
Abstract
Purpose:
Length stable diaphyseal femur and tibial shaft fractures in paediatric patients may be fixed with flexible intramedullary nails (FINs) in selected paediatric patients. Previous studies based on biomechanical models have suggested that the forces of gait may overcome the stability of this construct in patients weighing more than 45 kg. Surgeons occasionally use FINs for fixation in patients outside this limit. The purpose of this study was to evaluate whether FINs could be used in paediatric patients weighing over 45 kg without increasing the rate of complications.
Methods:
A retrospective cohort review was performed for 12 patients weighing over 45 kg with femoral or tibial fractures treated with FINs, matched 1:2 for gender and bone type with 24 patients weighing less than 45 kg; also with femoral or tibial fractures treated with FINs over the same period.
Results:
There was no significant differences in rate of major complication or increases in angulation between the study and control group. The study group had major complication (8.3%) of hypertrophic nonunion in the tibia, and the control group had one major complication (4.2%) of increased anterior bowing in the femur. The odds ratio of developing a major complication in the study group was 2:1 which was not significant (p = 0.06).
Conclusions:
FINs can be considered as a treatment option for fixation of femoral and tibial fractures in a select group of paediatric patients weighing more than 45 kg. Clinical and functional outcomes measurements in larger sample sizes are needed before making any definitive conclusions.
Introduction
Fractures of the femur and tibia are the second and third most commonly observed long bone fractures in the paediatric population. 1 These are often associated with high energy trauma which may lead to additional complications. 2 In some cases, these fractures can be managed in a conservative fashion, but surgical correction is indicated when additional factors such as open fractures, multitrauma damage or simultaneous head injury are involved. 2 As of late, the focus of treatment has shifted more towards operative fixation because of advancements in minimally invasive surgical techniques that minimise soft-tissue trauma and the recognition of rapid healing and remodelling in paediatric fractures making them amenable to minimally invasive internal fixation techniques. 3 Many surgical options are available including flexible intramedullary nail (FIN), reamed intramedullary nailing, plating, external fixation and prolonged traction. However, the use of flexible nails, which have gained popularity in length-stable fractures, can offer a less technically demanding and faster procedure at a lower cost. 4
The use of FINs is theoretically limited by the weight of the patient because the construct can be overwhelmed by the forces of gait. 5 A biomechanical study by Li et al 6 evaluated the bending moments in paediatric-sized femur models with simulated transverse midshaft fracture patterns that were stabilised with titanium intramedullary nails. They then correlated results with in vivo gait data and suggested that a maximum weight of 40 to 45 kg should be utilised as a cutoff for utilising this fixation modality. These findings were later corroborated by Deakin et al 5 who retrospectively evaluated 35 adolescent patients over 11 years of age who had fractures (21 tibias and 15 femurs) that were managed with FINs. They found malunion rates of 60% and 38% for femoral and tibial shaft fractures, respectively (n = 9 of 15 and 8 of 21) and found patients who developed complications to be significantly heavier (56 kg vs. 45 kg, respectively). 7
Although the theoretical cutoff of 45 kg exists, because of the growing epidemic of obesity in the paediatric population in the United States, 8 surgeons occasionally use this type of fixation in a selected group of patients over this weight threshold. Therefore, the purpose of this study is to evaluate if the use of flexible intramedullary nails in paediatric patients who are heavier than 45 kg is possible without increasing complications. More specifically, we focused on (1) determining the odds of developing a complication or nonunion and (2) whether there is a greater increase in angulation in patients undergoing FIN when stratifying by weight greater or less than 45 kg.
Methods
After obtaining proper Institutional Review Board approval, a multiinstitutional retrospective review of prospectively collected data was conducted to evaluate a consecutive series of all tibia and femur fractures admitted to our institution from January 2005 to December 2015 in patients younger than 18 years, which resulted in 1067 records. From this database, we evaluated all patients treated with flexible intramedullary nail (without end caps) that were heavier than 45 kg. All tibia and femur fractures were treated with two (2) flexible intramedullary nails. We then excluded patients who were skeletally mature, all pathologic fractures and all patients who had less than 12 months of follow-up. A cohort of 12 patients who were treated with either titanium or stainless steel flexible intramedullary nails was included (Table 1). All identified patients were placed in a long-leg cast postoperatively and made non–weight-bearing. This group was later defined as our study cohort.
Details of patients weighing over 45 kg undergoing flexible intramedullary nailing.
