
Abstract
We report the case of a 2-year-old Bedouin boy in whom developed severe and unusual complications after being stung, most probably, by the yellow scorpion Leiurus quinquestriatus hebraeus. Five hours after arrival to the emergency department, the boy had multisystem organ failure involving the central nervous system (seizure activity followed by coma with dilated, nonreactive pupils, and severe brain edema), shock (noncardiogenic), disseminated intravascular coagulation, renal failure, hepatic failure, and watery diarrhea, causing his death. In view of the relevant literature, we discuss the pathophysiologic events ultimately leading to his death.
Introduction
Between 30 and 40 infants and children are admitted every year to the Pediatric Intensive Care Unit (PICU) of the Soroka University Medical Center, Beer-Sheva, Israel, for general intoxication due to scorpion sting. In most cases, envenomation is caused by the yellow scorpion Leiurus quinquestriatus hebraeus, the most common and most dangerous scorpion species in the Negev desert of southern Israel (Figure 1). 1 –3 In the majority of cases, the scorpion is identified by the child, the parents, or the medical staff. In other cases, envenomation by the yellow scorpion is presumed by history and by the typical signs and symptoms, 2 which include stimulation or depression of the central nervous system (CNS) and stimulation of the sympathetic or parasympathetic nervous system, with the additional sign of priapism in males nearly pathognomonic for scorpion sting. In the most severe cases, heart failure, pulmonary edema, and cardiogenic shock are known as devastating complications. 4 –8 In the current communication, we describe a young boy who had brain edema, noncardiogenic shock, and coagulopathy several hours after envenomation that finally caused his death. We are not aware of similar complications after envenomation by the Leiurus quinquestriatus, nor by other scorpion species.

The yellow scorpion Leiurus quinquestriatus hebraeus.
Case Presentation
A 2-year-old, previously healthy, Bedouin boy was found in an open field adjacent to his hut, unconscious and sweating. According to the parents, he was unattended for several minutes. They denied trauma or ingestion of any drugs or pesticides (and stated that none is in their possession), but described that there were a large number of yellow scorpions in the surrounding area. Upon arrival at the Emergency Department (ED), the boy had no signs of trauma; he had altered mental status and was irritable, with an increase in muscle tone. His extremities were cold, and he had marked diaphoresis. Vitals signs showed normal respiratory rate, tachycardia of 148 beats/min, blood pressure 124/76 mm Hg (above the 95th percentile for age), elevated body temperature of 38.2°C, and normal oxygen saturation at 96% in room air. Otherwise, his physical examination was unremarkable except for a pronounced priapism. Blood tests showed mild hyperglycemia, slightly increased urea nitrogen, leukocytosis, and mild metabolic acidosis (Table 1).
Laboratory results on arrival and after patient's admission
AST, aspartate aminotransferase; ALT, alanine aminotransferase; WBC, white blood cell count; PLT, platelets; PT, prothrombin time; INR, international normalized ratio; PTT, partial thromboplastin time; BE/BD, base excess/base deficit; AChE, acetylcholinesterase; NA, not available.
Two hours after deterioration.
Results drawn after plasma, platelets and blood transfusion.
Blood sample taken while patient breathing room air.
Blood sample taken while patient was mechanically ventilated on supplemental oxygen.
The child's history, physical examination, laboratory results, and most typical presentation all suggested a yellow scorpion sting. 1 –3 He was admitted to the PICU, and according to the PICU's scorpion envenomation protocol, he was given intravenous maintenance fluids (5% glucose/0.33% NaCl solution) and a continuous drip of midazolam (0.1 mg·kg−1·h−1) and fentanyl (1 μg·kg−1·h−1) for pain and irritability. Echocardiography showed normal heart function with fractional shortening of 31%, (normal >28%); normal left ventricular end-diastolic dimension of 29 mm, and left ventricular end-systolic dimension of 19 mm, with no mitral valve regurgitation.
