
Abstract
A 6-month-old female spayed domestic shorthair cat was presented for evaluation of a focal subcutaneous swelling on the dorsal neck at the level of atlas. The magnetic resonance imaging and surgical treatment of a dermoid sinus associated with the cervical vertebrae is described. To the authors' knowledge, a dermoid sinus in this location has not been described previously in the cat. The prognosis following surgical resection appears favorable.
A dermoid sinus, also termed a dermoid cyst or a pilonidal cyst, arises due to failure of the skin and neural tube to separate completely during embryonic growth. 1 These sinuses may form a small opening to the exterior, as they extend from the skin toward the supraspinous ligament, to which they may or may not be attached.
Dermoid sinuses can affect the cervical, thoracic, sacral and coccygeal spinal cord segments dependent on their location. The neurological signs reflect the location of the sinus. However, not every animal with a dermoid sinus, whether it communicates with the subarachnoid space or not, will have neurological signs. 2 Neurological signs have been reported when the sinus communicates with the subarachnoid space and becomes infected, leading to meningitis, myelitis, or spinal cord compression. Various organisms, including Staphylococcus intermedius, may be cultured from the sinus and analysis of cerebrospinal fluid (CSF) reportedly reveals increased protein content and elevated white cell count if there is an associated meningitis/myelitis present. 3
Myelography can be used to detect the presence of meningeal abnormalities as well as spinal cord compression associated with communicating dermoid sinuses. The use of magnetic resonance imaging (MRI) for the diagnosis and assessment of this disease also has been described in two Rhodesian Ridgeback dogs and would seem to be superior to other imaging modalities in identifying the presence of a dermoid sinus. 4
Cervical dermoid sinuses are extremely rare in veterinary medicine and to the authors' knowledge they have not been reported in cats; only three dermoid sinuses have been reported in cats and these have all affected the thoracolumbar spinal cord.5,6 This report describes a cervical dermoid sinus in a cat and reviews the pertinent literature in veterinary and human medicine.
A 6-month-old female spayed domestic shorthair cat was presented to the Veterinary Teaching Hospital at the University of Georgia, College of Veterinary Medicine for evaluation of a focal subcutaneous swelling on the dorsal neck at the level of atlas. The swelling had been present since the owner adopted the cat at 4 weeks of age. In recent days prior to presentation, the owners had observed moistening of the hair and skin surrounding the swelling. The cat had no prior medical history.
Physical examination was normal with the exception of a 3 cm diameter, round lichenified skin nodule on the dorsal midline aspect of the neck at the level of the atlas, with a focal area of alopecia in the center of the lesion. At the time of presentation, no discharge was visible; however, overnight the hair surrounding the nodule became moist. A suspected ‘stalk’ or tract was palpated extending from the focal skin lesion deep to the subcutaneous tissues and fascia. The lesion was non-painful. Neurologic examination was normal.
Radiographs of the neck were obtained to evaluate the cervical vertebrae for potential osseous lesions. A linear opacity extending from the skin overlying the atlas, deep through the subcutaneous tissue was identified on radiographs. The lesion extended to the dorsal arch of the atlas (Fig 1a). In addition, severe deformity of the cervical vertebral column was observed. There was marked narrowing of the intervertebral discs from C2—C3 to C5—C6 giving the impression that the second through the sixth cervical vertebral bodies were fused with scoliosis; subjectively, the vertebrae appeared wider than normal. Scoliosis was most severe at C2–3 and C3–4 (Fig 1b). At that time, differential diagnoses for the skin lesion and associated stalk included dermoid sinus, a draining tract due to a foreign body, a parasite such as cuterebra larva, tissue abscess, or neoplasia. A complete blood count, serum chemistry panel, and urinalysis were performed. The mild lab-work abnormalities were considered clinically insignificant and were largely attributed to the young age of the cat.

Lateral radiograph of the cervical vertebrae (a). The intervertebral disc spaces of C2—C6 are narrowed which gives the appearance that the vertebral bodies C2 through C6 are fused. Ventrodorsal radiograph of the cervical vertebrae. There is scoliosis which is most severe at C2—C3 and C3—C4 (b).
