
Abstract
Objective
The purpose of this study was to identify the differences between the educational curricula, skill sets, and funds of knowledge required for certification as an Outdoor Emergency Care Technician (OEC-T), Emergency Medical Technician (EMT), and Emergency Medical Responder (EMR).
Methods
We directly and in detail compared topics and skills presented in the OEC-T curriculum with those presented in the EMT and EMR education and training curricula.
Results
The information and skills taught in the OEC-T curriculum are in general more extensive than those taught in EMR training but are not equivalent to EMT. The OEC-T program has more depth in environmental medical issues, such as altitude illness, hyperthermia and hypothermia. Completion of the EMR program is 112 hours shorter and constitutes 30% of the duration of the EMT program. Completion of the OEC-T program (for certification only and not including additional “on-hill” patroller training) is 80 hours shorter and is half the duration of the EMT program.
Conclusions
The OEC-T curriculum includes a skill set and fund of knowledge that exceeds those of the EMR program, but does not include all the knowledge needed for an EMT program. The OEC-T program prepares out-of-hospital providers to care for patients in the wilderness, with special emphasis on snowsports pathology. The EMT program places a greater emphasis on medical disease and emergency medication administration. These differences should be considered when determining staffing requirements for agencies caring for patients with snowsports pathology.
Keywords
Introduction
Ski patrols are paid or volunteer organizations working for ski area management or the US Forest Service, most often using the National Ski Patrol (NSP) curriculum to provide medical and transportation training for injured snowsports participants. 1 More than 95% of ski areas consider the NSP's Outdoor Emergency Care (OEC) program to be the standard for training ski patrollers. 1 Out-of-hospital (OOH) providers who successfully complete the OEC course are known as OEC-Technicians (OEC-T). Outside of the ski area environment, most OOH care in the United States is provided by the Emergency Medical Services (EMS) system, largely composed of emergency medical responders (EMR) (formerly known as first responders), emergency medical technicians (EMT) (formerly known as emergency medical technician–basic), and paramedics. 2
Each category of OOH emergency care provider is educated within unique training standards. This state of affairs has engendered some confusion about the specifics of education and skills. To understand the qualifications of individual providers, and to contribute to the discussions regarding 1) to what degree OEC-T training offered by the NSP is equivalent to EMR or EMT training, and 2) whether all ski patrollers should be trained at the EMT level, we decided that a logical first step is side-by-side comparison of programs. Therefore, we compared directly the differences among the OEC-T, EMT, and EMR educational curricula, skill sets, and funds of knowledge based on the fifth edition of
Methods
We used the fifth edition of
Results
Course duration varies among these programs, with the shortest being EMR, followed by OEC-T and EMT, respectively (Tables 1, 2, and 3). Completion of the EMR program is 112 hours shorter and constitutes 30% of the duration of the 160-hour EMT program (Table 1). Completion of the OEC-T program (for certification only and not including additional “on hill” patroller training) is 80 hours shorter and constitutes 50% of the duration of the EMT program. The OEC-T program is listed as “80+ hours,” indicating that OEC-T instructors incorporate additional “on the hill” practical field sessions (usually 40+ hours) to meet the educational needs for a person to become a ski patroller. To obtain an OEC-T certification and not become a ski patroller, a person must meet a minimum of 80 educational hours, as advised by the NSP National Medical Committee. The EMR program does not include a field-training component. Only the EMT program has a required clinical component, which typically occurs in a local emergency department (Table 1). The EMT curriculum provides the most comprehensive explanations, and greater hands-on training in certain topics (Tables 3 and 4).
Comparison of material contained in emergency medical technician and outdoor emergency care technician programs
OEC-T, outdoor emergency care technician; EMT, emergency medical technician.
We used the same method of comparison as described in the National Emergency Medical Services Educational Standards where “depth” refers to the level of detail and “breadth” refers to the amount of material taught in a course. 5 Depth is further separated into simple, fundamental, and complex levels of understanding. Breadth is further separated into simple, foundational, and comprehensive levels of understanding. 5 Both complex depth and comprehensive breadth levels of understanding (according to the National Emergency Medical Services Educational Standards) are used only in reference to the paramedic curriculum and are not used in our comparison. The differences between the OEC-T and EMT curricula are highlighted in Table 4 and visually presented in a Venn diagram (Figure).