Four hours after PICU admission, the patient had a generalized tonic-clonic seizure, which ended with intravenous administration of 1 mg diazepam. His condition rapidly deteriorated, however, to a state of shock with profound cardiovascular collapse. Fluid resuscitation was started immediately (0.9% NaCl crystalloid solution followed by fresh frozen plasma), along with tracheal intubation and mechanical ventilation, and 5 mL antivenom serotherapy was given intravenously (although not routinely given in our unit 3 ). The available antivenom, prepared in donkeys, is specific to the venom of the yellow scorpion Leiurus quinquestriaticus (processed and supplied by Central Laboratories, Israeli Ministry of Health, Jerusalem, Israel). (According to the manufacturer's instructions, each milliliter neutralizes at least 80 LD50 of the venom in 20-g mice.) That was followed by establishment of central arterial and venous catheters. Continuous inotropic and vasopressor support with dopamine and dobutamine (both reached maximal dose of 20 μg·kg−1·min−1) and adrenalin at 1.5 μg·kg−1·min−1 were given, and the dose was quickly increased. Nevertheless, severe hypotension continued for 6 hours. A broad-spectrum antibiotic was administered with ceftriaxone intravenously, after drawing blood for culture. Anticonvulsant treatment was started with a loading dose of intravenous phenytoin and was followed by maintenance treatment.
The patient had remained unconscious since the initiation of the seizure episode, and he rapidly deteriorated to a comatose state with Glasgow Coma Score of 3 and dilated nonreactive pupils. Disseminated intravascular coagulation with thrombocytopenia, prolongation of his prothrombin time and partial thromboplastin time tests, and decreased hemoglobin were treated with blood and blood products. He also began to have watery diarrhea, renal failure, and acidosis. His blood tests during the following hours showed signs of liver function impairment with elevated liver enzymes and hypernatremia (Table 1). Although repeated echocardiography examination showed normal cardiac function during the entire admission, noradrenalin had to be added owing to ongoing hypotension. Brain imaging was considered but delayed because of his unstable condition.