MRI (3.0 T General Electric Signa HDx, Milwaukee, WI, USA) of the brain and neck was performed under general anesthesia. The cat was premedicated with an intravenous injection of glycopyrrolate, hydromorphone, and midazolam. Induction was achieved with propofol and the cat was maintained under general anesthesia with isoflurane. The following sequences were performed in the axial and sagittal planes: T1-weighted fluid attenuated inversion recovery (T1W FLAIR), T2-weighted (T2W), Short tau inversion recovery (STIR), and three dimensional fast spoiled gradient echo (3D FSPGR) sequences. In addition, T1W FLAIR and 3D FSPGR images were obtained following administration of gadopenetate dimeglumine (Magnevist, Berlex Laboratories, Wayne, NJ, USA) at a dose of 0.1 mmol/kg of body weight.
The lesion affecting the skin was difficult to discern on digital examination. The extent and course of the palpable subcutaneous lesion was visible on MRI. Superficially, the lesion was present in the subcutaneous fat and extended cranially and deep to the level of the dorsal arch of the atlas. A depression in the epaxial muscle was identified at the point where the lesion penetrated the muscle (Fig 2). In comparison to the surrounding muscles, the lesion had the following characteristics; the lesion was iso- to slightly hyperintense on T1W FLAIR and hyperintense on T2W images. Additionally, in the portion of the lesion contained within the epaxial muscles there was a central area that was hyperintense with a thin hypointense tissue surrounding it on all imaging sequences. At the level of spinal is cervicis muscles extending deep to the dorsal arch, the lesion had discrete borders; however, the portion that extended superficially had ill-defined borders. On the sagittal images, the lesion was surrounded by tissue with imaging characteristics consistent with fat.
