
Abstract
Background
Scorpion sting envenomation is a life-threatening emergency and a common public health problem in many regions of the world, particularly in children. Children are at greater risk of developing severe cardiac, respiratory, and neurological complications.
Objectives
The aims of this study were to evaluate demographic, clinical, laboratory, treatment, and outcome characteristics for pediatric patients with scorpion sting envenomation in southeast Turkey and to describe features that may be predictive of the need for pediatric intensive care unit (PICU) care.
Methods
A total of 52 charts of children (mean age: 7.7 ± 2.8 years; age range: 1.5–15 years) presenting with scorpion sting envenomation to a single hospital in southeastern Turkey were investigated. General characteristics of the children, species of the scorpions, anatomic site of the sting, clinical and laboratory findings, treatment approaches, complications, and outcomes were recorded.
Results
Twenty-four stings (46.2%) were inflicted by Androctonus crassicauda, 1 (1.9%) by Leiurus quinquestriatus, and the sources of the other stings were not known. Thirty-one patients (59.6%) were admitted from rural areas. Admission from a rural area was a significant risk factor for severe envenomation. Foot-leg was the most frequently stung part of the body (48%). The greatest number of stings occurred in the summer (78.8%). Cold extremities and tachycardia were the most frequently seen clinical findings (38.4% for both). Twenty patients (38.5%) had signs of serious envenomation and required admission to the PICU. Hemoglobin, white blood cell count, activated prothrombin time, aspartate aminotransferase, alanine aminotransferase, and creatine phosphokinase levels were higher in severely envenomed children compared to levels in those with mild-moderate stings. Antivenom was given at a primary or secondary health center before arrival to our hospital in 44 (84.6%) patients, without any apparent difference in the number of patients presenting with mild-moderate and severe envenomed stings. All patients recovered after treatment except for 1 child who died with severe pulmonary edema.
Conclusions
We found no clinically useful demographic or epidemiological data to guide decision making regarding the need for PICU admission for pediatric victims of scorpion sting in our area. Decisions on transfer and admission to a PICU should be based on the development of systemic findings of envenomation.
Keywords
Introduction
Scorpion envenomation is common in certain areas of the world including the Middle East, Latin America, Africa, and India. 1 Factors that can affect the severity of scorpion envenomation are the anatomic location of the sting as well as the age, weight, and health status of the victim. 2 Children are more susceptible to scorpion envenomations, and the clinical manifestations of envenomation may be more severe in children and may result in multi-organ failure and death. 3 The clinical manifestations of scorpion envenomation appear to be secondary to activation of both the sympathetic and parasympathetic nervous systems. Although the venoms of certain species may produce apnea, bradycardia, and hypotension, more commonly activation of the sympathetic nervous system leads to hypertension and pulmonary edema. Severe scorpion envenomations, characterized by cardiovascular, pulmonary, and neurological manifestations, can be life threatening as a result of complications such as myocardial dysfunction, shock, pulmonary edema, or hypertensive encephalopathy. Scorpion toxins also may produce severe central nervous system manifestations, including marked irritability and unconsciousness. 4
As in other areas of the Middle East, Androctonus crassicauda and Leiurus quinquestriatus are the main scorpion species of southeast Anatolia 5 that can cause severe autonomic and central nervous system abnormalities and cardiac and respiratory dysfunction. As a result of the potential threat to life, it may be reasonable to hospitalize all children stung by a scorpion regardless of the clinical severity. However, routine admission to a pediatric intensive care unit (PICU) is unreasonable because of cost issues and the manpower intensity associated with PICU services. 6 Thus, identifying factors that may predict which patients will need PICU care is very important. The aims of this study were to evaluate demographic, clinical, laboratory, and treatment characteristics as well as outcomes in our pediatric patients with scorpion sting envenomation and to describe features that may be predictive of the need for PICU care.
Materials and methods
Patients
This was a retrospective study of the medical records of all children diagnosed with scorpion envenomation who were admitted to Dicle University Hospital over a 12-month period extending between January 2005 and January 2006. Dicle University Hospital is a referral hospital in southeast Turkey and receives nearly all children with scorpion stings who present to other primary and secondary health centers.
Cases were admitted to our Pediatric Emergency Unit, and initial evaluation and management were performed by emergency staff. The diagnosis of scorpion envenomation was based on a positive history of scorpion sting, with a scorpion being seen or killed by relatives or a bystander.
