
Abstract


Long-Term Pain In Cats
A sister article reviewing the current state of knowledge on long-term pain in cats, including issues such as persistent postsurgical pain and diabetic neuropathy, appears on pages 188––199 of this issue of J Feline Med Surg, and at: doi:10.1016/j.jfms.2010.01.002
A detailed review of the literature pertaining to both the noninflammatory and inflammatory forms of feline DJD has recently been published. 1 The focus of the present review are the clinical aspects of diagnosing and treating pain associated specifically with non-inflammatory (eg, non-immune-mediated, non-infectious) DJD.
How prevalent is radiographic evidence of feline DJD?
Degenerative joint disease occurs in both the axial and appendicular skeleton. Beadman et al performed the first extensive radiographic evaluation of DJD of the feline axial skeleton in 1964. 2 Since then, the studies that have been performed suggest that the most frequent site of axial skeleton DJD is the T7–10 area.3–6 The most severe lesions, however, appear to be in the lumbar or lumbosacral area. The reported incidence of axial skeleton DJD differs markedly between the different studies, which is likely to reflect the increasing frequency of axial skeleton DJD with age, and partly also differences in how DJD has been defined. For the appendicuar skeleton, the available information suggests that the most commonly affected joints are the hip and elbow, followed by the stifle or possibly tarsus.3–9 As for the axial skeleton lesions, there are differences between the studies in how DJD is defined. Hardie et al 3 claimed that all joints with radiographic signs of DJD were osteoarthritic, while Clarke et al 4 attempted to distinguish between radiographic signs of DJD such as enthesiophytes and soft tissue mineralization (which may not represent osteoarthritis) and osteoarthritis.
Long-Term Pain in Cats
However, the studies referred to above were performed using radiographs that were sourced from the practice archives — these were often thoracic or abdominal views and not necessarily films that had been taken of the skeleton per se. This is obviously going to bias the joints available for evaluation in such studies. No studies have yet been published where every joint has been evaluated in a randomly selected population of cats to ascertain the prevalence of DJD in this species. Recently, one of the authors (BDXL) performed a cross-sectional study designed to evaluate the prevalence of feline appendicular and axial skeleton DJD. Using a database of 1640 cats from a single practice (Morrisville Cat Hospital, Cary, NC, USA), a population of 100 cats, equally distributed across four age groups (6 months to 5 years, 6–10 years, 11–15 years and 16–20 years), was randomly selected (regardless of health status) to participate in the study. Thorough evaluation of orthogonal radiographs of every appendicular joint and every part of the axial skeleton showed that 91% of the 100 randomly selected cats (with ages equally distributed across the age range from 6 months to 20 years) had at least one appendicular joint with radiographic DJD. 10 The most frequently affected joints were the hip, followed by the stifle, tarsus and then elbow. Fifty-five percent of the cats had axial column DJD. The thoracic segment was most frequently affected, followed by the lumbo sacral area. Much of the DJD seen was mild and the radiographic appearance often differed from that seen in the dog. Only age was significantly associated with the presence of DJD. Bodyweight, body condition score and sex were not significantly associated with the presence of DJD. This study indicates that the prevalence of DJD in domesticated cats is high. Examples of the radiographic features in moderately affected hip, stifle, hock and elbow joints — the most commonly affected appendicular joints — are shown in Figs 1 to 4.

Elbow (14-year-old cat). Craniocaudal projection (a) shows osteophytes in the area of the medial coronoid of the ulna and on the medial distal humerus. There is evidence of osteophytosis or mineralization of the soft tissues on the lateral aspect of the distal humerus. The mediolateral projection (b) shows significant perijoint osteophytosis and soft tissue mineralization. Some of the periarticular soft tissue mineralization (joint-associated mineralization) is shown in (c), an oblique view highlighting the cranial and caudal aspects of the joint. These mineralized fragments (both cranially and caudally) are usually found attached to the joint capsule, often projecting into the joint. Cartilage damage is seen in joints showing this joint-associated mineralization

Hips (11-year-old cat). The ventrodorsal view of the pelvis (a) shows bilateral DJD, with significant new bone on the cranial effective acetablular rim (cranial part of the acetabulum seen on the ventrodorsal projection) and an apparently shallow acetabulum bilaterally, and new bone formation at the attachment of the joint capsule on the neck of the femur (possibly similar to the ‘Morgan's’ line seen in dogs). Note there is relatively little osteophytosis of the femoral neck or other areas of the acetabulum — signs frequently seen in dogs with hip DJD. New bone at the cranial effective acetabular rim in the form of a ‘triangle’ is a prominent and common feature of feline hip DJD. (b) Enlargement of the right side of (a)

Hock (14-year-old cat). The mediolateral view (a), which is slightly oblique in projection, shows osteophytosis on the cranial aspect of the distal intertarsal joint — a common finding in feline hock DJD. Subjectively, the tibiotarsal joint appears ‘narrow’, but this is very difficult to assess. Also seen is some degenerative change on the proximal aspect of the calcaneus. The craniocaudal view of the same hock (b) shows scant evidence of DJD, with a little roughening of the distal lateral aspect of the calcaneus. The craniocaudal view is often of low yield in determining whether DJD is present

