
Abstract
Objective
In austere environments, patient management decisions are often limited by obtainable resources. Portable ultrasound may allow for the detection of fractures when imaging modalities such as radiography are unavailable. We used a simulation training model in a pilot study to examine the ability of emergency medical technicians (EMTs) to detect the presence or absence of a variety of simulated fracture patterns with portable ultrasound.
Methods
The fracture simulation model is composed of a mechanically fractured bare turkey leg bone housed in a shallow container within a completely opaque gelatin solution. Five different fracture patterns were created. Twenty EMTs sonographically evaluated these models with a portable ultrasound device to determine the presence or absence of a fracture.
Results
EMTs correctly identified the presence or absence of a fracture in the no fracture, transverse fracture, and oblique fracture models 95% of the time. They always correctly identified the presence of a fractured model when assessing the comminuted and segmental fracture models. Across all fracture patterns, a final detection sensitivity of 97.5% (95% confidence interval [CI]: 94.1%–100.0%) and a specificity of 95.0% (95% CI: 85.4%–100.0%) were observed.
Conclusions
Using portable ultrasound, EMTs correctly detected the presence or absence of simulated long bone fractures with a high degree of sensitivity and specificity. Future studies may evaluate the ability of other groups to use ultrasound to assist in the diagnosis of fractures and examine the clinical impact of this skill in environments where conventional imaging modalities are limited or unavailable.
Introduction
In the wilderness and other austere environments, decisions regarding patient management are often limited by obtainable resources. Diagnostic tools and tests such as plain radiography, computed tomography, and blood analysis often require equipment that is too large or impractical for use in remote or out-of-hospital locations. Consequently, the decision to evacuate or the ability to appropriately treat patients may be jeopardized. Fracture detection has traditionally required large devices, but portable ultrasound may allow for the detection of fractures in areas where other imaging modalities such as radiography are not readily available.
Evaluation by ultrasound for fracture detection has the advantage of immediate clinical correlation and can be made by people with minimal training in the use of ultrasound.1,2 We recently described a novel trainer for the ultrasound identification of long bone fractures that has been evaluated by physicians familiar with the dynamic use of ultrasound.3,4 Using this simulation training model, we sought to study the ability of emergency medical technicians (EMTs) to detect the presence or absence of a variety of simulated fracture patterns using a portable ultrasound device.
Methods
Simulation Model
The simulation model is composed of a bare turkey leg bone that is mechanically fractured and housed in a shallow plastic container within a firm gelatin matrix. The diaphysis of the bone is approximately 15 cm long with a diameter of 1.5 cm. A training model containing a single transverse fracture and 5 study models were created with different fracture patterns: no fracture, transverse fracture, segmental fracture, oblique fracture, and comminuted fracture. The training model was semi-opaque to allow visualization of the underlying bone, while the study models were completely opaque (Figure 1). Approximately 3 mm to 5 mm of bony cortex displacement was present at each fracture site.
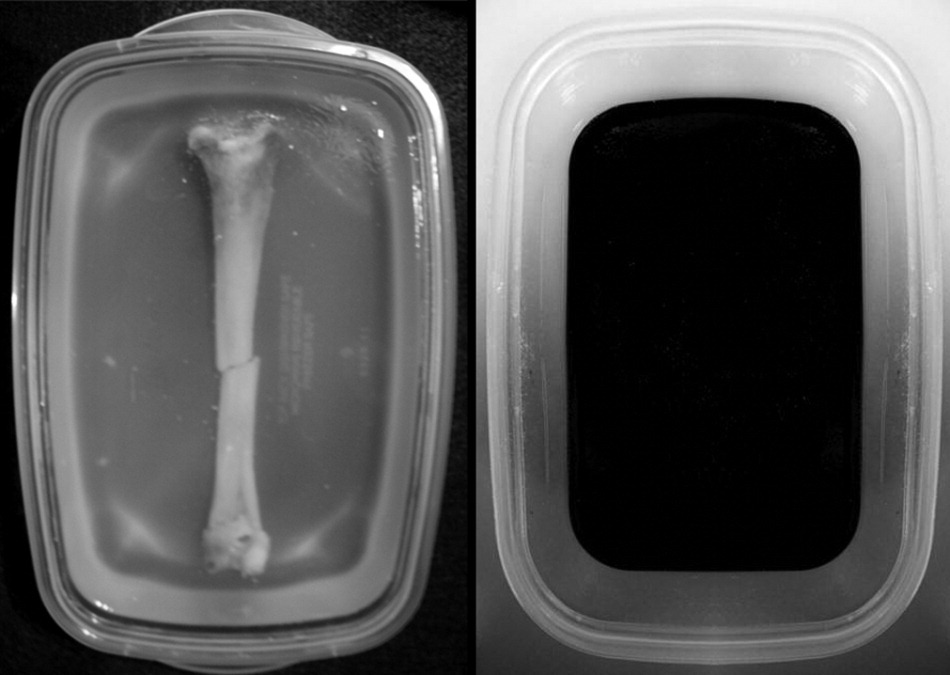
The semi-opaque training model (
Model Evaluation
The study was granted exemption from continuing review by our study site institutional review board and the requirement for written informed consent was waived by the review committee. A convenience sample of 20 EMTs were consecutively enrolled in the emergency department at Madigan Army Medical Center at Fort Lewis, WA. None of the EMT participants reported previous familiarity with the practical use of ultrasound. Participants received a 2-minute standardized orientation and training session ensuring familiarization with examination of the semi-opaque fracture model (Figure 1). They then sonographically evaluated the 5 completely opaque models with a SonoSite M-Turbo portable ultrasound device (Sonosite Inc, Bothell, WA) equipped with a 10-5 MHz transducer head. They were blinded to the true identity of the underlying fracture pattern. Participants were presented the study models in an identical order and were allowed an unlimited amount of time to complete their sonographic assessment. Their ultrasound impressions of the presence of a bony fracture were then recorded for each model.