Intravenous antivenom was given if it had not been administered at the referring hospital. The antivenom used was purified polyvalent anti-scorpion serum produced by the Refik Saydam Hygiene Center in Turkey. Tetanus toxoid was also given when indicated. After initial care, all patients were hospitalized. Blood pressure, pulse rate, body temperature, respiratory rate, oxygen saturation, and level of consciousness were monitored. Children with altered mental status or with findings of autonomic storm, vomiting, seizures, dyspnea, and pulmonary edema, either before or after admission to our hospital, were transferred to the PICU. Mildly-moderately envenomed patients were managed in regular wards. After antivenom administration, treatment consisted primarily of supportive care. The PICU of Dicle University Hospital is a multidisciplinary regional referral center, with a 7-bed unit treating approximately 500 critically ill children per year.
Demographic data, geographical location in which the sting occurred, sting locations on the child's body, time intervals from sting to admission to hospital, local and systemic signs and symptoms of envenomation, results of hematological and biochemical laboratory tests, management, length of hospital stay, and outcome were recorded. In terms of geographical location, villages were considered to be rural areas, and towns and city centers were considered to be urban areas.
Patients were classified into 2 groups depending on the severity of clinical findings (mild-moderate and severe). These grades were determined for this study by one of the authors (M.B.) based on review of the charts. Mild-moderate envenoming included asymptomatic patients, those with only local pain, those with less severe systemic findings (such as nasal pruritus), foreign body sensation in the throat, sialorrhea, dysphagia, irritability, tachycardia, tachypnea, and mild to moderate breathing difficulties. Severe envenoming included patients with nystagmus, severe breathing difficulties, lethargy, stupor, coma, focal or generalized seizures, increased muscular tone, low blood pressure, cardiac failure, and/or acute pulmonary edema. 7
Laboratory Investigations
Laboratory investigations were performed in all children to measure the following variables (using standard laboratory methods): hematocrit, hemoglobin, white blood cell count (WBC), platelet count, activated partial thromboplastin time, prothrombin time, international normalized ratio, serum glucose, urea, creatinine, total bilirubin, alanine aminotransferase (ALT), aspartate aminotransferase (AST), alkaline phosphatase, creatine phosphokinase (CPK), lactate dehydrogenase, sodium, potassium, chloride, and calcium. Arterial blood gases, including arterial blood oxygen saturation, were also measured. Electrocardiography was performed in all patients, but echocardiography was used only selectively.
Statistical Analysis
