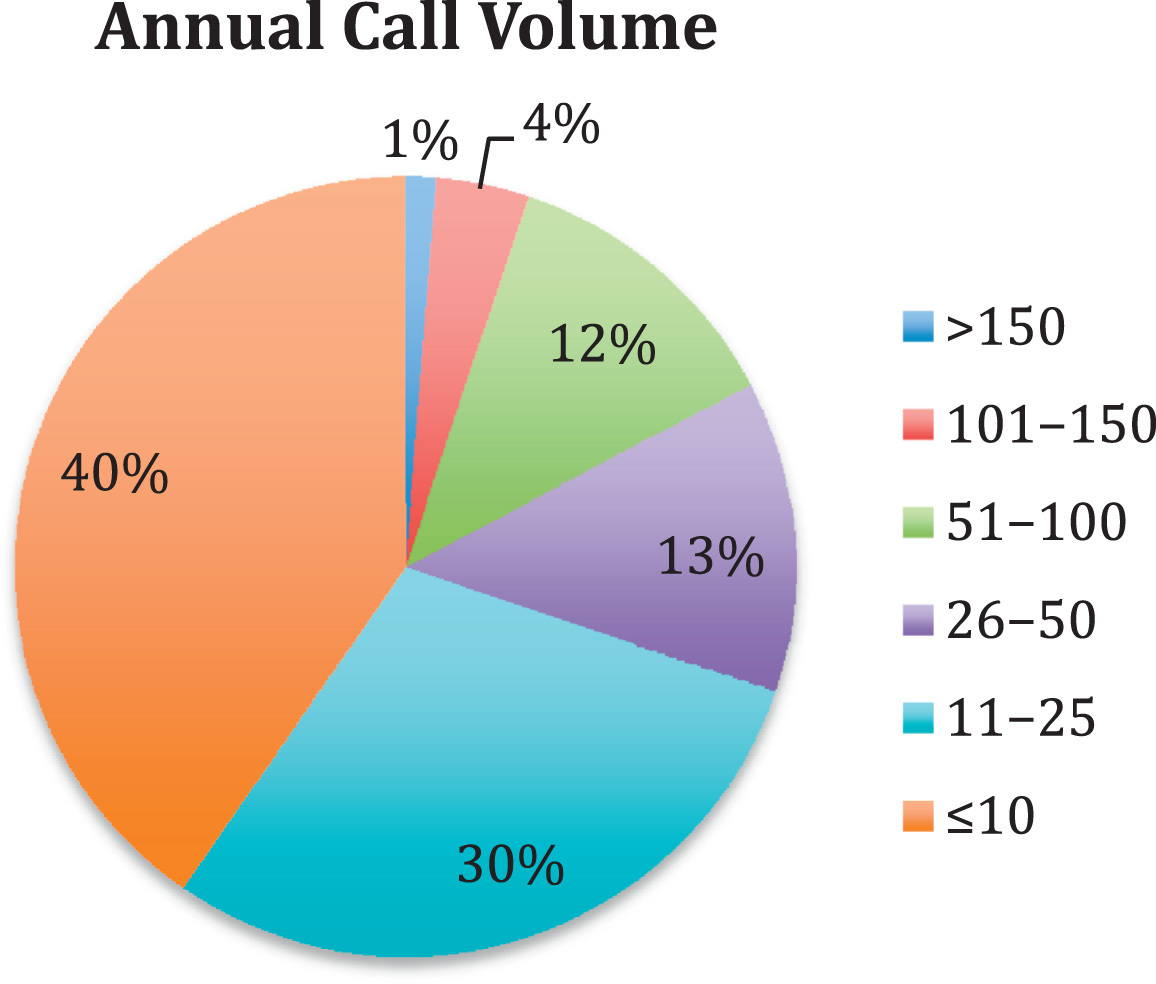
Average annual call volume for reporting search and rescue teams in the Intermountain West geographic area.