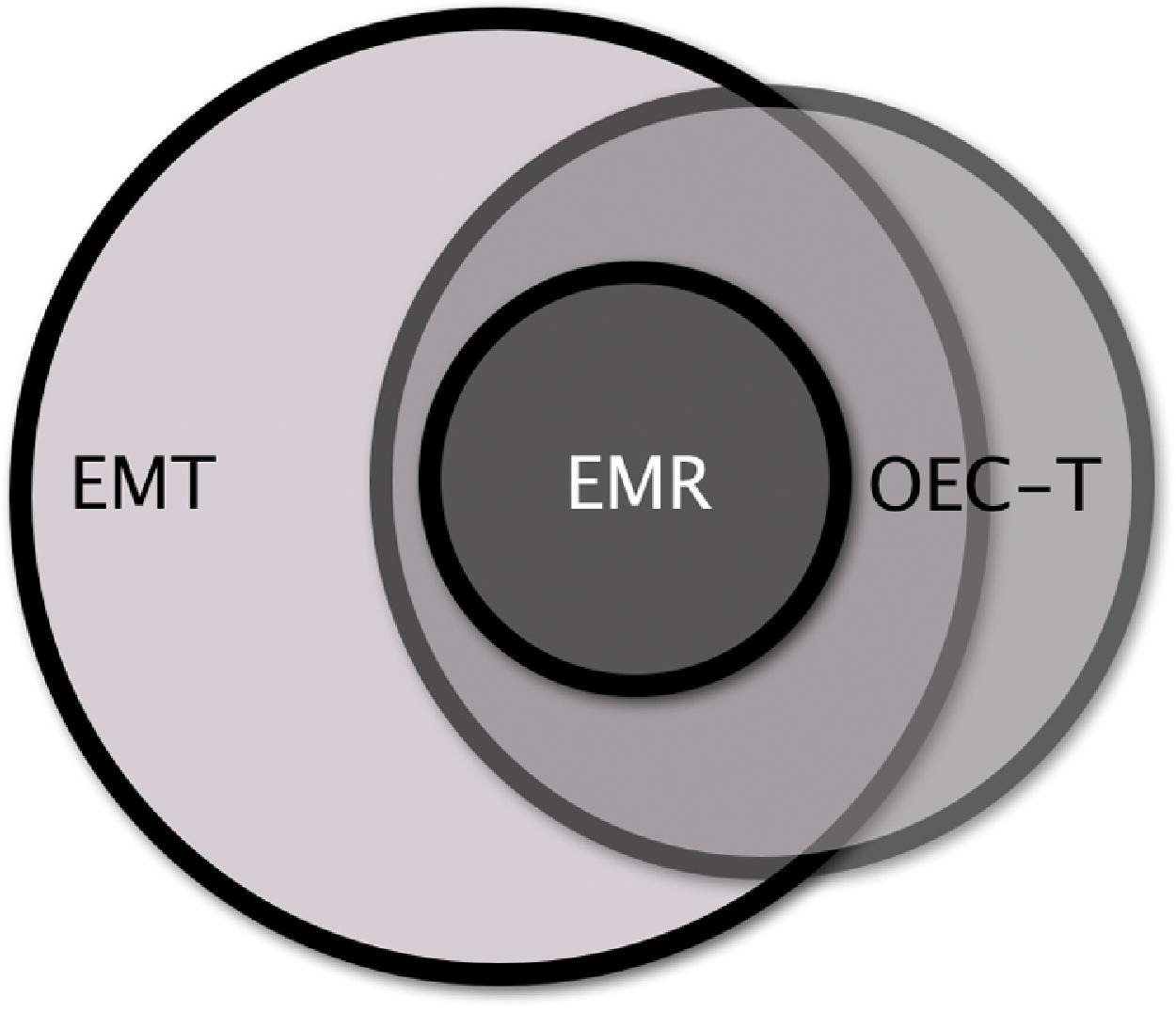
Visual representation comparing the programs: emergency medical responder (EMR), emergency medical technician (EMT), and outdoor emergency care technician (OEC-T).
Discussion
Our comparison of the OEC-T, EMR and EMT programs demonstrate that the EMR program is significantly shorter in duration, provides a more simple level of understanding, and teaches fewer psychomotor skills than the OEC-T and EMT programs. Therefore, the EMR level of training may not be appropriate for ski patrollers with first responder (and sometimes beyond) responsibilities for patients with medical conditions and injuries managed in isolated regions in the absence of higher level OOH providers. The OEC-T curriculum includes all of the NHTSA EMR requirements, but not all of the NHTSA EMT requirements.
The EMT curriculum is twice the duration in hours of the OEC-T curriculum. It places greater emphasis on ambulance operations and pathophysiology of medical diseases, and has more depth when teaching skills in patient monitoring and emergency medication administration. The OEC-T program places greater emphasis on wilderness operations, backcountry extrication considerations, adaptation and improvisation, environmental injuries, and first aid specific to snowsports pathology. To achieve precise equivalency of the 2 programs, should such be desired, would be a function of adding to either program the missing elements from the other program.