The values were expressed as mean ± SD. Comparison between mild-moderate and severe patients was done by Mann-Whitney U test or χ2 test. Statistical analyses were performed using SPSS version 12.0 (SPSS Inc, Chicago, IL). A P value less than .05 was considered significant.
Results
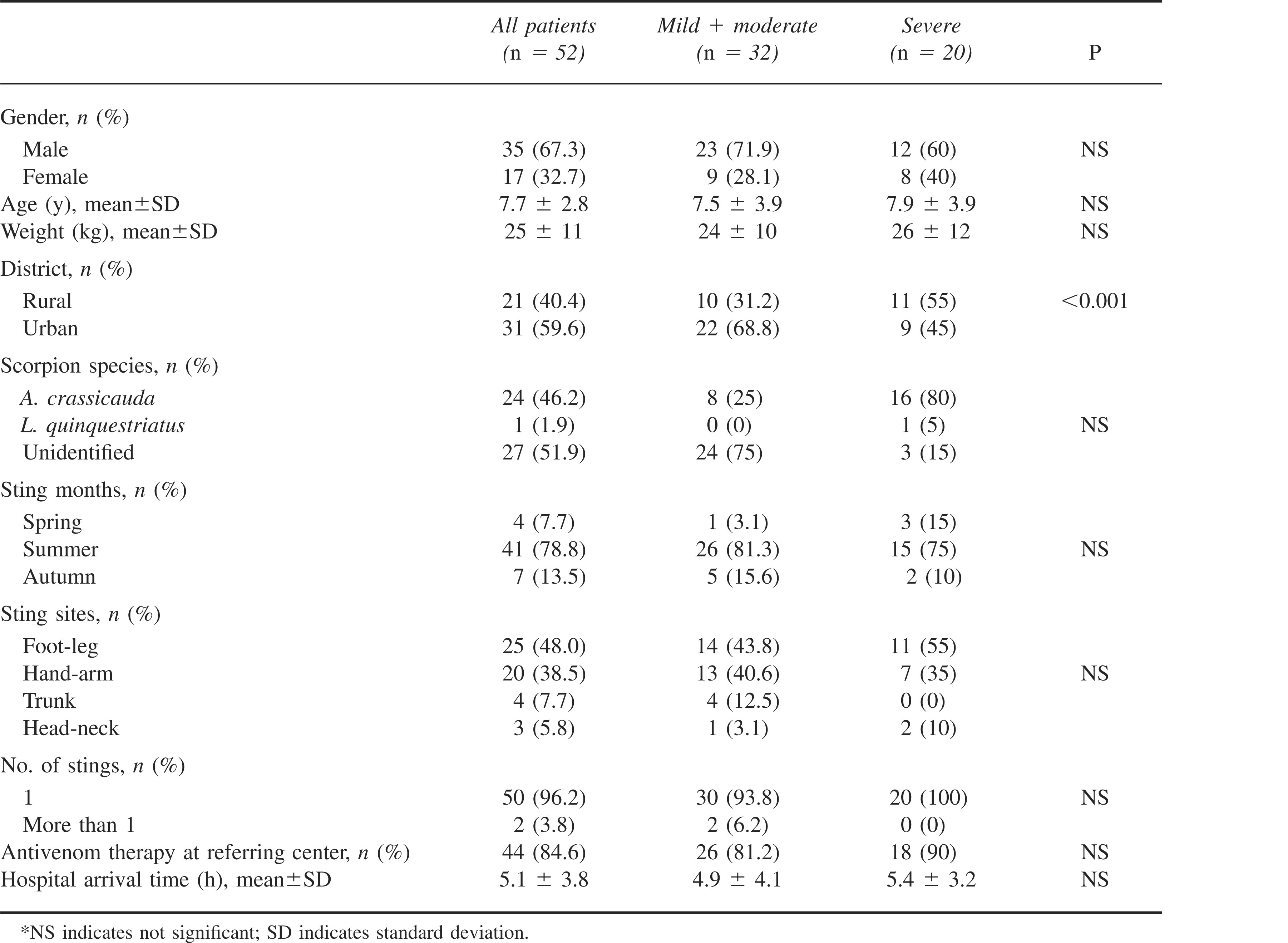
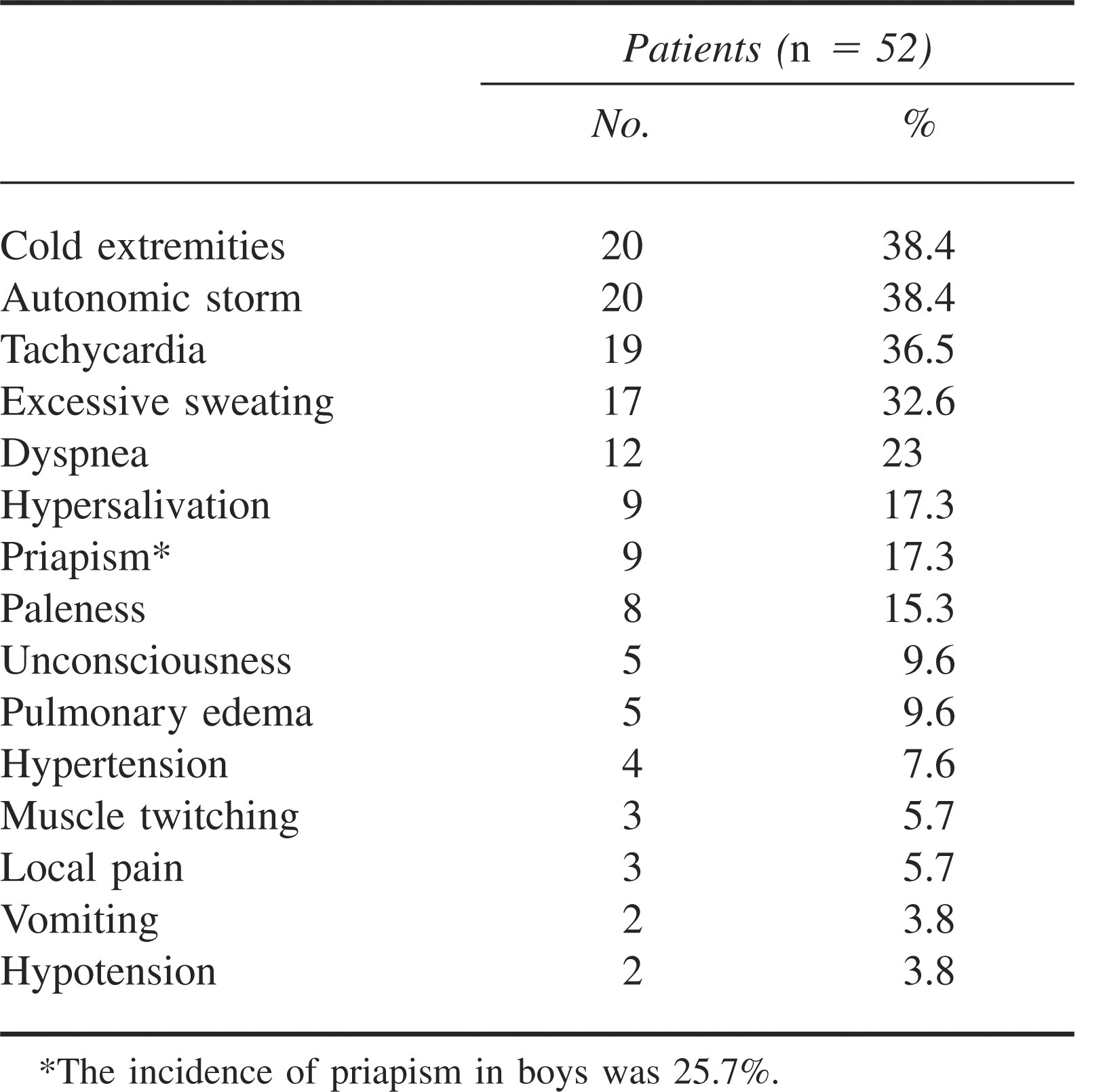
The study population consisted of 52 children (male: 35; female: 17) aged 7.7 ± 2.8 years (range: 1.5–15 years). Thirty-two (61.5%) patients were classified as mild-moderate (MME), and 20 (38.5%) were classified as severe (SE). Demographic and epidemiological characteristics of the patients are shown in Table 1. Sex distribution, mean age, and weight of children were found to be similar between the MME and SE groups (P > .05). Children in the SE group were more frequently from rural areas (P < .05). The distribution of sting months, sting hours, sting sites, scorpion species, number of stings, and hospital arrival time were similar in both groups (P > .05). Cold extremities due to vasoconstriction (38.8%), tachycardia (36.5%), and excessive sweating (32.6%) were the most prominent clinical findings on admission to the hospital (Table 2). Laboratory findings of patients on admission to hospital are shown in Table 3. Electrocardiographic changes were not seen in our series, except for sinus tachycardia in 19 patients (Table 2).
Demographic and epidemiological characteristics of children stung by scorpions in southeast Turkey over 12 months