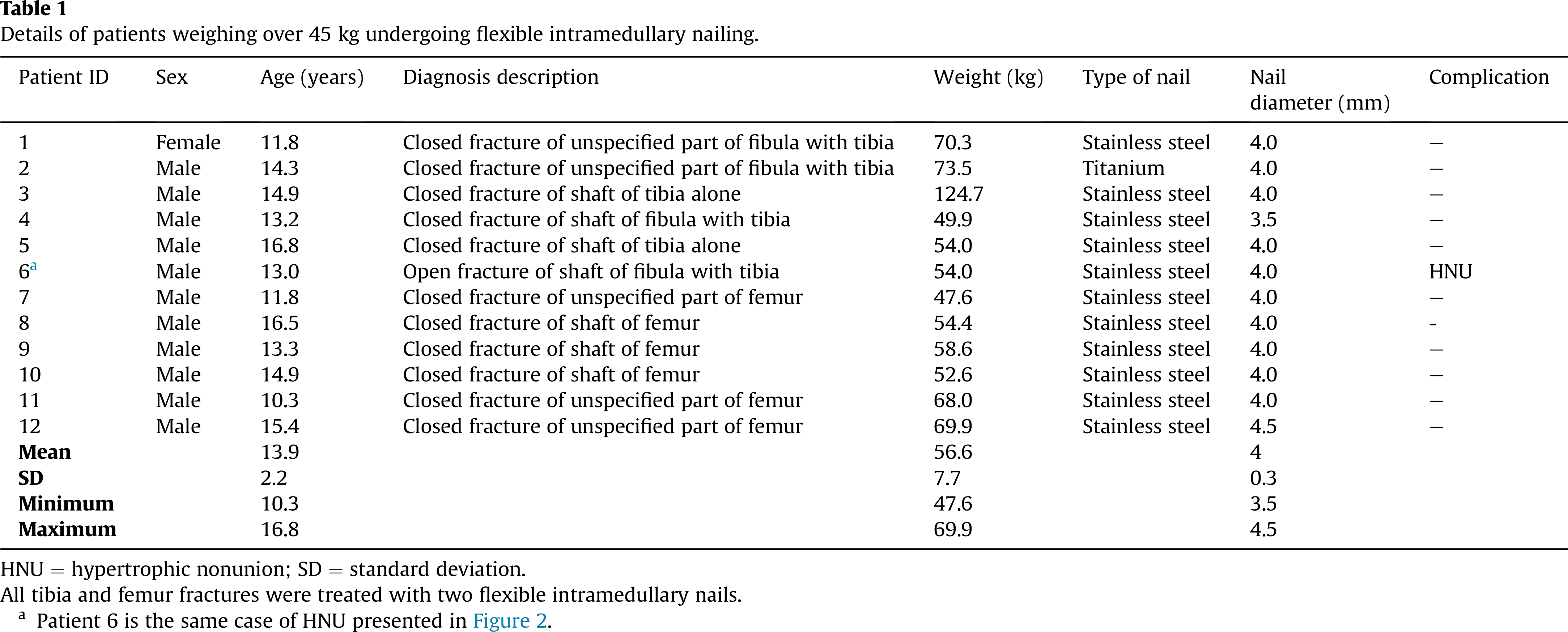
HNU = hypertrophic nonunion; SD = standard deviation.
All tibia and femur fractures were treated with two flexible intramedullary nails.
a Patient 6 is the same case of HNU presented in Figure 2.
This cohort was then 1:2 matched by gender and bone type (femur or tibia) with patients treated over the same time period who weighed less than 45 kg and were also treated with FINs (Table 2). We followed the Strengthening the Reporting of Observational studies in Epidemiology (STROBE) guidelines to assure proper quality control of our study. 9 All patient case notes and radiographs were reviewed to construct a database of relevant details. The specific data collected included age, gender, weight, body mass index (BMI), mechanism of injury, concurrent injuries, fracture classification according to the (AO) system, duration of implant surgery, nail size, length of time until union, date of implant removal, duration of removal surgery, complications experienced during surgery, any postoperative complications until final follow-up. Time for union was defined as the earliest time after the index procedure in which at least three cortexes showed bridging on antero-posterior and lateral films. Major complications were defined as delayed union, nonunion, malunion, deep infection, nail breakage, refracture or any condition requiring early nail removal. Minor complications were defined as nail site irritation and superficial infection. Delayed union was defined as lack of bony bridging in at least 3 of 4 cortices on coronal and sagittal radiographs at 3 months, and nonunion was defined by the same criteria at 6 months. 10 Malunion in the femur was defined as shortening of greater than 20 mm at the fracture site, angulation greater than 15° in the sagittal plane (anterior bowing) or 10° in the coronal plane (varus/valgus malalignment). 11 Malunion in the tibia was defined as shortening of greater than 20 mm at the fracture site, angulation of greater than 10° in the sagittal plane or 5° in the coronal plane. 5
Details of patients weighing below 45 kg undergoing flexible intramedullary nailing.