Methods
The SAR operations are typically the responsibility of the county sheriff’s office, so we began by contacting the sheriff’s department in all 281 counties in the Intermountain West. The one exception is the state of New Mexico, in which the State Police act as the SAR incident command, and we were able to obtain a list of all recognized SAR agencies within the state. A 15-question electronic survey was developed that queried call volume, team composition, training activities, and medical oversight and was sent to each county (Table). If no response to the initial e-mail request was received, additional e-mails and telephone calls were made to compile an accurate contact list. Results were descriptively analyzed using Excel (Microsoft, Redmond, WA) and SurveyMonkey (Palo Alto, CA). The University of Utah Institutional Review Board reviewed and approved our study.
Fifteen-question electronic survey developed to query call volume, team composition, training activities, and medical oversight
SAR, search and rescue; CPR, cardiopulmonary resuscitation; EMR, emergency medical responder; EMT, emergency medical technician; AEMT, advanced emergency medical technician; RN, registered nurse; APRN, advanced practice registered nurse; PA, physician assistant; MD, doctor of medicine; DO, doctor of osteopathy; EMS, emergency medical services.
Results
Of the SAR agencies contacted, 56% (156) of jurisdictions responded to the survey. The response rate for the individual states was as follows: 67% in Arizona (10 of 15), 56% in Colorado (36 of 64), 48% in Idaho (21 of 44), 41% in Montana (23 of 56), 59% in Nevada (10 of 17), 58% in New Mexico (19 of 33), 69% in Utah (20 of 29), and 74% in Wyoming (17 of 23). The mean annual call volume of responding teams was 29 missions (range, 0 to 154; Figure 2). The highest call volume teams were located in Clark County, Nevada (154), El Paso County, Colorado (152), and Boulder County, Colorado (146). Nine teams from the Intermountain West region reported an average of 0 missions per year. Teams were composed of on average 41 volunteers (range, 0 to 300) and 1 paid member (range, 0 to 26). Although the sheriff’s office in most communities is responsible for organizing SAR response, 76% of teams have someone other than the actual sheriff acting as SAR team commander.
