
Abstract
Case 1
A 16-month-old female spayed domestic shorthair cat was presented to the emergency facilities with a 3-day history of vomiting, apathy and anorexia. On presentation, the cat was reluctant to stand. Physical examination showed evidence of systemic shock (hypothermia, pale mucous membranes, prolonged capillary refill time and tachycardia). Abdominal palpation revealed abdominal distension, discomfort and several cylindrical intra-abdominal structures.
The cat was warmed using a warming blanket and treated with intravenous fluids (lactated Ringer's solution [Fresenius Kabi] and hetastarch), buprenorphine (0.014 mg/kg q4h IV, Temgesic; Essex Chemie, Switzerland) and amoxicillin/clavulanic acid (20 mg/kg q8h IV, Augmentin IV; GlaxoSmithKline). Laboratory examination revealed anaemia (haematocrit 10%; reference interval [RI] 33–45%), leukopenia (white blood cells 2.5 × 10 9 /l; RI 4.6–12.8 × 10 9 /l), thrombocytopenia (45 × 10 9 /l; RI 180–680 × 10 9 /l) and mildly elevated urea nitrogen (24.11 mmol/l; RI 6.28–11.71 mmol/l). Further values were within normal limits, but blood gas analysis was not performed.
Thoracic radiographs were unremarkable. Abdominal radiographs displayed marked distension of gas-filled small intestinal loops and patchy serosal detail (Fig 1). Abdominal ultrasound revealed two distinct populations of intestinal loops surrounded by free abdominal fluid. One population comprised distended bowel loops displaying regional asymmetric wall thickening with layering maintained. Intestinal peristalsis was absent, but no intraluminal or intramural obstruction could be seen. The other population of intestinal loops appeared normal. Doppler ultrasonography was not performed to measure intestinal perfusion.

Preoperative laterolateral and ventrodorsal radiographs of case 1 showing distended intestinal loops and loss of detail in the mid-abdomen
Based on these findings extraluminal obstruction or regional paralysis with secondary effusion was suspected and surgery recommended.
Surgical findings, treatment and outcome
A standard midline exploratory coeliotomy was performed, following a whole blood transfusion (50 ml, type A). After removing 200 ml of intra-abdominal serosanguineous fluid, grossly distended bowel loops were identified. These had undergone a 360° clockwise rotation around the mesenteric root and were herniated through a tear in the mesenterium; the tear was located halfway between the intestines and the mesenteric root in the mesenterium in the middle of the jejunum. The affected portion of the bowel extended from the middle of the jejunum to 1 cm oral of the ileocaecocolic junction. Thrombi were evident within the venous mesenteric vessels. The volvulus was corrected as previously described, 1 allowing decompression of the distended bowel segment. Approximately 45 cm of small intestine was considered devitalised. This was resected and an end-to-end anastomosis was performed with two simple continuous suture patterns (Fig 2) using polydioxanone (PDS 4/0) on a 3/8 tapered cutting needle, leaving approximately 50–60 cm of small intestine remaining. The anastomosis site was subsequently omentalised and the abdomen was lavaged prior to closure.

Postoperative view of sutured intestines in case 1
Histological examination of the resected segment revealed severe haemorrhage of the small intestine with necrotising enteritis.
The cat made a satisfactory recovery from surgery and was discharged 72 h later. Four months after surgery, the cat was reported to suffer from diarrhoea, which did not improve with various dietary modifications. Despite this, the owner was satisfied with the outcome of surgery.
Case 2
A 5-year-old male Bengal cat was presented to the emergency facilities with a 1-day history of lethargy and vomiting. On presentation, the cat was in lateral recumbency. There was evidence of severe shock on physical examination. Abdominal palpation revealed discomfort and a mid-abdominal mass.
The cat was warmed using a warming blanket and treated with intravenous fluids (lactated Ringer's solution and hetastarch), buprenorphine (0.014 mg/kg q4h IV), clindamycin (11 mg/kg q12h IV, Antirobe; Pfizer) and enrofloxacin (5 mg/kg q24h IV, Baytril; Bayer). Initial blood work revealed mild anaemia (haematocrit 20%; RI 33–45%) and leukocytosis (white blood cells 24 × 10 9 /l; RI 4.6–12.8 × 10 9 /l). Other values were within normal limits; acid-base status was not evaluated. Abdominal radiographs revealed distended small intestinal loops, which appeared to be piled onto one another, and occasional gas bubbles both within the small intestinal loops and free within the epigastric and hypogastric areas. Based on these findings, either intussusception or mechanical obstruction and perforation of the gastrointestinal tract was suspected and surgery was recommended.