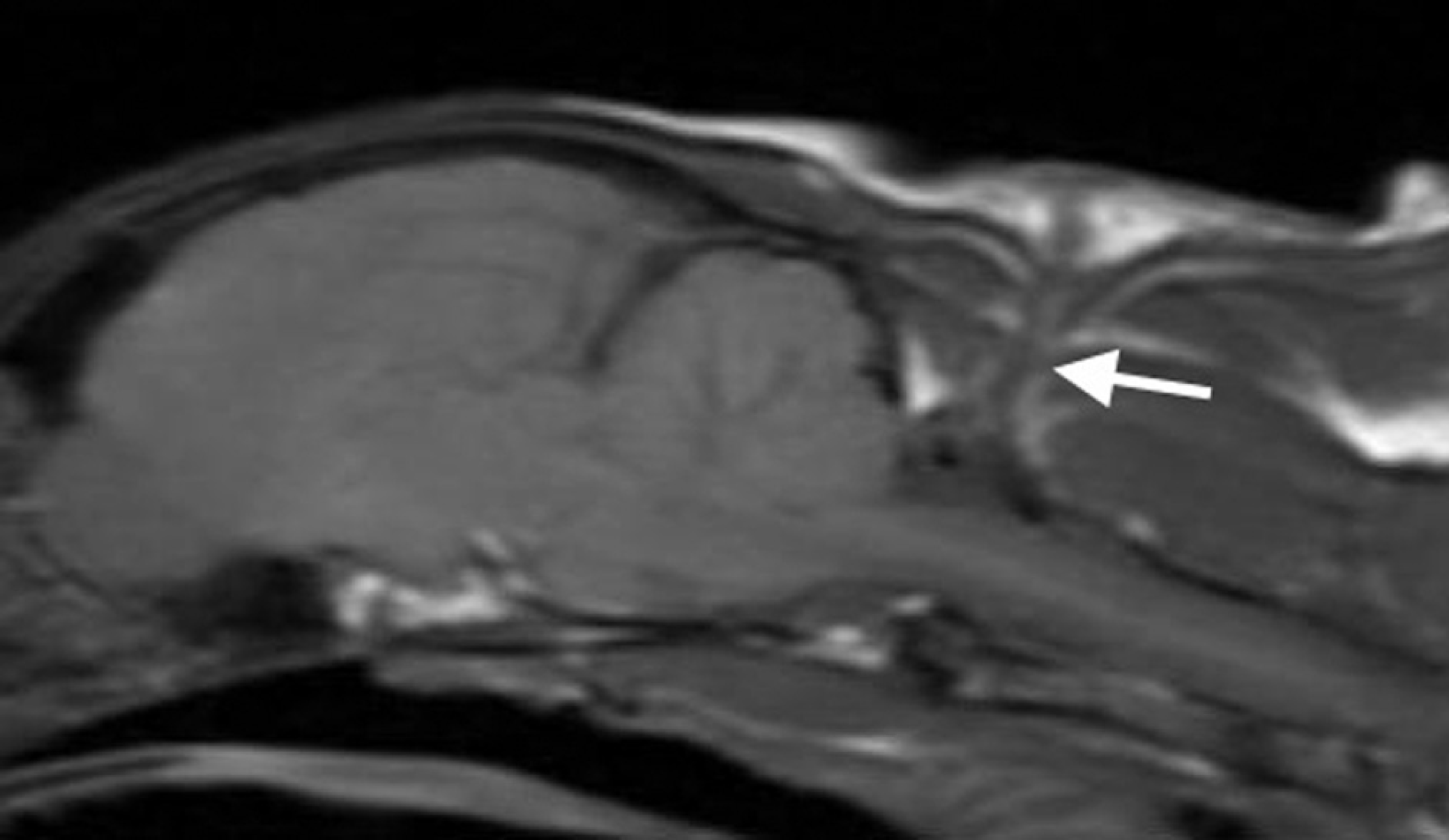
A sagittal T1W FLAIR image of the brain and cranial spinal cord. The palpable subcutaneous lesion is observed in the subcutaneous fat. There is a visible depression in the epaxial muscles as the lesion penetrates the muscle. The lesion extends deep to the muscle to level of the dorsal arch of the atlas (white arrow).
At the cranial margin of the atlas, there was a midline defect in the dorsal arch (Fig 3). At the level of the defect, the dorsal meninges extended to the arch of the atlas which resulted in the subarachnoid space taking on a slight triangular shape in the axial plane (Fig 4). While present on T2W sagittal images, this area was best appreciated in the axial plane on the T2W, STIR, and post-contrast FSPGR images. On T2W images, this area of dorsal expansion was hyperintense while on T1W FLAIR, and FSPGR axial images, this area was hypointense. The MRI characteristics of the dorsal extension of the subarachnoid space at the cranial margin of C1 were most consistent with CSF. Despite this, it is possible that the triangular shape may have represented attachment of the lesion to the dorsal midline aspect of the dura. The lesion contrasted minimally after IV gadolinium administration. Additionally, on the T2W images, there was a lack of signal from the nucleus pulposus of the intervertebral discs from C2—C3 to C5—C6.
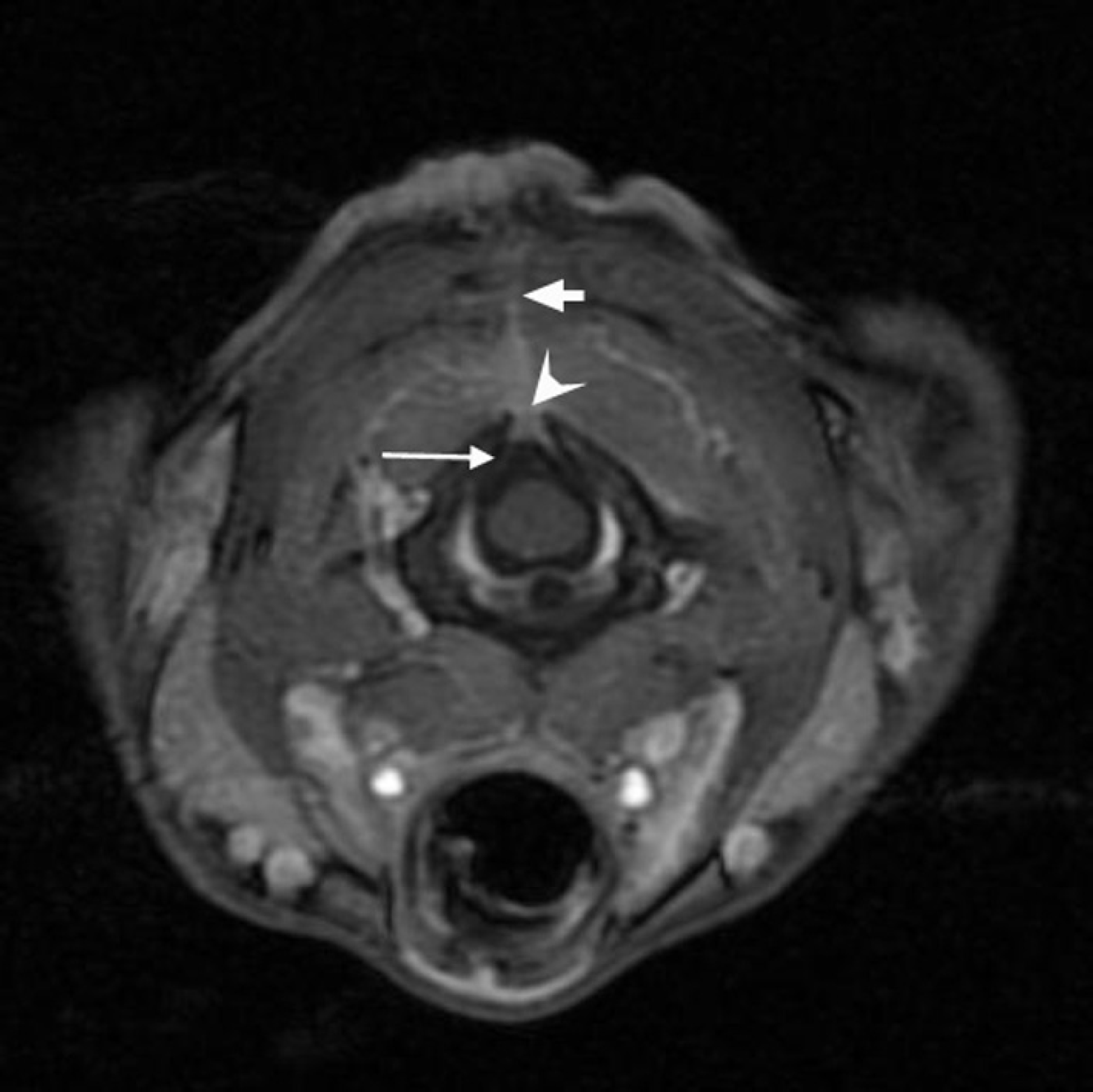