Frequency of the clinical symptoms on admission to the hospital
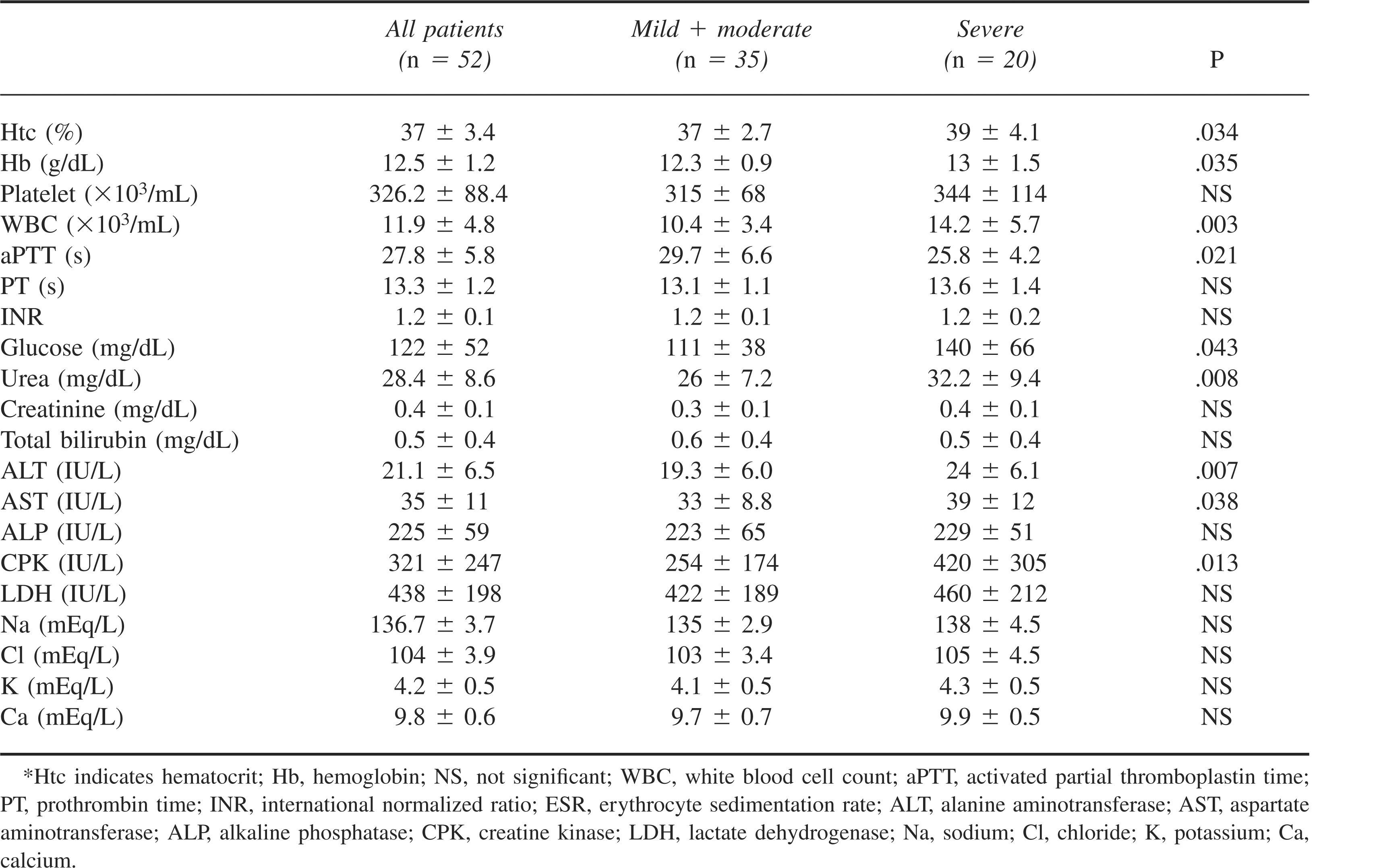
Laboratory findings of patients on admission to the hospital (mean±SD)
Antivenom therapy was used in 44 (84.6%) patients at a primary or secondary health center before arrival to our hospital. Twenty-six patients were in the MME group (81.2% of MME patients) and 18 were in the SE group (90% of SE patients) (P > .05). Antihistamines and steroids were administered in nearly all patients (98% for both) at the referring centers. One additional vial of antivenom was given to 7 (13.4%) patients in the SE group. Sodium nitroprusside for hypertension (n = 3, 5.8%), prazosin for autonomic storm (n = 20, 38.5%), and dopamine for hypotension (n = 2, 3.8%) were used exclusively in children in the SE group. One of these children died as a result of cardiac and respiratory arrest. This patient arrived from a rural area and was in very poor clinical condition, with cardiac and respiratory instability at the time of admission to hospital. Mechanical ventilation was not needed in any patient except the one who died. Surviving patients were discharged from the hospital in 2.5 ± 1.2 days in apparent good condition. There were no adverse reactions to any of the drugs administered, including no antivenom reactions. There was no significant difference in length of hospital stay between SE and MME groups (2.8 ± 1.3 and 2.2 ± 1.2 days, respectively).