Training offered to SAR team members is both technical and medical in nature. Instruction in a wide breadth of technical specialties is made available to SAR teams. The environments of the counties in which individual teams operate typically dictated the types of trainings conducted.
Most teams (67%) did not require medical training before joining but 79% of teams provided at least basic first aid and cardiopulmonary resuscitation (CPR) training to their membership. Multiple levels of medical training were represented on teams (Figure 3). The highest levels of medical training of SAR teams members were as follows: first aid/CPR (66%), emergency medical responder (17%), emergency medical technician (10%), advanced emergency medical technician (3%), paramedic (2%), registered nurse (1%), advanced practice registered nurse (0%), physician assistant (0%), and medical doctor/doctor of osteopathy (1%). Of these, 23% had additional formal training in wilderness medicine, such as a wilderness first responder course that focused on limited medical resources, extended patient care and difficult evacuation. Local emergency medical services (EMS) rather than SAR team personnel performed 60% of the medical care during missions. Of these local EMS providers, only 35% were cross-trained in SAR operations.
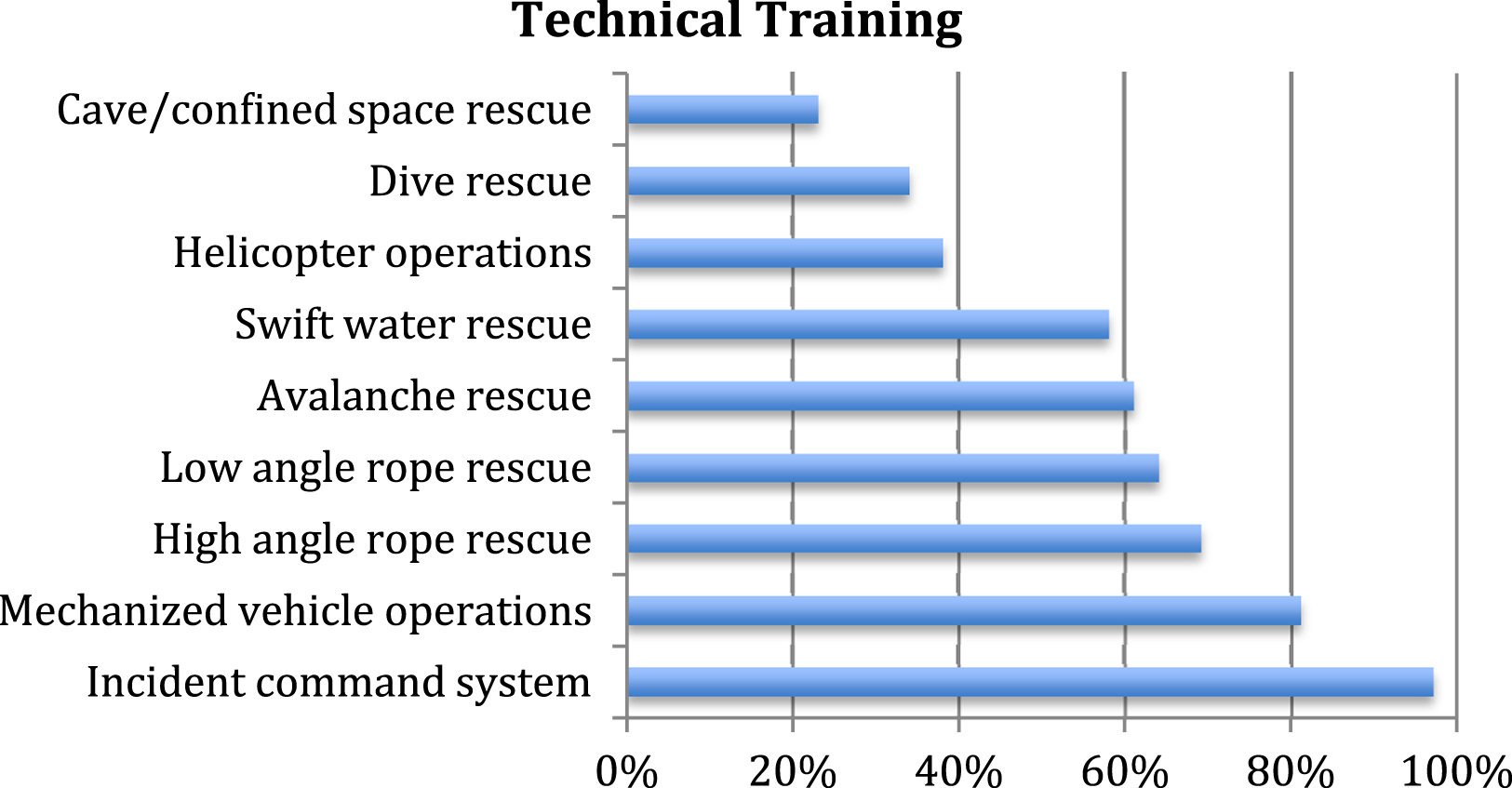
Percentage of Intermountain West search and rescue teams that provide specialized technical training.
Of the responding SAR teams, 41% had medical oversight physicians tasked with overseeing medical operations. Of these physicians, 69% were emergency medicine trained, followed by family medicine (23%), surgery (6%), and internal medicine (2%). Although there is a statistically significant association with counties that had higher call volumes and physician medical direction (two-sample t test: n1, 85; n2, 62; P < .0001), as many as 44% of teams (28 of 64) that respond to 20 or more annual calls had no physician-level medical oversight (Figure 4). Physicians participated directly during SAR missions and also indirectly through training programs. Reported activities of medical directors included creation of medical protocols, formal medical instruction, active participation on SAR missions, direct online medical consultation with field providers during missions, and prescribing medications.