A 3D FSPGR axial image at the level of the cranial aspect of the atlas. The 3D FSPGR was performed utilizing a chemical fat saturation pulse. There is a midline defect in the dorsal arch of the atlas (white arrowhead). In comparison to the muscle, the palpable subcutaneous lesion is visible as a hyperintense structure (short white arrow). There is an expansion of the dorsal subarachnoid space (long white arrow).

T2W axial image at the level of the atlas. The palpable subcutaneous lesion is observed in the epaxial muscles overlying the atlas (white arrowhead). There is a deviation of dorsal meninges toward the defect in the arch of the atlas which results in a triangular shape of the subarachnoid space in the axial plane (white arrow).
Although the MR (Magnetic Resonance) images were suggestive of a contiguous structure connecting the skin lesion with the meninges, a definitive connection could not be confirmed. To better define the relationship between the skin lesion, palpable subcutaneous structure, and meninges, myelography was performed using iohexol (Omnipaque 300, Winthrop-Breon, New York, NY, USA) at a dose of 0.4 mg/kg injected into the subarachnoid space between L5 and L6 vertebrae. The myelogram was normal with the exception of an area at the level of the cranial margin of the dorsal arch of the atlas where the subarachnoid space was expanded dorsally, similar to what was observed on sagittal T2W images. A communication could not be appreciated between the palpable stalk and subarachnoid space. Fistulography was not performed, as an opening at the epidermis could not be identified. Analysis of CSF obtained from the cisterna magna prior to myelography was normal.
