
Abstract
Objective
The purpose of this study was to examine the relationship between acute mountain sickness (AMS) and the fraction of exhaled nitric oxide (F
Methods
A total of 314 healthy young male recruits were voluntarily enrolled. Before ascent to an elevation of 4300 m, their F
Results
The AMS group had lower F
Conclusions
Basal F
Introduction
Acute mountain sickness (AMS) is a common illness affecting people entering high altitudes, causing adverse health effects that seriously affect physical performance. In the field of high altitude medical research, the prediction of AMS susceptibility in individuals going to high altitudes is still a thriving area of study. Researchers have been looking for the factors to predict AMS. So far, data from studies on the factors to predict AMS are inconsistent. Some studies have shown that poor hypoxic ventilatory response,1,2 age, 3 –5 and body mass index (BMI) 5 are associated with AMS development; however, other studies have indicated that these factors are not associated with AMS. 6 –10 Macinnis et al 11 reviewed the genetics of altitude illness in 2010 and reported that no reliable genetic factors to predict AMS have yet been identified. In addition, the methods for measuring some factors cannot be adopted for a large population, as these methods are not noninvasive, simple, quick, convenient, and relatively low-cost. Thus, we are searching for some simple, quick, convenient, and relatively low-cost methods to predict AMS risk.
The pathophysiological mechanisms of AMS development are still unclear; however, it is reported that vascular constriction during hypoxia, especially cerebrovascular and pulmonary vascular constriction, plays a role in AMS. 12 Nitric oxide (NO) is a gaseous signaling molecule with a large variety of physiological functions, including airway and vascular smooth muscle relaxation and the regulation of ventilation–perfusion matching. 13 Nitric oxide is produced endogenously within the upper and lower respiratory tract and can be measured in exhaled gas. 14 Studies have revealed that during hypoxic breathing, the exhaled NO from the respiratory tract of high altitude pulmonary edema (HAPE) –susceptible subjects was lower than that from the control subjects at both altitude and sea level and that a negative relationship existed between the exhaled NO and the pulmonary artery pressure. 15 Exhaled NO is associated with AMS susceptibility during exposure to normobaric hypoxia. 16 The defect in pulmonary endothelial cell and respiratory epithelial cell NO synthesis is one of the mechanisms contributing to exaggerated hypoxic pulmonary hypertension during short-term high altitude exposure. 17 These findings indicate that exhaled NO might be associated with AMS susceptibility during exposure to high altitude.
Smoking can cause hypoxia and is also associated with a decline in lung function. Some scholars have suggested that smoking is not significantly correlated with AMS, 3 ,10,18 but others believe that it may be a risk factor for AMS. 19 However, these conclusions cannot be effectively verified because of a lack of quantitative measurement of smoking behavior in these studies (the data were qualitative and collected by questionnaires) and an absence of effective measurement of the inhalation level, which is of great importance when evaluating exposure. Because of the great individual variations, the inhalation level may not be adequately evaluated by self-reported smoking behavior. The use of carbon monoxide (CO) monitors to quantify smoking has been reported, in which the level of exhaled CO has been widely used as an indication of smoking cessation.20,21 Carbon monoxide may also play an important role in the pathophysiology of airway diseases 22 and hemoglobin survival, which may be potentially related to AMS. 23 However, more precise monitoring is required to determine the relationship between the level of exhaled CO and AMS.
As gaseous signaling molecules,24,25 NO and CO have the characteristics of continuous production, rapid delivery, and rapid diffusion; thus, they can be detected by exhaled gas tests.14,26 In practice, measuring the fraction of exhaled NO and CO (F
Materials and Methods
Ethics Statement
This study was approved by the Ethical Review Board of the Third Military Medical University, Chongqing, China. There was no interaction between the study researchers and the individuals whose data were accessed. Personal information was removed from all data before retrieval and analysis.