Laboratory re-evaluation following fluid therapy showed severe anaemia (haematocrit 10%; RI 33–45%) and hypoalbuminaemia (9 g/l; RI 30–40 g/l). A transfusion of one unit (30 ml) of fresh frozen plasma and one unit (50 ml) of whole blood was administered and a standard midline coeliotomy was performed.
Surgical findings, treatment and outcome
A mesenteric volvulus, in which the intestines had rotated 270° around the mesenteric root in a clockwise direction, was found (Fig 3). The affected intestines — extending from the middle of the jejunum to the ileum — were black and severely distended. Although no thrombi were observed, no pulse was palpable in the mesenteric vessels. An enterectomy of approximately 40 cm of the jejunum and proximal ileum, preserving the ileocolic junction, and an end-to-end-anastomosis with two simple continuous suture patterns of poly-dioxanone (PDS 4/0 on a 3/8 tapered cutting needle) were performed. Omentum was placed around the anastomosis of the approximately 60 cm of small intestine remaining and the abdomen was lavaged and closed.
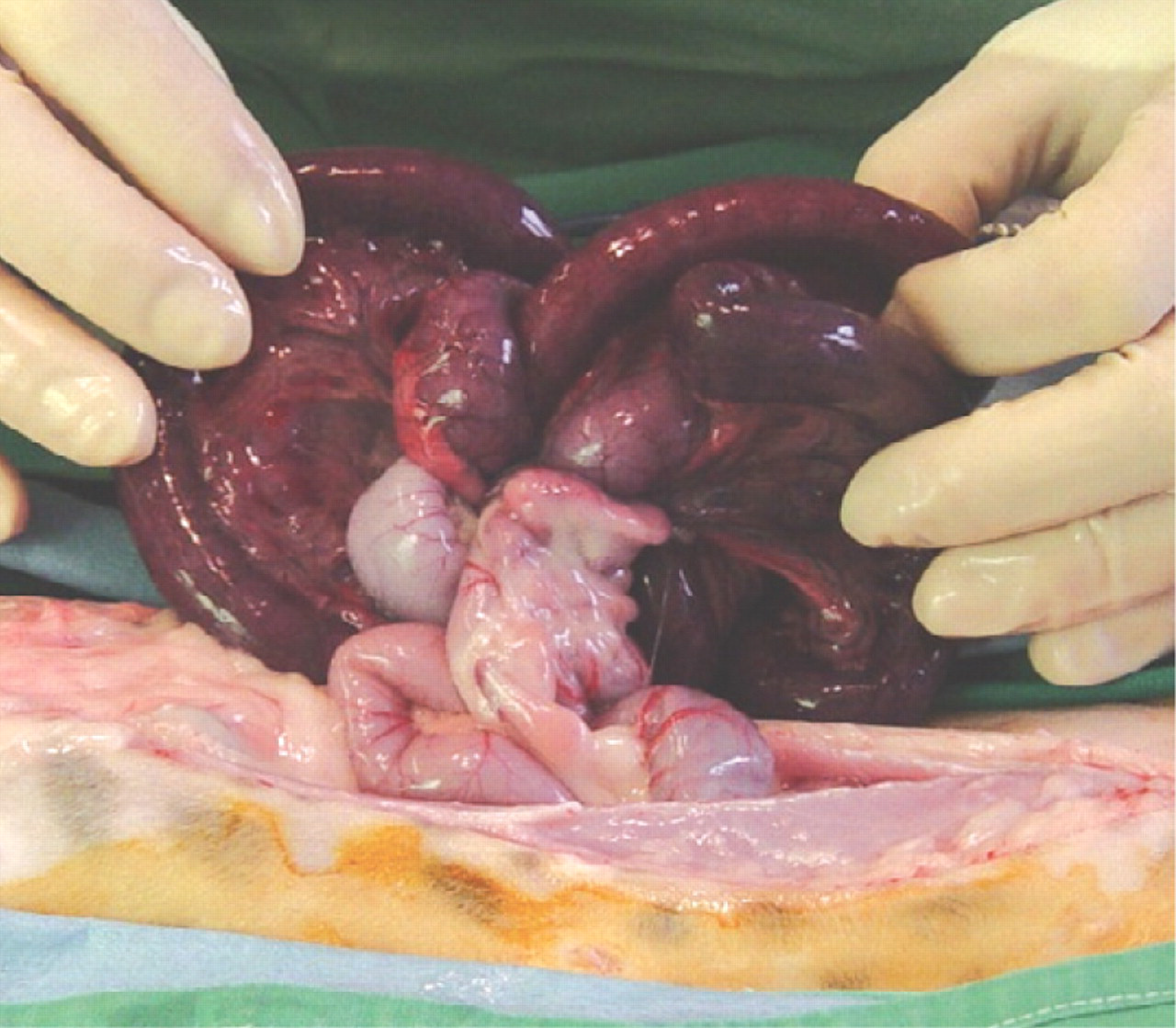
Intraoperative examination of rotated intestinal loops in case 2
Histological examination of the resected loop revealed necrosis of the mucosa and submucosa, and severe vascular stasis and haemorrhage, which was interpreted as haemorrhagic infarction.