Discussion
In Turkey, in terms of public health, important scorpion species are identified as A crassicauda, L quinquestriatus, Mesobuthus gibbosus, and Mesobuthus eupeus—all of which are members of the Buthidae family. 8 In our series, identification of scorpions showed that 24 stings (46.2%) were inflicted by A crassicauda and 1 (1.9%) by L quinquestriatus. A crassicauda venom has an intravenous lethal dose, 50% (LD50) in mice of 0.32 ± 0.02 mg kg−1, which makes it one of the most toxic species of scorpion in the world.9,10 This scorpion has been reported to be the most toxic and frequent scorpion species of the Arabian Peninsula and southwest Iran, which neighbor our region.4,11
The mean age of the patients in our series was 7.7 ± 2.8 years. Young children may be stung as a result of careless behavior, such as walking barefoot, lifting up stones, and putting on clothes and shoes without checking them for the presence of scorpions. Parental awareness of these issues should be stressed as a preventative measure.
In this study stings occurred to lower or upper extremities in 86.5% of the cases, a frequency similar to that provided by previous reports.2,4,12 This is likely due to factors including the high level of agricultural activity in rural areas, the frequency of wearing sandals or walking barefoot, the habit of putting on shoes without preshaking them, and hand searching for scorpions in homes. 13 People are stung by scorpions on their extremities because that is the body part they present most commonly to the scorpion.
In our study, male children predominated over females (67.3% vs 32.7%). Several authors have found similar results in terms of higher numbers of stings in boys than in girls.14,15 Boys probably go outside more commonly and often play in places where scorpions live, such as rubbish areas in our country.
Pulmonary edema developed in 9.6% and dyspnea in 23.0% of our patients. Acute pulmonary edema has been attributed to acute left ventricular failure due to massive release of catecholamines or myocardial injury induced by the venom.16,17 Cardiogenic shock and pulmonary edema are the leading causes of death after scorpion envenomation4,18; however, breathing disturbances have also been observed in patients without pulmonary edema or myocardial damage after scorpion envenomation. 19 In our series, predominant signs involving the cardiovascular system were tachycardia (36.5%), dyspnea (23.0%), and paleness (15.3%). Hypertension (7.6%) and hypotension (3.8%) were rare on admission to our hospital. On the other hand, there were also manifestations of cholinergic stimulation, including excessive sweating (32.6%) and vomiting (3.8%). Systemic findings have previously been reported to be more frequent in children. 2 Although age and weight of children are reported to be risk factors for developing severe reactions to envenomation from scorpion stings,4,6,12 we did not find age or weight differences between cases with SE and MME in our study. This may be due to the fact that the mean age of the patients was relatively high in our study group.
The clinical manifestations of scorpion envenomation are predominantly sympathetically and parasympathetically mediated, depending on the scorpion species. 4 Systemic effects of scorpion envenomation include massive autonomic neurotransmitter release (autonomic storm, adrenergic or cholinergic) as a result of the excitatory neurotoxins of scorpion venom. 20 Autonomic storm was observed in 38.4% of our study group, and 5 (9.6%) patients had pulmonary edema. It is known that scorpion venom contains neurotoxins that act by opening up the sodium channels at pre-synaptic nerve terminals, thereby initiating autonomic storm. Alpha-receptor stimulation by the scorpion toxin plays a major role, resulting in hypertension, tachycardia, myocardial dysfunction, pulmonary edema, and cool extremities. 21 The unopposed effects of alpha-receptor stimulation lead to suppression of insulin secretion, hyperglycemia, and free radical accumulation injurious to myocardium. 3 Previous studies on scorpion envenomation reported left ventricular dysfunction, myocarditis, respiratory failure, and pulmonary edema in victims of scorpion stings.22,23
The mean hospital arrival time in our study was 5.1 ± 2.8 hours. No association was found between degree of severity and hospital arrival time. It has been suggested that delay in scorpion antivenom administration could reduce its effectiveness. 1 Most of our patients (84.5%) received antivenom at primary and secondary health institutions before arrival to our hospital. No information was available, however, regarding the time interval between stings and antivenom administration. It could be possible to question the beneficial effect of antivenom in scorpion sting envenomation, since there were no significant differences regarding prior antivenom injection and the number of MME and SE group patients. However, it is not possible to clearly conclude that these patients would not have been much sicker if they had not received antivenom.
Higher levels of hematocrit, hemoglobin, WBC, blood urea nitrogen, and glucose in the SE group compared to the MME group might have occurred as a result of fluid loss secondary to excessive sweating, vomiting, and stimulation of the autonomic nervous system (Table 3). Activated partial thromboplastin time shortening may have been due to an acute phase response of scorpion envenomations, as occurs in early-phase disseminated intravascular coagulation. 24 It was thought to have no clinical significance. We have observed this finding also in snakebite envenomation in our center. 25 Higher AST, ALT, and CPK levels may be signs of cardiac and/or skeletal muscle injury. Sofer and co-workers 26 reported raised CPK levels in all degrees of scorpion envenomations, which reflects the increased skeletal muscle activity due to the sting.