Following myelography, surgical dissection was undertaken immediately for removal and histological evaluation of the lesion. An oval skin incision was made around the structure in the epidermis. The dissection along the dorsal midline musculature allowed visualization of the lesion as a thin fibrous band extending deep through the musculature to the level of dorsal arch of the atlas. A large branch of the lesion and one additional minor branch located more cranially were identified. The lesions were ligated superficial to their deep attachment at the dorsal arch of the atlas, using 3.0 Polydioxanone (PDS; Ethicon, Johnson & Johnson). A discrete attachment to the meninges was not appreciated.
Histologically, the lesion was composed of a central portion of fibrous tissue oriented perpendicular to the skin surface. The tissue extended from the mid-dermis to the deep surgical margin and consisted of mature eosinophilic collagen fibers, representing fibrosis, and numerous, haphazardly arranged fibroblasts intermixed with small blood vessels. Intermixed in the granulation tissue were rare neutrophils, mast cells, and eosinophils. There was no histological evidence of dural tissue or neoplasia. No infectious organisms were observed after staining with hematoxylin and eosin, Gram stain, or Gomori methenamine staining (GMS). Based on the young age of the cat, the lack of significant associated inflammation, and the location of the tissue, the lesion was considered to be a developmental anomaly, or congenital dermoid sinus. The cat recovered uneventfully from surgery and was monitored postoperatively for 3 days during which time the cat remained neurologically normal.
Two months following surgery the cat's neurological examination was normal. The surgical site had healed without complication; however, the owner reported that since shortly after surgery the cat had been scratching around the surgical site and left ear. On examination, there was superficial dermatitis affecting the pinna and skin surrounding the ear; amoxicillin/ clavulanic acid was prescribed. However, the skin lesion worsened and at subsequent evaluation a few weeks later, the cat had an ulcerated area of skin at the surgical site. Otoscopy revealed no evidence of infection. The skin was treated topically with Tricide solution [Tris ethylenediaminetetraacetic acid (EDTA)]. At the time of last communication about 6 weeks postoperatively, the cat had responded well to the Tricide solution and the scratching had improved. The owner also reported no change in the neurologic status at that time.
A dermoid sinus is the result of embryologic maldevelopment in which there is failure of the neural tube to completely separate from the ectoderm. Typically, the lining of the sinus is comprised of structures found in skin including hair follicles and glands with a lumen incorporating hair, cells, and glandular debris. 1 There are five types or classes of dermoid sinuses documented in the human literature, based upon the tissue type involved:6,7 type I extends deep from the skin or subcutaneous tissue as a cylindrical sac to the level of the supraspinous ligament but it is not attached to this ligament; type II is a superficial sac that does not extend to the supraspinous ligament, but it attaches to the ligament via a fibrous band; type III is a superficial sac that does not extend to the supraspinous ligament; type IV penetrates the vertebral canal and attaches to the dura mater; and type V is a ‘true’ cyst composed of a closed epithelial lined sac with no communication to the skin. 8 It is likely that the cat described in this report had a type IV dermoid sinus, as it extended deep to the dorsal arch of atlas at surgery, although a connection to the dura mater was not confirmed.
A review of the veterinary literature on dermoid sinuses revealed limited information, isolated to case reports or case series. Dermoid sinuses are reported more commonly in the dog as compared to the cat, with most case reports describing tracts in the lumbosacral area. Dermoid sinuses have been described in a variety of dog breeds.9,10 In the cervical region, dermoid sinuses have been documented in the Golden Retriever, 11 Boerboel, 12 and Rhodesian Ridgeback. 10 Multiple case reports in the Rhodesian Ridgeback have led to research which suggests that there is a genetic connection between the cutaneous ridge and development of dermal sinuses related to fibroblast growth factor genes, specifically duplications in FGF3, FGF4, FGF19, and ORAOV1. 13 While a genetic basis may exist in the Rhodesian Ridgeback, the etiology of this defect in other breeds and species has yet to be elucidated.