Two days after admission, a computed tomography scan showed extensive brain edema and ischemic changes (Figures 2A and B) with typical “reversal sign” 9 and signs of transtentorial herniation. Therapy was started with mannitol and mild hyperventilation but clinical deterioration followed, and brain death was declared 8 days after admission. Bacterial blood culture showed no growth. Postmortem examination was not granted by the parents.
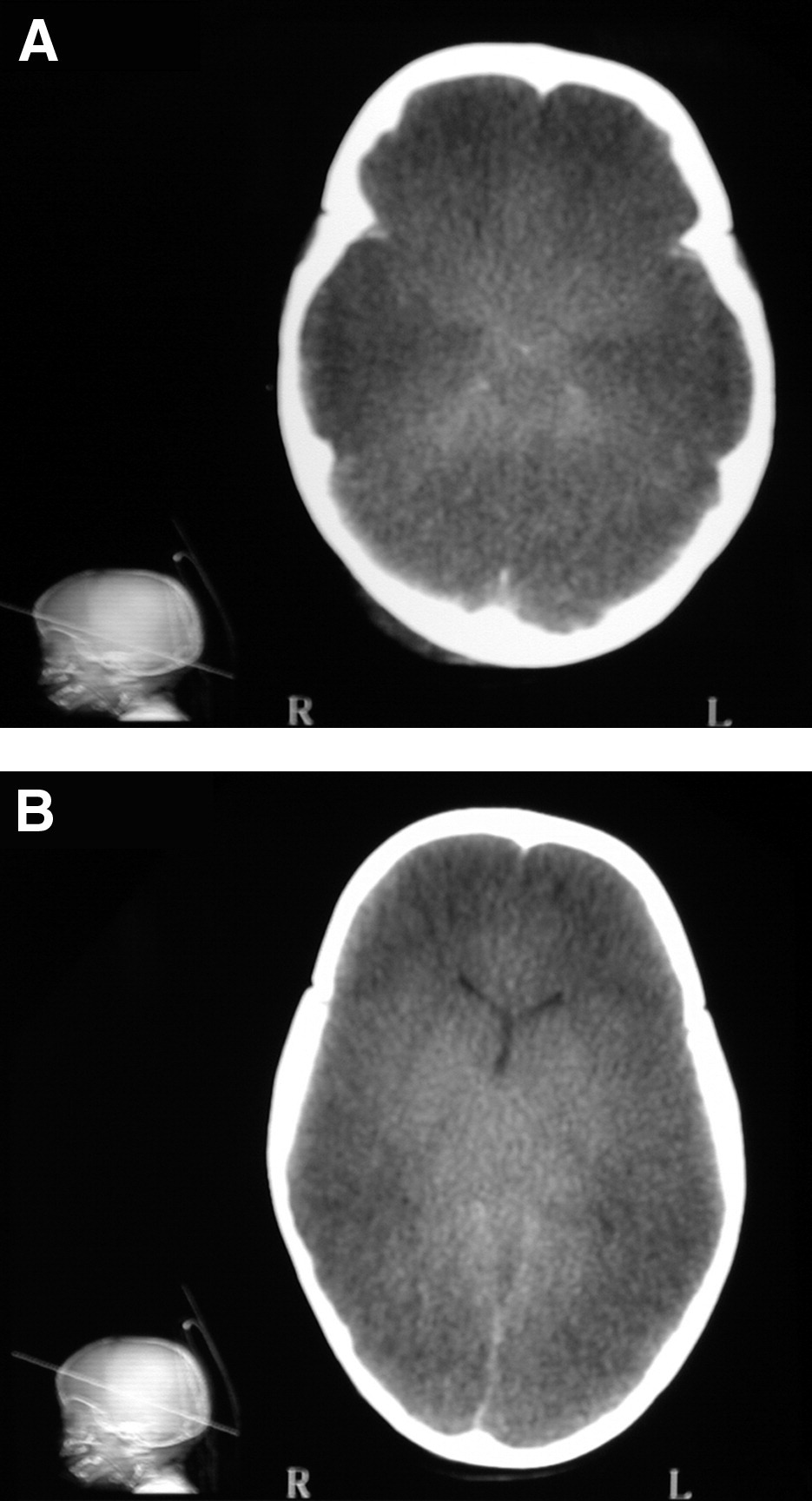
(A, B) Two representative slides of the patient's computed tomography scan demonstrating extensive brain edema, diffuse decreased attenuation, and loss of gray-white matter differentiation, with relative increased attenuation of the basal ganglia, effacement of the sulci, and obliteration of the basal cistern and the fourth ventricle.
Discussion
Death from scorpion sting is uncommon in our institution. Since the establishment of our PICU in 1982, only 5 children have died of scorpion envenomation, among more than 700 children admitted with general intoxication after scorpion sting. Three of the 5 died of cardiogenic shock and ventricular arrhythmias,3,8 1 child died of sepsis, 10 and the fifth child, presented here, died of brain edema caused by transtentorial herniation concomitantly with severe noncardiogenic shock, coagulopathy, and multiple organ failure. We are not aware of any similar descriptions of pathophysiologic events and clinical deterioration after scorpion sting in the literature. Although the individual features of encephalopathy, severe shock, disseminated intravascular coagulation, diarrhea, acidosis, and renal and hepatic dysfunction may be seen in a wide range of disorders, including septicemia, cardiogenic shock, heatstroke, and the effect of severe hypoxia, all of these can be distinguished from the illness presented in our patient. Septicemia was excluded by negative microbiological results. Cardiogenic shock was excluded by recurrent normal echocardiography examinations before and after the shock episode. There was no clinical or laboratory evidence of substantial hypovolemia, and no documented hypoxemia after the patient's arrival to the ED and the PICU.