Statistics
Data were described as proportions of models correctly identified as fractured or not fractured. An overall sensitivity and specificity for correct identification of fracture presence was calculated with 95% confidence intervals (CIs) via a 2 x 2 contingency table analysis.
Results
The 20 EMTs participating in this study were representative of all 3 primary levels of certification in Washington State (EMT Basic, EMT Intermediate, and EMT Paramedic). They correctly identified the presence or absence of a fracture in the models with no fracture, a transverse fracture, and an oblique fracture 95% of the time. Participants always correctly identified the presence of a fractured model when assessing the comminuted and segmental fracture models. All identification errors were made by different EMTs with no EMT committing more than 1 incorrect ultrasound assessment among the fracture models. Across detection of all fracture patterns, a final sensitivity of 97.5% (95% CI: 94.1%–100.0%) and a specificity of 95.0% (95% CI: 85.4%–100.0%) were observed in our study (Table). Sonographic assessment of all 5 opaque study models was generally completed in approximately 5 minutes.
The correct identification of the presence or absence of a fractured model based on sonographic examination by 20 EMT participants ⁎
Overall sensitivity = 97.5% (95% CI: 94.1%–100%). Overall specificity = 95.0% (95% CI: 85.4%–100%).
Discussion
Austere environments often present significant diagnostic and therapeutic challenges to those providing medical care. Ultrasound is frequently used in the bedside evaluation of the trauma patient, as a tool in vascular access procedures, and to assist in abscess identification and management. 5 Portable ultrasound is a versatile tool that has been shown to alter the disposition and treatment of patients in remote environments. 6 It is well suited for use in settings where traditional radiography may not be immediately available such as in rural areas, military and humanitarian medicine applications, and in the prehospital setting.
Recently, ultrasound has emerged as a useful tool for both fracture identification and similar applications such as the dynamic visualization of fracture reduction.5,7 Bone is not penetrated by ultrasound, and cortical discontinuities greater than 1 mm may herald the presence of a fracture (Figure 2). 5 Not surprisingly, the ability to use ultrasound to identify fractures increases with time and practice. Medical simulation models such as the one used here allow such training without placing patients at risk for discomfort or harm, as well as providing known pathology. While a modest amount of research exists demonstrating the ability of prehospital providers to use ultrasound, there appears to be a lack of studies examining their ability to use this tool to detect fractures. 8
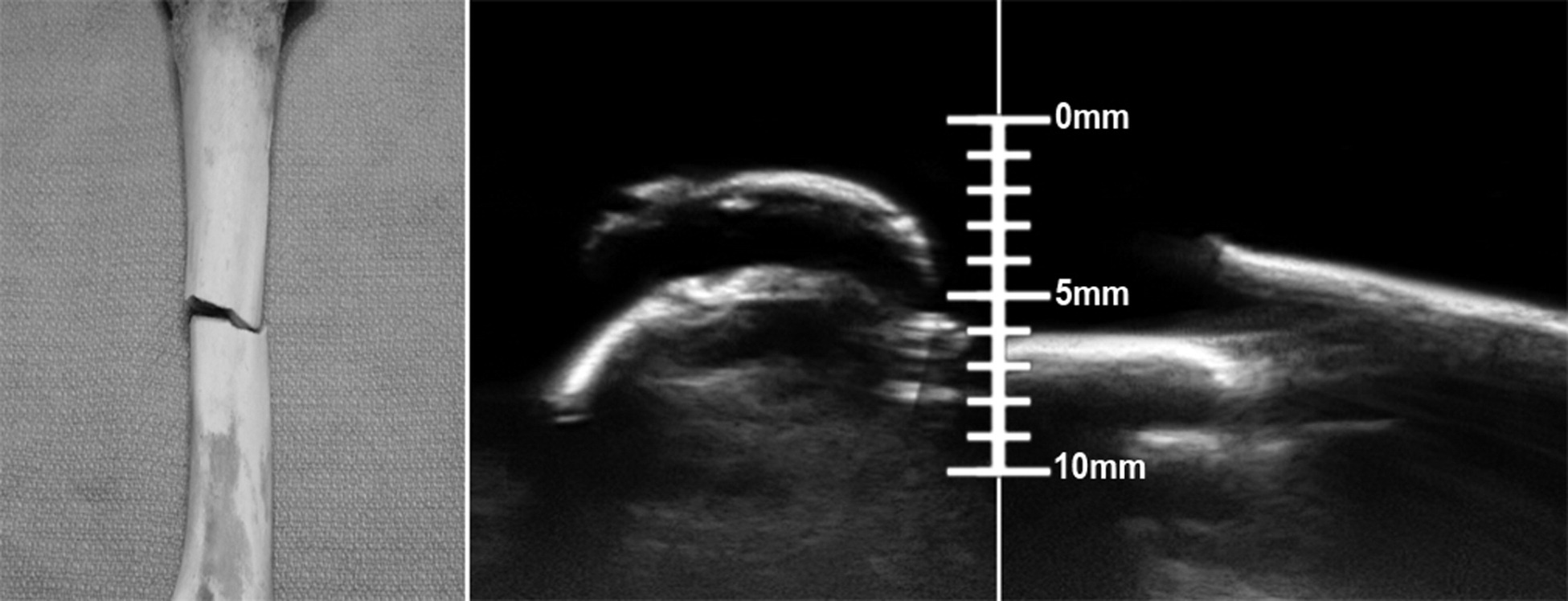
Close-up image of a transversely fractured bone prior to placement in the opaque gelatin (