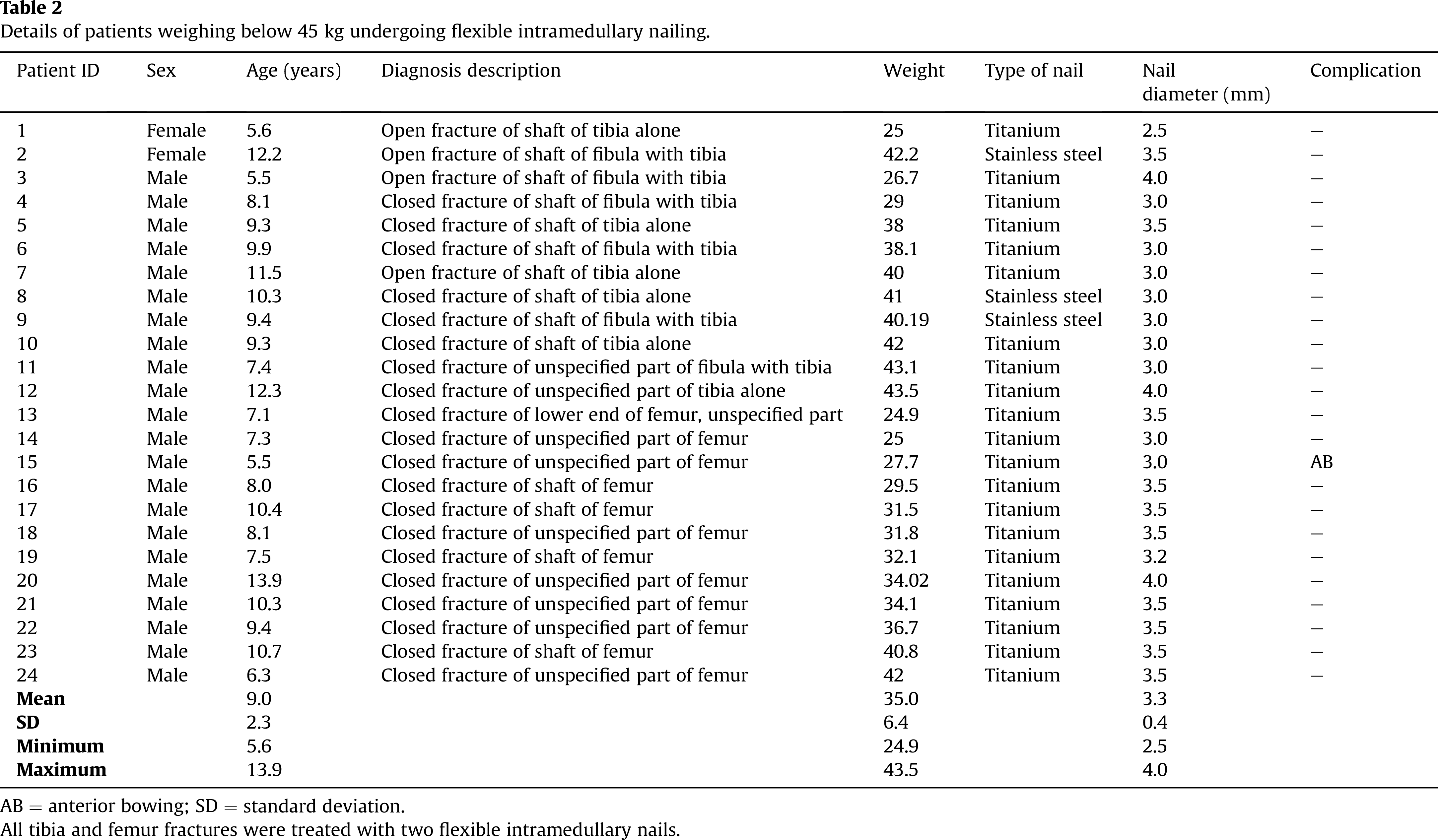
AB = anterior bowing; SD = standard deviation.
All tibia and femur fractures were treated with two flexible intramedullary nails.