Subjects and Settings
Recruits of a highland troop in West China were selected as the study population. They were receiving training at a military base at an altitude of 1350 m. A total of 391 healthy male servicemen were voluntarily enrolled. Before the questionnaire and physical examination, all recruits attended a meeting held at the base to clarify the purpose, method, and significance of the study. Individuals interested in participating in the study signed a consent form. The consent form required the participant's signature only and excluded other personal identifying information.
One investigator then performed an examination to obtain basic demographic data, ascent history, and drinking and smoking histories. Their health records were obtained from the troop's health service authority. An individual was excluded if any of the following was found: 1) previous ascent to an altitude >2900 m, 2) being born and raised in a region with an altitude >2500 m, 3) other acute diseases during the study period, including cold and diarrhea, 4) asthma or other pulmonary diseases, 5) any other severe chronic diseases, or 6) incomplete study information.
Variables of age and BMI (calculated as weight in kilograms divided by stature in meters squared) extracted from the health record were controlled. Drinking behaviors were surveyed by questionnaire and classified into 2 categories: 1 for current drinking and 0 for no current drinking. Smoking behaviors were also surveyed by questionnaire and classified into 2 categories: 1 for current smoking and 0 for no current smoking. If smoking currently, the subject needed to provide the duration of his smoking history and the amount of his weekly consumption. Vital capacity (VC) and forced vital capacity (FVC) were tested with a pulmonary function meter (AS-505, Minato Medical Science Corp, Osaka, Japan), according to the manufacturer's instructions. Smoking and drinking were also prohibited during the operation.
Fraction Exhaled Nitric Oxide and Carbon Monoxide Tests
The F
Tests for F
Acute Mountain Sickness Diagnosis
Subjects were divided into 3 groups. The groups were deployed to the destination at an altitude of 4300 m one after another by bus from the training base in April 2010. Each group traveled together with 2 observers on the 1080-km journey, in which the average altitude was 4254 ± 988.88 m (standard deviation), as shown in Figure 1. During the 4-day journey, they traveled during the day and rested for 1 night at each army service station.
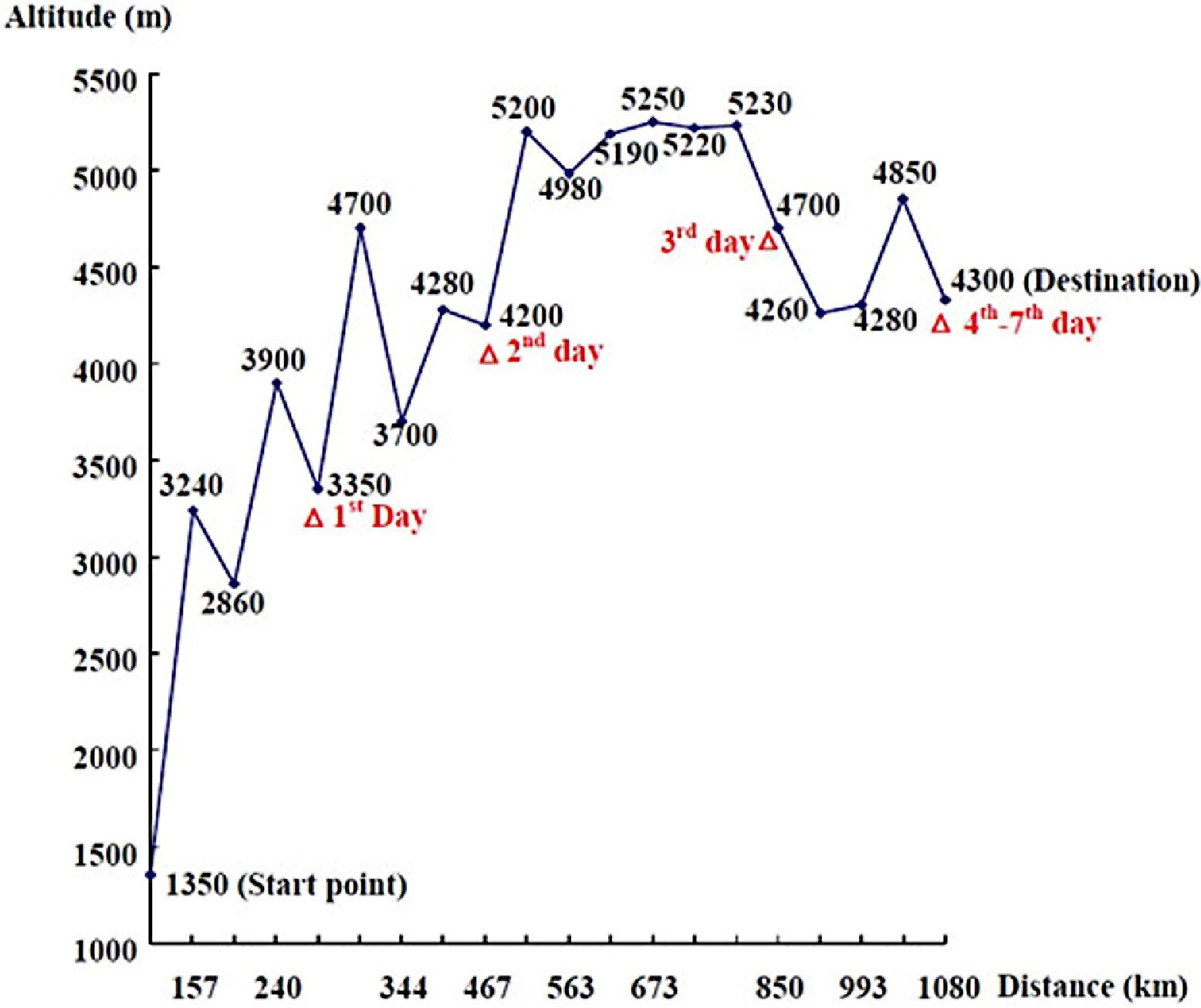