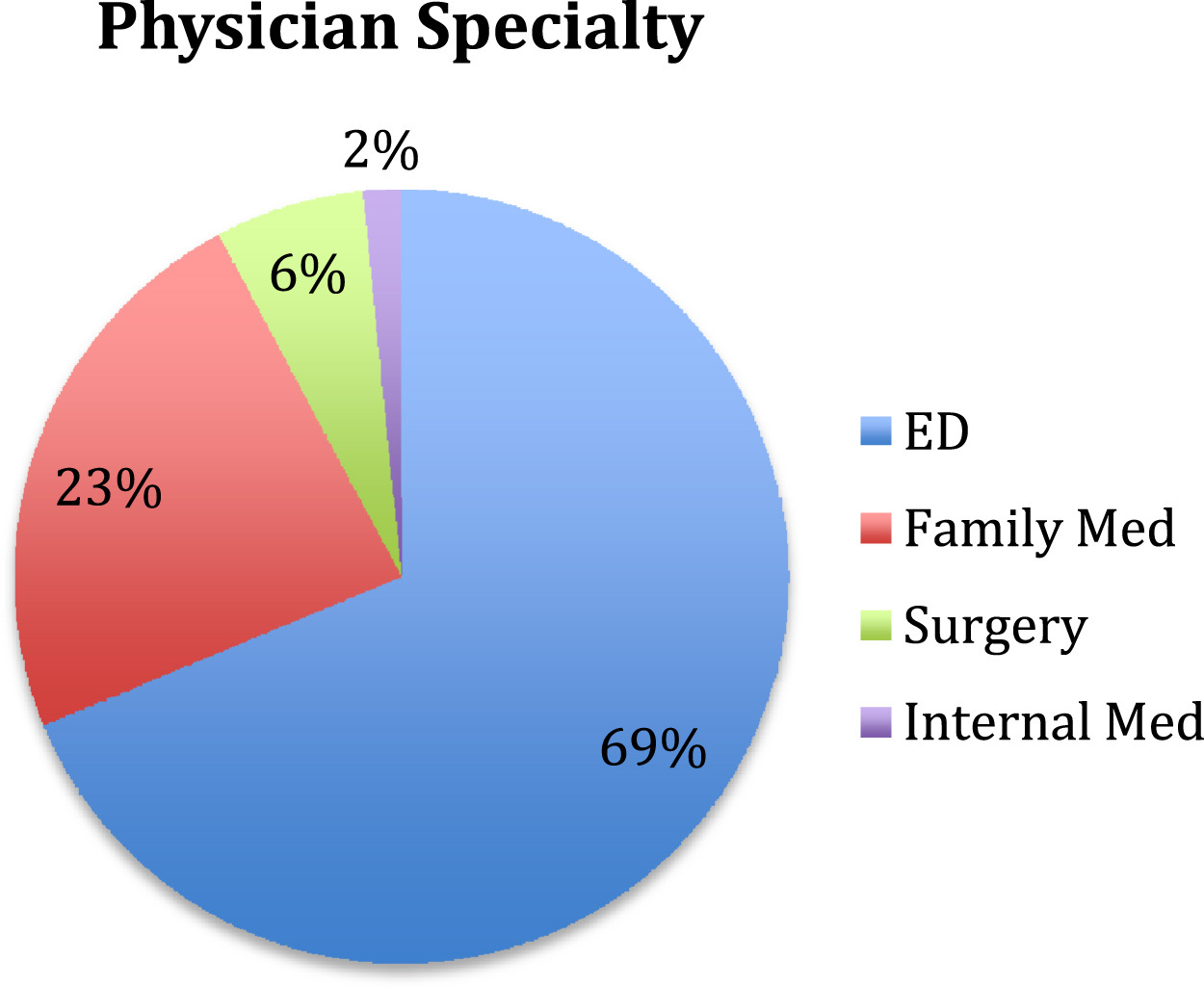
Relationship between call volume and medical specialty. ED, emergency department.
Forty-five percent of physician medical directors had protocols allowing for an expanded scope of practice due to the remote nature of SAR medical care. This expanded scope allowed wilderness providers to practice beyond their typical urban certification and skill set. Examples of expanded treatment options included intravenous access, medication administration, selective spinal immobilization, reduction of dislocations, and use of supraglottic airway devices.
Discussion
This study showed great variance among the Intermountain West SAR teams in their team composition, call volume, training, and level of medical direction. A thorough literature review revealed minimal formal research focused on these team variables in the region examined for this paper and also throughout the remainder of the United States.
Nearly all of the responding teams relied heavily on volunteer team members to execute their SAR missions. The exceptions to this trend were the rare instances when paid employees of the county sheriff’s department (sheriffs, deputies, and so forth) made up the entirety of the membership. Typically, limited training was required before full membership, and deficiencies were addressed with course offerings including first aid/CPR, swift water rescue, dive rescue, avalanche rescue, high-angle rope rescue, low-angle rope rescue, cave/confined space rescue, helicopter operations, mechanized vehicle operations, and the incident command system. These in-house sessions promoted safe and organized operations in the challenging and dynamic mission environments.