All measurements were performed in the picture archiving and communication system by two authors (DV and JJ), twice blinded from each other’s measurement and from their previous measurement. Using a previously validated method, 12 the angles of the lower extremities were measured using the anatomical axis. The specific measurements were the anatomic medial proximal femoral angle (aMPFA) and anatomic lateral distal femoral angle (aLDFA) for the femurs and anatomic medial proximal tibial angle (aMPTA) and anatomic lateral distal tibial angle (aLDTA) for the tibias. Then, to determine the exact degrees of angulation, midshaft lines of the proximal and distal fracture segments were traced, and then the deformity was measured by subtracting from 180° the degrees obtained from the intersection of both lines.
There were 12 patients in the study cohort weighing more than 45 kg (mean weight of 65 kg; range, 48–125 kg). There were 11 males and 1 female with a mean age of 14 years (range 10–17 years) and a mean BMI of 24 kg/m2 (range 17–38 kg/m2). The majority of these patients underwent FIN with stainless steel nails (n = 11) and only one patient underwent FIN with titanium nails. There were six patients who underwent FIN on the femur and six who underwent FIN on the tibia, all of whom suffered a closed fracture. The mean length of follow-up was 1 year.
The matched comparison cohort had 24 paediatric patients, with a mean weight of 31 kg (range 15–43 kg). This cohort had 22 males and two females with a mean age of 9 years (range 6–14 years) and a mean BMI of 20 kg/m2 (range, 15–25 kg/m2). In contrast to the study cohort, most patients underwent FIN with titanium nails (n = 21) and only three received stainless steel nails. There were 22 patients who underwent FIN on the femur for a closed fracture and two who underwent FIN on the tibia for an open fracture. The mean length of follow-up was 1.3 years.
All data were inputted in to an electronic spreadsheet (Microsoft Excel, Microsoft Office; Microsoft Corporation, Redmond, Washington). After defining whether our data were normally distributed or not, either two tailed t-tests or Wilcoxon signed-rank tests were performed to compare outcomes between both groups. Then Fishers exact tests were used to determine if the difference of proportions between the groups is significant. An alpha error of less than 5% was used to determine our differences as significant.
Results
There were no significant differences in terms of major complications between both cohorts. The study cohort had an odds ratio for developing a major complication of 2.1 (95% confidence interval = 0.1–36.6), however this was not significant (p = 0.6). More specifically, there was one case of hypertrophic nonunion in the study cohort (8.3%) and only one case of increased anterior bowing (4.2%) in the matched comparison cohort. Figures 1 and 2 show the injury and the following hypertrophic nonunion case in the study cohort, respectively. There were no instances of nail breakage, refracture, deep infection, early nail removal or minor complications in either group.

Tibial shaft fracture in a 13-year-old male.

Flexible intramedullary nailing, showing hypertrophic nonunion at follow-up.
In the study cohort, the case of hypertrophic nonunion of the tibia was in a 54 kg (BMI 21.91 kg/m2) boy who was 13 years of age at the time of injury. Nonunion was observed and confirmed 6 months after the index procedure. The patient complained of some pain at the fracture site mostly while walking but was very active and seen playing and running by the mother. We attempted conservative treatment with immobilisation and reduced activity, but the patient was lost to follow-up after that visit. Similarly, in the comparison cohort, the case of increased angulation of the femur was in a 6-year-old patient who weighed 28 kg (BMI 22 kg/m2) with an increased anterior bowing of 27° at follow-up 1 year after the insertion surgery (7 days after nail removal).
There were no differences in the alignment between the two cohorts. In the study cohort, the alignment change from postoperative radiograph to latest follow-up was 2.0° [standard deviation (SD) = 3.1°] in the coronal plane and 1.9° (SD 1.8°) in the sagittal plane. In the comparison cohort, the change in angulation was 1.3° (SD = 1.8°) in the coronal plane and 2.8° (SD = 2.2°) in the sagittal plane. Neither of these differences were significant (coronal plane, p = 0.5; sagittal plane, p = 0.2).
In terms of joint angles, there were no significant differences in anatomic angles between the study and comparison groups in the tibias or the femurs. The tibias in the comparison group at latest follow-up had a mean aMPTA of 89° (SD = 2.4°) and aLDTA of 89° (SD = 2.5°). In the study group, the mean aMPTA was 88° (SD = 2.9°) and aLDTA was 89° (SD = 3.2°). These differences were not significant (aMPTA p = 0.3; aLDTA p = 0.8). The femurs in the comparison group at latest follow-up had a mean aMPFA of 88° (SD = 3.6°) and aLDFA of 83° (SD = 3.9°). In the study group, the mean aMPFA was 87° (SD = 4.6°) and aLDFA was 84° (SD = 2.9°). These differences were also not significant (aMPFA p = 0.7; aLDFA p = 0.5).