Changes in altitude and distance during the journey (Δ indicates the sleeping altitude each day).
The AMS diagnoses were based on the Lake Louise score (LLS), an international standard scoring system for AMS.
28
Before ascending, all investigators and subjects had become familiar with the LLS. The symptom investigations were performed every day after arrival at each army service station at 9
Statistical Analysis
The data were analyzed using SPSS 13.0 software (Chicago, IL) and a probability value of less than .05 was considered statistically significant in all analyses. Before analyses, all data were reviewed by the principal investigator for completeness.
We first performed descriptive statistics: 1) the LLSs were classified into 3 groups (0 point, 1–4 points, and 5 or more points), and the number of each category and percentage on each day were computed; 2) the number and percentage of smoking and drinking behaviors in AMS diagnosis categories were computed; 3) the mean and standard deviation of each continuous variable (ie, age, BMI, VC, FVC, F
A Student's t test was performed to determine the mean difference in each continuous variable between the AMS and non-AMS groups, and a χ2 test was performed to determine drinking and smoking behavior differences between these 2 groups. Pearson's correlation test for continuous variables and Spearman's correlation test for categorical variables were used to evaluate relationships between age, BMI, VC, FVC, smoking, drinking, F
Next, to test the relationship between the AMS score and F
Finally, a logistic regression was used to test the predictive values of F
Results
After filtering, 314 healthy servicemen remained in our study (mean age ± SD, 20.18, ± 1.73 years; mean stature ± SD, 171.74, ± 6.49 cm; mean weight ± SD, 63.27, ± 7.10 kg).
The total distance of the journey was 1080 km, in which the highest altitude encountered was 5250 m and the highest sleeping altitude was 4700 m (day 3; Figure 1). The data indicated that AMS developed and increased when the subjects entered the highland. The peak appeared on day 3, after which the incidence decreased. On day 7, AMS was nearly absent in the population. There was no case of HAPE or high altitude cerebral edema.
Both the highest LLS and the largest number of individuals with an LLS > 4 appeared on day 3, when the average LLS was 3.87 ± 3.37 and 119 individuals had an LLS > 4 (37.9%; Table 1). According to our criteria, 119 (37.9%) of the 314 subjects (equal to the total number of subjects having an LLS > 4 on day 3) investigated on the total journey were diagnosed with AMS, with the highest LLS reported as 21.