Our EMT study population regularly practices beyond the physical walls of the hospital with portable and practical tools and was minimally trained in the use of ultrasound. The ultrasound used in this study is the size of a laptop computer, but other models exist that are commonly used in out-of-hospital environments. Our results may be limited by applicability only to this particular portable ultrasound device. While this model has been previously evaluated as a useful training tool, the degree that these skills are transferable to living patients is uncertain. Portable ultrasound may have potential as a useful tool, but its cost could be prohibitive to some. According to SonoSite, their product line ranges in price from around $25,000 to $60,000 (D. McGaskey, written communication, December 2009). In certain austere environments such an investment may be impractical, particularly when the overall impact of portable ultrasound in changing the management of a person with an extremity injury remains uncertain.
Some limitations specific to our study should be noted. While ultrasound can detect subtle cortical irregularities suggestive of a fracture, we chose to create displacement of 3 mm to 5 mm at the fracture site. Fracture detection rates with less displacement may be lower than observed in our study. Also, participants trained on a semi-opaque model with a transverse fracture to learn the ability to identify normal and abnormal cortical appearance by ultrasound. However, the fractured models contained other fracture types that appear somewhat different on ultrasound. Although all fracture types consistently disrupt the cortical surface, semi-opaque model training that included all fracture types might have altered the final detection rates. While we presented participants with the models in the same order, an order effect may have existed in our study for which we did not control. It should also be noted that our study model population contained a high percentage of fractured models, with only 1 of the 5 models being free of a fracture. The overall ability to correctly identify a fractured model may not be similar in model populations consisting of more or less abnormal models.
As a diagnostic tool, portable ultrasound appears to be well suited for use in austere environments and also for the detection of long bone fractures. In our pilot study, EMTs without familiarity in other applications of ultrasound were able to identify the presence or absence of a fracture with a high degree of sensitivity and specificity in all of the models presented to them. Further studies are needed to examine the potential clinical impact of this skill in environments where conventional imaging modalities are limited or unavailable.
Footnotes
The abstract accompanying this work was presented at the Wilderness Medical Society: 2009 Wilderness Medicine Conference and Annual Meeting, July 29, 2009, Snowmass, CO.
The authors have no conflicts of interest or financial relationships with SonoSite to disclose. The views expressed herein are solely those of the authors and do not represent the official views of the Department of Defense or Army Medical Department.