Discussion
Flexible intramedullary nails are a good surgical option for fixation of paediatric patients weighing less than 45 kg with length-stable femoral and tibial shaft fractures. However, the patient’s weight must be taken into consideration so that the forces of gait will not overcome the strength of internal fixation provided by the hardware. 6 With a growing number of obese children in the United States, it is beneficial to find fixation options for long bone shaft fractures in children weighing more than 45 kg. Stainless steel FINs being stronger and less flexible than titanium FINs 13 may be an option for fixation in heavier children. This study examined cases of FIN fixing femoral and tibial fractures in paediatric patients weighing over 45 kg and compared them to a lighter cohort, finding no significant difference in the rate of major complications and no significant difference in change in angulation between groups from the post-op radiograph until latest follow-up.
There were multiple limitations in our study. Our study group had a small sample size that was retrospectively analysed. Although our mean follow-up was greater than 1 year (426 days), a follow-up of patients until skeletal maturity would be preferred to more thoroughly track any changes in angulation over time. The matched cohort had a different mean age; heavier patients tended to be older; hence, the groups were not matched for this. Nonetheless, this study exemplifies the importance of this possible fixation method in these patients.
To date, there is still debate about the maximum weight limit for a patient who can receive FINs for stabilisation of length-stable diaphyseal femur and tibia fractures. Aslani et al compared intramedullary nails to external fixators in both tibial 1 and femoral2 fractures, finding no significant difference in time to union or increased risk of malunion in both cases. Goya et al performed a randomised controlled trial of titanium elastic nails versus stainless steel elastic nails for femoral shaft fractures in 35 children aged 6–12 years, and follow-up at 6 months found no significant difference in radiological angulation in the sagittal and coronal plane, as well as a similar complication rate in both groups. 14 That study also noted that stainless steel nails are also less expensive than titanium systems. Wall et al 10 compared 56 femoral fractures with titanium nails to 48 femoral fractures with stainless steel nails, finding a lower malunion rate in SS (6.3%) compared to titanium (23.2%) and a higher major complication rate with titanium (35.7%) than SS (16.7%), with similar rates of minor complications, insertion and extraction times. In a multicentre series of 234 femur fractures treated by titanium elastic nailing, Moroz et al found odds ratios for poor outcomes to be 3.86 for children aged 11 years or older and 5.0 for those children that weighed more than 49 kg. 7
Other studies have suggested that FINs may not be the best option in heavier paediatric patients. Deakin et al 5 studied FINs in adolescents aged over 11 years, finding malunion rates of 60% in femur fractures and 38% in tibia fractures, and the mean weight was 56 kg in the malunion group and 45 kg in those without malunion. Porter et al 15 compared titanium elastic nails with submuscular locked plating in paediatric femur fracture models simulating both comminuted and oblique fracture patterns, finding that locked plating provides a more biomechanically stable construct than elastic intramedullary nailing. Miller et al 16 used trochanteric entry, solid, locked, reamed intramedullary nails for femur fractures in 17 patients younger than 12 years with increased risk for malunion because of weight and/or fracture pattern. They found no instances of avascular necrosis, nonunion or malunion, suggesting that osteonecrosis may be avoided in this procedure if the trochanteric entry site is used rather than the piriformis fossa (where there is potential damage to the ascending cervical branch of the medical femoral circumflex artery). Atef and El Tantawy 17 treated 26 open unstable metaphyseo-diaphyseal fractures of the tibia in adolescents aged 13–16 years (mean weight 49.81 kg) with FINs augmented by monolateral external fixation, finding no evidence of angular deformity or limb-length discrepancy. They found that this treatment allowed easy access for wound care and early ambulation, while augmenting the stability of the fixation provided by flexible nails alone.
Conclusion
Stainless steel flexible intramedullary nails can be considered as a treatment option in a properly selected group of paediatric patients who weigh more than 45 kg with length-stable diaphyseal femur and tibia fractures. However, larger cohorts with longer follow-up are needed to aid in the detection of successful union and other complications. More importantly, the clinical and functional outcomes of patients with different fixation types are needed to make any definitive conclusions.
Footnotes
Conflict of interest statement
The authors declare that they have no conflicts if interest to disclose.