The number (percentage) of subjects in different Lake Louise Score categories on each day and the mean Lake Louise Score on each day (n = 314) a
LLS, Lake Louise Score.
Some subjects missed the investigation during the follow-up: 7 missed on day 4; 17 missed on day 5; 31 missed on day 6; and 44 missed on day 7.
Maximal LLS during the 7-day investigation.
The mean and standard deviation of each continuous variable in the AMS and non-AMS groups are shown in Table 2. Age, BMI, and FVC did not differ between the groups. However, F
Mean and SD of each continuous factor in acute mountain sickness and non–acute mountain sickness groups
AMS, acute mountain sickness; BMI, body mass index; F
Student's t test for each factor.
Drinking and smoking behaviors in acute mountain sickness and non–acute mountain sickness groups
AMS, acute mountain sickness.
χ2 test for each factor.
Factors affecting fractions of exhaled nitric oxide and carbon monoxide in smoking and nonsmoking groups
F
Student's t test for each factor.
The correlation coefficients between LLS (daily LLS and max-LLS) and the other variables and those among the other variables were analyzed. Negative correlations with max-LLS and most-day LLSs were observed for VC, FVC, F
The separated linear regressions showed that both F
In the separated and integrated logistic regression models, F
Separated and integrated logistic regression models to test the predictive value of fractions of exhaled nitric oxide and carbon monoxide, adjusted for age, body mass index, vital capacity, and drinking behavior (n = 314)
F
Values for F
Hosmer-Lemeshow test.
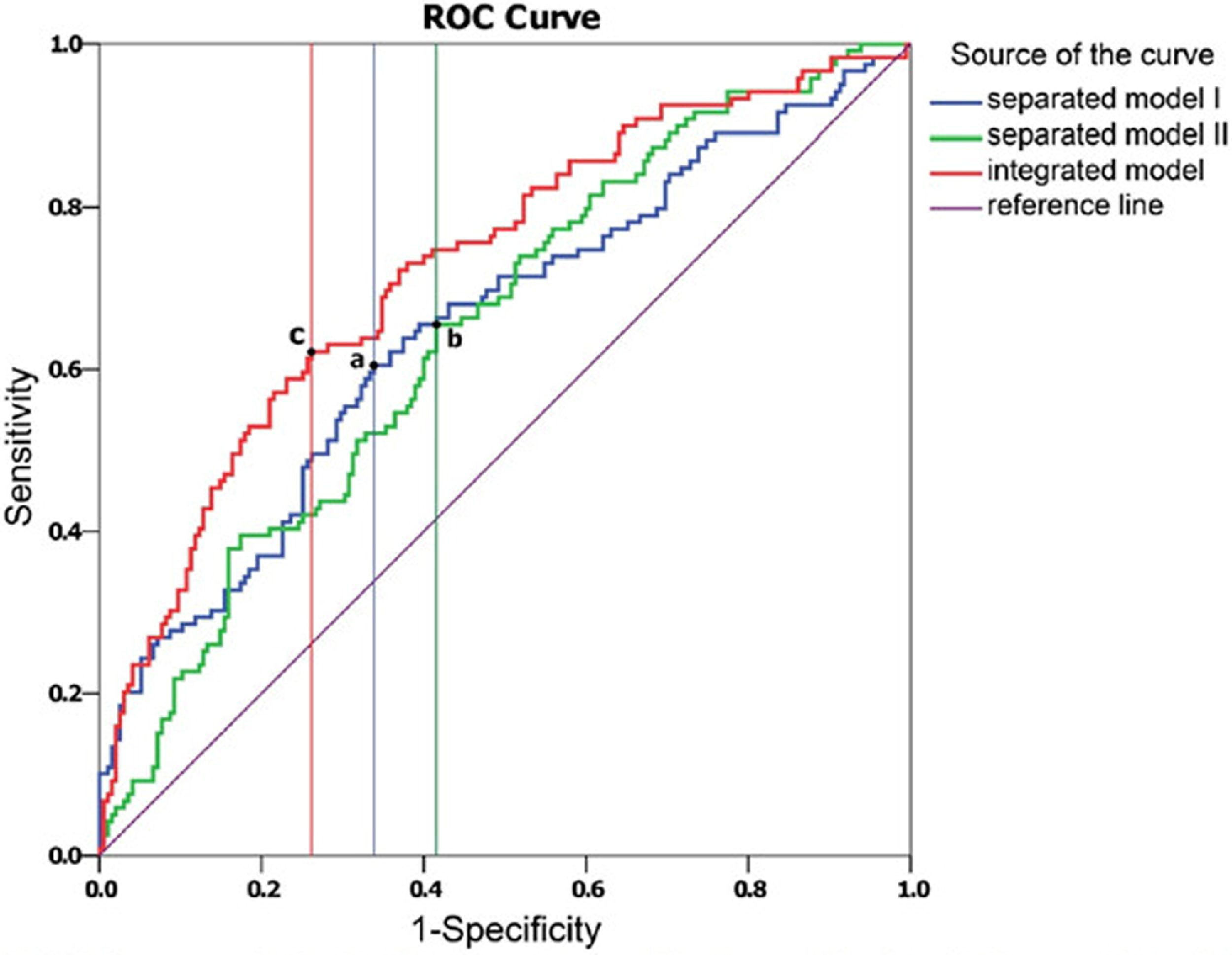
Receiver operating characteristic curves of the logistic regression models (a: cutoff value = 0.374, sensitivity = 60.5%, specificity = 66.2%; b: cutoff value = 0.370, sensitivity = 65.6%, specificity = 58.5%; c: cutoff value = 0.406, sensitivity = 62.2%, specificity = 73.9%). Separated model I (blue line): the logistic regression models to test the predictive value of the fraction of exhaled nitric oxide; separated model II (green line): the logistic regression models to test the predictive value of the fraction of exhaled carbon monoxide; integrated model (red line): the logistic regression models to test the predictive value of the fractions of exhaled nitric oxide and carbon monoxide).
Receiver operating characteristic curve analyses for logistic regression models