Neurological manifestations such as agitation, convulsions, and coma were also seen in our patients. Ten (19.2%) patients developed impaired consciousness, and 5 had coma. Neurological manifestations can be explained by hypertensive encephalopathy or brain ischemia. 27 Neurological manifestations have been observed in severe scorpion-envenomed patients and are correlated with poor outcome.28,29 One of our 5 comatose patients died.
Priapism was noted in 25.7% of boys and resolved without any specific therapy in 1 ± 0.2 days.
The treatment of scorpion envenomation is mainly based on supportive care, symptomatic relief, and the use of specific scorpion antivenom. An intravenous line should be placed for administration of scorpion antivenom and other medications as needed. Mild symptoms should be controlled with non-narcotic analgesics and antihistamines. 7 Antihistamines and steroids had been administered to nearly all patients in our study (98.0%) before admission. Although not protocol driven, use of these agents was found to be a common approach of primary care doctors in our region.
As a result of the risk of adverse reactions, scorpion antivenom should be used only when moderate or severe findings are observed. Scorpion antivenom is the only specific treatment and is widely used in many countries. 1 Scorpion antivenom has been shown to neutralize toxin in humans and to prevent its cardiac and neural effects in experimental animal studies, and, thus, very early antivenom administration may diminish the severity and duration of sympathetic hyperstimulation. 30 –32 To the contrary, however, Abroug et al 1 did not find any beneficial effects of antivenom when it was given in the first 30 minutes of sting when compared with those who were treated in less than 1 hour. However, a limited number of severe stings in the latter study makes it difficult to derive firm conclusions about the effect of scorpion antivenom in patients with severe clinical manifestations. Bawaskar and Bawaskar33,34 concluded that scorpion antivenom is no more effective at alleviating or reversing the cardiovascular effects of scorpion venom in severe cases when compared to prazosin, which prevents and reverses the cardiovascular manifestations of severe scorpion envenomation. Antivenom was given to all patients in our study, with 84.6% of children receiving antivenom at the referring center and others received it on admission. In 13.4% of patients repeated doses were needed because of the severity of envenomation.
Alpha-receptor stimulation by scorpion toxins plays a major role in pathophysiology, resulting in hypertension, tachycardia, myocardial dysfunction, pulmonary edema, and cool/vasoconstricted extremities.13,35 Prazosin, a competitive postsynaptic alpha-1, adrenergic receptor antagonist, should be the first line of management after antivenom therapy.35,36 Prazosin has demonstrated efficacy in treating both hypertension and hypotension following scorpion stings. In the hypertension stage it acts as an antihypertensive agent by reducing afterload. It has also been reported to reverse hemodynamic changes in tachycardic, hypotensive victims by acting as a vasodilator agent that corrects hemodynamic abnormality by reducing preload and afterload without triggering tachycardia. 37 Since the advent of prazosin the mortality rate of scorpion sting victims is less than 1%. 38 Bawaskar and Bawaskar 36 stated that morbidity and mortality due to scorpion envenoming depend upon the time lapse between the sting and administration of the postsynaptic alpha-1 blocker, prazosin hydrochloride.
There are limitations to our study. The most important is the fact that this was a retrospective chart review study, and, therefore, our data were limited to what was recorded on the patient records. The time interval between sting and arrival to first referring center was not recorded. The time interval before first antivenom injection was also unknown. For these reasons, we cannot clearly explain the difference in severity between victims coming from rural vs urban areas. It can, however, be hypothesized that poor management and transport facilities in rural areas might be responsible for more severe clinical presentations to referral hospitals.
In conclusion, we were unable to derive any findings based on demographic and epidemiological data to guide decision making regarding PICU admission for pediatric victims of scorpion sting in our area. The only significant difference, living in a rural area vs an urban area, is not likely to be useful in determining the need for PICU admission. Since patient care in PICUs is far more costly and manpower-intense than care provided in regular ward rooms, we propose that only children who develop systemic manifestations should be transferred to the PICU.