Although scorpion venom has no direct coagulopathic effects, we have to assume that the disseminated intravascular coagulation was secondary to the shock. The appearance of shock after seizures, with immediate dilated unresponsive pupils and coma, seems to originate from a CNS injury. In cases of hypovolemic or cardiogenic shock, patients usually do not deteriorate as rapidly and pupils do not become dilate within minutes. Distinct cortical deterioration before any other organ deterioration was reported by Ismail et al 11 in 4 fatal cases of children admitted with severe hyperthermia (3 children) or hypothermia (1 child) after scorpion sting. The children had signs of encephalopathy manifested by agitation and seizures, followed by isoelectric encephalograms before cardiac manifestations. In another study of 9 fatal cases, the same authors documented CNS manifestations that preceded the terminal hypotension and cardiac arrest. 12 It has been suggested that CNS manifestations are due to the penetration of the venom through the blood-brain barrier, which is known to have relatively increased permeability in young children. Computed tomography scans were not performed in these cases, and, therefore, brain edema and tentorial herniation cannot be excluded. Symptoms of systemic intoxication after scorpion sting may be caused by the venom (toxins) itself, neurotransmitters (catecholamines), and proinflammatory cytokines released by the venom. 10 ,13–15 Central nervous system–related symptoms may include irritability, tremor, and altered level of consciousness as well as coma, convulsions, hypothermia, or hyperthermia. 7 ,11,12,16
There are also a few reports of brain infarcts after scorpion sting. One report from our area describes two 7-year-old children, one with hemiparesis and the other with hemianopsy and one-sided no. 7 cranial nerve paralysis. Both children were stung in the face. 17 The authors of that report suggest that the anatomic proximity of the stings to the CNS may have been significant in the etiology of infarct development. Most reports of cerebral infarcts come from India, and the suggested etiologies are thrombotic episodes, 18 reduced blood flow in the carotid arterial system due to vasospasm related to the autonomic storm, 19 and disseminated intravascular coagulation. 20 In a report from Mexico, 21 magnetic resonance imaging showed signs of brain infarction with no vascular occlusions, suggesting hypotension or shock as the cause of cerebral infarction.
Brain edema as a primary cause of death after scorpion envenomation has not been previously described. Cupo et al 22 describes brain edema as an incidental finding in postmortem examination of 3 children who succumbed to cardiorespiratory failure after scorpion sting. This case of rapidly developing acute severe encephalopathy and shock resembles previously reported series and cases of hemorrhagic shock and encephalopathy syndrome in young infants. 23 –25 The main features of this syndrome include sudden shock, encephalopathy, seizures, disseminated intravascular coagulation, watery diarrhea, acidosis, hypernatremia, renal failure, and elevated liver enzymes. 23 –25 Computed tomography scan and postmortem examinations were significant for severe brain edema and cerebral herniation from unclear etiology.23,24 All these features emerged in our child. The etiology of hemorrhagic shock and encephalopathy syndrome is unknown. Many factors, including metabolic disorders and different infectious etiologies, were examined and ruled out. 23 –25 This entity, however, does resemble heat stroke in many aspects.25,26 Elevated body temperature is a common sign of scorpion envenomation, but it was only mildly elevated (38.2°C) in our child.
Summary and Limitations
First, because scorpion sting was not documented in this case, one can argue that this previously healthy 2-year-old child might have had some other intoxication or disease. We think that is highly unlikely. The combination of sudden decrease of consciousness, irritability, intense perspiration, and priapism in a male is nearly pathognomonic for scorpion envenomation in our area. Acetylcholinesterase inhibitor insecticide intoxication was excluded, as the serum pseudo acetylcholinesterase level was above normal (Table 1). Second, one may argue that the child had respiratory failure (apneic episodes or hypoxemia) or cardiac manifestations (ventricular arrhythmias) or high fever immediately after the sting and before arrival to the ED that caused hypoxic ischemic encephalopathy and anoxic multisystem organ failure. That is unlikely because respiration, heart rhythm, blood pressure, and blood tests, including blood gases, were all normal or nearly normal (except for leukocytosis, a common feature in scorpion envenomation) upon arrival at the ED and in the PICU.
In conclusion, we assume that this boy had an unusually severe brain insult either due to direct CNS toxicity (penetration of the toxins through the blood-brain barrier, affecting the CNS neurons) as suggested by Ismail et al, 12 or due to an unusual secondary effect of neurotransmitters and proinflammatory cytokines on blood vessels that caused brain ischemia and cytolytic brain edema. Because this devastating complication is very rare, we cannot comment on possible preventable effects of specific scorpion antivenom given to victims upon arrival at the clinic.