AUC, area under the curve; NPV, negative predictive value; PPV, positive predictive value; ROC, receiver operating characteristic.
ROC curve of separated models I.
ROC curve of separated models II.
Discussion
The results of the statistical analysis suggest that higher F
Pulmonary NO may play an important role in the physiological response to acute high altitude hypoxia.
12
Some studies have demonstrated the importance of pulmonary vascular endothelial and alveolar epithelial NO synthesis in the regulation of pulmonary vascular responsiveness to high altitude exposure,
32
and that a lower F
The latest F
Measured F
The results indicate that smoking behavior at low elevations significantly decreases the risk of AMS when one travels to a high altitude. However, this does not mean that smoking is entirely beneficial for decreasing AMS. Some studies have shown that smokers exhale significantly less NO than do healthy volunteers.36,37 In our study, the F
The results of the logistic regression analysis further validate the relationship between AMS and F
The results showed the 95% CI for the mean F
This study is, to our knowledge, the first to focus on the relationship between AMS and exhaled gases (F
Limitations
Several limitations exist in the study design and should be considered when generalizing our findings to other populations or conditions. First, in this study, occupation, diet, and physical load at a high altitude were negligible because everyone experienced the same condition. Therefore, the identifiable risk factors for AMS among such a specialized population are limited. Second, the Operating Manual of the Micro+ Smokerlyzer monitor points out that subjects with F
Conclusions
In conclusion, the concentrations of F
Footnotes
Funding
This study was supported by 973 project of China (2012CB518201). This work was supported by a research grant from the Chinese National Science Support Project (2009BAI85B01).
Acknowledgments
We are grateful to the medical department of the highland military units and their staff for providing great assistance in this study. We also thank the volunteers for participating in this study. We would like to thank Miss Xie-Wan Chen and Ms Xiao-Qing Zhan for a critical reading of the manuscript and kindly giving precious advice.
Disclaimer: There are no conflicts of interest to disclose.
⁎
These authors contributed equally to this work.