The results of this study confirmed the hypothesis that physician medical direction was underrepresented within the Intermountain West SAR community. The recent push for increasing physician involvement in prehospital medical direction extends to these remote environments as well. 1 The remote nature of the mission locations, the minimal medical equipment often available to austere care providers, and the extended patient care and extraction times demand a medical director knowledgeable and versed in all these traits.
Our findings that 59% of reporting SAR teams were without formal physician medical oversight suggests that opportunities exist for physicians to become involved on a volunteer basis with SAR teams in the Intermountain West, and likely other regions as well. 2 The required duties of medical directors have not been standardized but there are current efforts to create clear guidelines. 1 Those with previous experience creating prehospital protocols, online direction, and remote experience are best suited for these positions but others can learn these skills or borrow from successful programs. 3 Our results suggest that physicians from a variety of training backgrounds (emergency medicine, family medicine, surgery, internal medicine) are involved and can likely be successful in the SAR medical arena.
Certifications and licensure often limit the advanced care warranted by the ill and injured in remote environments. 4 For example, the scope of practice of an urban emergency medical technician does not include shoulder dislocation reduction but that may be required to decrease pain and increase mobility in a wilderness setting. Protocols that educate SAR teams to selectively immobilize (or not immobilize) the spine may allow a patient to self-evacuate rather than employ an extensive litter carry, which may pose a danger for rescuers as well as the victim, for a patient with very low risk of spinal injury. The expansion of standard urban scopes of practice is important in wilderness patient care and evacuation to definitive urban care. 5 The algorithms included in field-based practice scopes can greatly increase patient comfort and outcomes while promoting a safe and less difficult rescue. In the SAR environment, precedent exists for expanded care regimens including intravenous access, selective spinal immobilization, medication administration, dislocation reduction, and use of supraglottic airway devices to meet the unique demands of austere patient care and evacuation. Although these skills are taught in a variety of wilderness medical course types, legally they require physician oversight to be practiced in the field.4,5 Alteration of the traditional provider skill set requires both a comprehensive training program and legal documentation by a physician medical director.
Specific SAR medical direction skills and training can be obtained through numerous resources. 6 For those interested in medical direction or SAR activities, contacting local SAR commanders, typically the county sheriff’s office, is a suitable avenue to acquire team and membership information. The Wilderness Medical Society (WMS) and other organizations offer comprehensive guidance for care providers in the form of committee-driven treatment guidelines, annual conferences, and a variety of practical training modules. The WMS and the National Association of EMS Physicians host the Wilderness EMS Medical Directors course for interested practitioners. This specialized training highlights the knowledge and skills required to effectively provide medical oversight for a SAR agency.
This study has some clear limitations that are worth mentioning. Most notable is the response rate of 56%, which, while low, was not unexpected given the large number of volunteer agencies that we were attempting to contact. In reviewing the jurisdictions that did not respond, the authors considered that many of the nonresponders were from areas with little to no SAR activity. If those do truly represent less active SAR teams, then it is likely that their data would decrease the overall percentage of formal medical oversight in the Intermountain West. This finding can be interpreted in one of two ways: either more medical direction is warranted or, because the call volume is so low, medical direction is unnecessary. Further efforts to collect data from the nonresponding jurisdictions and a more detailed understanding of outcomes of SAR missions would clarify this point. Another potential flaw in our data is that many of the respondents were SAR coordinators or sheriff’s personnel who may have little understanding of medical terms and certifications. Thus, it is possible that the responses given do not accurately define the actual makeup of their teams. We attempted to use standard nomenclature, and every effort was made to define potentially confusing terms in the survey that was distributed.
Conclusions
Intermountain west SAR teams vary in their composition, training, and level of medical direction. Medical directors participate in a range of SAR activities including medical protocol drafting (including expanded scope of practice), medical training, mission participation, medical consultation, and prescribing medications for field use. The national push to increase medical oversight of prehospital services should also include remote SAR medicine. This study confirms that vast opportunities exist for physician integration into SAR teams in the surveyed states and likely throughout the United States.