Only three cases of dermoid sinuses in cats have been documented. The first two cases were described by Rochat et al; a subcutaneous lumbar mass on the left side of the vertebral column, palpated deep within the abdominal muscles in a 10-year-old domestic shorthair and four separate masses in a linear array deep within the tissues of the right paralumbar region in a 7-month-old domestic shorthair. 6 In the 10-year-old cat, the sinus was described at surgery as a well-circumscribed, encapsulated mass between the internal abdominal oblique and transverse abdominus muscles with minimal vascular supply. 6 Histology revealed a cyst filled with keratin and lined with stratified squamous epithelium, having the appearance of normal epidermis. 6 In the 7-month-old cat, the sinus was described similarly as four masses tethered together by connective tissue which extended through the flank muscles to the peritoneum. 6 Histology of the lesions from this cat revealed that the masses were composed of haired skin with dermal cystic structures lined by squamous epithelium; within the lumen of the cyst, squamous debris and hair shafts extended from the cyst wall. 6 Histology of both of the lesions was consistent with subcutaneous dermoid sinuses, similar to the dorsal midline structures described in dogs. As neither of these dermoid sinuses extended to the spinal canal or supraspinous ligament, and both were present in the flank area, it is not possible to grade them further. Neither of the lesions communicated with the neuraxis. The third case was a 16-month-old Balinese which presented for ataxia and was diagnosed with a dermoid sinus at the level of the third thoracic vertebrae. 5 Neurologically, the affected cat displayed postural reaction deficits, a crouched posture, and was nonambulatory paraparetic with fecal and urinary incontinence. 5 Based on the clinical signs and neurological deficits, a compressive lesion was suspected between the second thoracic and third lumbar spinal cord segments. Euthanasia was elected due to the advanced and chronic clinical signs and poor prognosis for return to complete function. 5 At necropsy, the spinal cord was swollen at the level of the third thoracic vertebrae. Histology of the lesion revealed a cystic structure connected to the meninges dorsally, and enclosed in a dense connective tissue capsule with hair follicles and sebaceous glands. 5 In contrast to the cat in the dermoid sinus, the lesion did not communicate with the subcutaneous tissues or skin.
In humans, about 60% of dermoid sinuses communicate with the subarachnoid space; of all sinuses reported in the human literature, up to 30% are attached to the conus or filum terminale, 10–20% terminate blindly in the extradural space, and less than 10% terminate in the subcutaneous tissue or adjacent musculature. 14 Similar to the cat described herein, humans primarily seek evaluation due to infection or irritation of the skin; neurologic deficits are infrequent, despite the large percentage of skin lesions contiguous with the central nervous system. 15
Given the ability to discern soft tissue structures, MRI provided detailed information regarding the anatomic relationships between the dermoid sinus, vertebral column, dura and spinal cord in the cat reported here. In humans, dermoid sinuses typically appear hypointense on T1W images and hyperintense on T2W images with enhancement on T1W images after administration of gadolinium. 16 If the sinus is lipid lined, the structure may be hyperintense on both T1W and T2W images. 14 The dermoid sinus in the cat reported here had similar imaging characteristics as those observed in humans. In the portion of the dermoid sinus near its attachment to the dorsal arch of the atlas, the central region was hyperintense on both T1W and T2W images consistent with lipid. Despite such characteristic imaging findings, MRI may not provide a definitive diagnosis. Consequently, surgical exploration often is pursued following imaging to define the extent of the sinus. 16
The purpose of this manuscript was to document the occurrence, and to describe the MR characteristics and surgical treatment of a dermoid sinus associated with the cervical vertebrae of a young cat. To the authors' knowledge, a dermoid sinus in this location has not been described previously in the cat. Based on this report, the discovery of a skin lesion along the dorsal midline in animals with no known trauma should raise the suspicion for a dermoid sinus and careful palpation may reveal extension toward the vertebral column. Animals with a suspected dermoid sinus should undergo a thorough neurologic exam to identify the presence of deficits which would incriminate involvement of the neural axis. Ultimately, MRI should be performed to characterize the anatomical relationships of the surrounding anatomy. The prognosis following surgical resection appears favorable in the limited cases reported.