Ski patrollers are educated and trained to assist persons in distress at downhill and backcountry ski areas. Established in 1938, the NSP is dedicated to serving the public and outdoor recreation industry by providing OOH provider education. The organization has more than 26,000 members serving more than 600 patrols. The NSP provides OEC-T education, leadership training, safety programs, and transportation services, but is not a licensing agency. 6 The NSP's National Medical Committee must approve the OEC-T course, originally titled Winter Emergency Care (WEC). This training program continues to be the most accepted program for ski patrollers, with more than 95% of all US ski areas designating OEC-T certification as an entry requirement for their ski patrollers.
Not all ski patrols (mostly “professional” or “pro” patrols) use OEC-T education. A small number require or accept EMT certification, rather than OEC-T plus on-hill training, and are not affiliated with the NSP. Also some patrols honor the OEC-T card for acceptance on a patrol, but are not members of the NSP.
Healthcare professionals with current MD, DO, PA, NP, RN, LPN, paramedic, or EMT licensure may complete an abbreviated version of the OEC-T course, known as the Challenge Course, that focuses on providing OEC-T-specific knowledge and skills that may not have been learned during prior training. 7 On successful completion of the Challenge Course, these persons are granted an OEC-T card identical to that obtained by graduates of the standard OEC-T course.
Outside of the ski area environment, EMS provides the majority of OOH emergency care. The NHTSA has been charged with establishing educational goals and standards for the various levels of EMS providers. These levels are EMR, EMT, advanced emergency medical technician (AEMT), and paramedic. Completed in 2009, the National EMS Education Standards constitute realization of the 1996 vision for updating and advancing education standards in OOH care. The revised system is composed of core competencies for each level of EMS provider, with corresponding scope of practice models. These education standards replace the Department of Transportation (DOT) National Standard Curricula (NSC) developed in the mid 1990s. 2 ,4,8,9
Not included for comparison in our evaluation are courses offered by organizations such as Wilderness Medical Associates (WMA) and the National Outdoor Leadership School–Wilderness Medicine Institute (NOLS-WMI). These courses include wilderness first responder (WFR) and wilderness emergency medical technician (EMT-W) courses based on the prior NHTSA EMR curriculum and EMT National Standard curriculum. Graduates of these programs are eligible to take the National Registry of Emergency Medical Technician (NREMT) examination and apply for state certification or licensure. Wilderness education incorporated into these courses may count (depending on the state) as continuing education credit toward national or local recertification as an EMR, EMT, or paramedic. It should be noted that, similar to some knowledge and skills taught in the OEC-T course, the additional wilderness knowledge and skills not contained in the NHTSA core curriculum are usually not recognized by county EMS systems and state licensing boards.
An OEC-T is granted certification from the National Ski Patrol and is commonly under the direction of a physician medical advisor, with local ski area management advising the patrol on nonmedical issues. The EMR and EMT providers are either certified or licensed by state authorities and typically operate under the direction of a county physician medical director.
The OEC-T scope of care may vary between ski areas as determined by physician medical director preferences and individual ski area policies because of different needs at individual ski areas, as some have medical clinics at the base whereas others are located far from any advanced medical care. As members of a county or state EMS system, EMTs follow policies set by the system medical director. A ski patrol's policies and procedures may not necessarily be identical to those of the EMS district in which they are located. That could lead to confusion or possibly conflict during patient transfers and mutual aid responses. However, the NSP encourages local ski patrols to interface with their local EMS system so that conflicts are minimized. The OEC-T has a national standard of training allowing portability of the credential from state to state, whereas EMR and EMT training and credentialing currently vary from state to state. The EMR and EMT training will become more standardized, however, if more states change to the new national educational standards used for comparison in this study.
Study Limitations
We used recently published materials to provide the most up-to-date information. A limitation of our analysis may be that the EMR and EMT curricula are not currently in use across the entire country or may not accurately reflect the current status of EMR and EMT educational standards. Because the most recent edition of OEC-T was recently published, we may have overestimated or underestimated the duration of medical training for the OEC-T course.
Conclusions
We show in this study that the EMT and OEC-T programs are not the same. We have enumerated the specifics of these programs in a side-by-side comparison. Although significant overlap exists between these programs, wilderness and ski resort providers and agencies need to take the differences into consideration when deciding on training curricula and staffing. Based on the curriculum, it is our impression that the OEC-T program adequately trains responders to initially manage snowsports pathology. We recommend that agencies anticipating significant non-snowsports medical pathology or prolonged evacuation times to definitive care consider augmenting the OEC-T training program or adding EMT providers. These providers could provide more advanced care for these situations. Also EMTs should consider augmenting their wilderness or snowsports medical training before caring for snowsports patients.
Footnotes
Acknowledgment
We would like to disclose that coauthor David H. Johe, MD, is Medical Editor of