The cat recovered and was discharged after eating normally on day 6 following surgery. Two years later, the cat died in a road traffic accident. The owner reported persistent soft stools, which improved temporarily with the administration of metronidazole (10 mg/kg q12h PO, Flagyl; Sanofi-Aventis), from the time of discharge until death. Despite this, the owner was satisfied with the outcome of surgery.
Discussion
Mesenteric volvulus is an uncommon condition in dogs, with a breed predisposition reported in German shepherd dogs. 1–3 Torsion of the small intestine around the mesenteric root can be partial or complete. 3–6 A case of chronic (4-month, partial) mesenteric volvulus has been published. 4 In previously reported cases of intestinal volvulus involving cats, the patients (three in total) have not survived. 7,8
In the cats in this report, one was found to have a classical volvulus around the mesenteric axis, similar to previously reported canine cases. 1–3 In the other, herniation of jejunal loops through a mesenteric tear, with partial torsion around the mesenteric root, was observed. This presentation is described in large animals, especially horses, in which small bowel loops herniate through mesenteric defects, presumably caused by previous trauma, with subsequent volvulus. 9
Diagnosis of intestinal volvulus in dogs is usually based on clinical and radiographical findings. Abdominal radiographs typically reveal distended gas- and fluid-filled intestines with small bowel loops lying parallel to each other, and loss of serosal detail. 2,5,6 In the feline cases presented here, a radiographic diagnosis of volvulus was not as straightforward. Not only, therefore, may diagnosis be more challenging in cats than in dogs, but the condition also might be all the more unexpected in cats. A whirlpool sign may be encountered on ultrasound examination, as well as on computed tomography (CT) scans, created by the malposition of the mesenteric artery and vein, which is described in human medicine. 10 In the first cat, on the basis of radiographic findings of free abdominal gas, further diagnostics were not performed, similar to previously published cases. 11 The second case revealed signs of segmental ileus and focal wall thickening most likely due to wall oedema. These findings are consistent with small intestinal volvulus, but a thrombus was not confirmed.
The prognosis for dogs with volvulus is considered extremely grave unless immediate diagnosis and treatment is achieved or the torsion is only partial, both of which are seldom the case. 6 Indeed, clinical outcome appears to depend largely on the degree of rotation and the time elapsed between the onset of clinical signs and treatment. 12 However, clinical signs were apparent for between 1 and 3 days prior to treatment in the cats in this report. Immediate recognition and treatment of intestinal volvulus may, therefore, be less critical in cats than in dogs. It remains unclear if partial volvulus is typical of this disease in cats, as seen in case 1, and/or if volvulus in cats in general has a better prognosis. We are not able to explain the pathogenesis of partial small intestinal volvulus or the better outcome in cats in comparison with dogs; nor are we aware of anatomical differences except for the shortened overall length of the intestine of the cat. 13
Both cats in this report suffered long-term postoperative diarrhoea, which is likely due to short bowel syndrome following resection of large lengths of the small intestine. 14,15 This might be an important long-term complication that must be considered if extensive (in these cases, approximately 40–50%) small bowel resection is performed in cats with small intestinal volvulus. Despite this complication, the owners of both cats were satisfied with the outcome of surgery. In a retrospective case series to determine the outcome in cats and dogs undergoing still more extensive (>50%) resection of the small intestine, the length of resected intestine was not associated with the outcome, and four of the five examined cats had a favourable outcome. 16 Given that the present cases underwent less extensive resection than was reported in that study, it might be assumed that the resulting diarrhoea is not solely due to the resection and that, possibly, other unknown circumstances caused damage to the remaining intestinal loops.
The cases described in this report suggest that the diagnosis of intestinal volvulus may be more difficult in cats than in dogs and that preoperative radiographs may be suggestive only of obstruction. Given volvulus in a herniated mesenterium in one cat, surgeons should consider repair of mesenteric tears in cats to avert volvulus. The prognosis in cats may not be as poor as in dogs and owners should be encouraged to agree to surgery but should be made aware of a risk of short bowel syndrome.
Ultimately, however, as only two cases are presented, further studies (evaluating pathogenesis, outcome and anatomical differences) are warranted before general conclusions about volvulus in cats can be made.
Acknowledgements
The authors wish to thank Dr J Howard for her writing assistance.