Stifle (2-year-old cat). On the mediolateral view (a), mineralization between the femur and tibia is likely to be meniscal mineralization (a common condition in cats), and recent work has shown that this feature is predictably associated with cartilage damage, especially on the medial femoral condyle. 11 The craniocaudal view (b) shows the apparent intra-articular mineralization. This mineralization is found in the cranial horn of the medial meniscus
Radiographic appearance of DJD in the elbow and hips of cats
Radiographic appearance of DJD in the hocks and stifle of cats
These examples demonstrate what the authors consider to be moderate radiographic signs for the joint in question.
Further research by Mila Freire working in Lascelles' laboratory has evaluated the gross and histological appearance of joints and related this to the radiographic findings (unpublished observations). This has shown that the radiographic features assessed in previous studies are indicative of cartilage damage, and also that there are many joints of middle-aged cats that have significant cartilage damage, but no radiographic signs of DJD. This confirms previous suggestions that feline DJD may be associated with less of a tendency to form new bone than its canine counterpart.3,4
Are radiographic features of DJD associated with pain?
In the study by Hardie et al, 3 although 90% of the cats evaluated had radiographic evidence of axial and/or appendicular skeleton DJD, only 4% had any mention of arthritis or problems with mobility in their medical records. The records being evaluated were referral hospital records, and the cats were not primarily referred for mobility problems. It is not known for how many of these cases the referring veterinarians' records were also available for review. In a similar study by Godfrey, 9 approximately one-third of cats (21 out of 63) with radiographic appendicular joint osteoarthritis had clinical signs of mobility impairment (lameness, stiff gait, difficulty jumping, hind limb weakness, shuffling fore limb gait and inactivity), and in fact were radiographed for that reason. In another retrospective radiographic study of the prevalence of DJD in cats, 16.7% of cats with radiographic signs of DJD were reported to be lame. 4 However, the authors of this last study suggested that lameness per se may not be the most obvious clinical sign associated with feline DJD.
In contrast to these suggestions that radiographic signs of DJD may not be obviously associated with lameness or mobility impairment, several studies have indicated that there exists a population of cats with radiographic DJD that are mobility impaired,5,6,12,13 and that this mobility can be significantly improved following administration of a non-steroidal anti-inflammatory drug (NSAID). Together, this suggests radiographic DJD can be associated with pain.
However, there appears to be a mismatch between the radiographic findings and the clinical examination findings. In the study by Clarke and Bennett, 5 the presented data suggests that 34% of joints assumed to be painful on manipulation during a clinical examination did not have any signs of radiographic osteoarthritis. In another study, where every joint was radiographed and also evaluated by careful physical examination in the fully conscious cat, there was only moderate overlap between the parameters of ‘radiographic DJD’ and ‘pain on manipulation’. 6 In that study, 55 joints had radiographic signs of osteoarthritis (using the radiographic criteria widely employed for assessing canine osteoarthritis, which are assumed to be relevant to cats), but only 18 (33%) of these were painful on manipulation. This appears to support the notion that radiographic osteoarthritis is not necessarily associated with pain in cats. It also supports the suggestion that some radiographically normal joints may be painful — possibly due to DJD. Further work by one of the authors (BDXL) has confirmed that the sensitivity of pain on manipulation to predict radiographic DJD is low, but that the sensitivity of crepitus, thickening or effusion to predict radiographic DJD is reasonably good (60–80%) (unpublished data).
Just as in other species, it is important to remember that radiographic findings of DJD in cats should be used to confirm our suspicions of the presence of the disease process, and not to guide treatment. It should also be borne in mind that it appears that cats do not appear to form as much radiographic pathology as other species, and so the absence of obvious radiographic signs does not preclude the presence of DJD that may be associated with pain. Importantly, a thorough evaluation for other orthopedic or systemic disease that may result in impaired mobility (such as Achilles tendonopathy, diabetes with accompanying diabetic neuropathy, or cardiac disease resulting in exercise intolerance) should be performed.
Assessing feline patients for DJD-associated pain
In dogs, most of us are familiar with using a combination of owner history, examination findings and radiography to make an assessment of whether DJD-associated pain is present. Generally, by adopting this three-point approach, we can be relatively certain about the diagnosis — that is, to use a phrase coined by Dr Samantha Lindley, ‘the triangle of uncertainty’ is small (see right). Additionally, in dogs, signalment can provide very strong clues as to whether to suspect DJD-associated pain and an underlying disease.
By contrast, with so much less known about feline DJD, and many veterinarians' perceptions that cats are difficult to examine for orthopedic disease, coupled with a general lack of knowledge about what the radiographic signs of feline DJD are, the ‘triangle of uncertainty’ becomes much larger. The clinical approach to the feline patient should aim to make this triangle as small as possible through gathering a reliable history, and conducting performance tests, an orthopedic examination, radiography and other diagnostic tests.
History of impaired mobility and activity
Due to the nature of chronic pain associated with DJD, which is generally gradual in onset, the accompanying behavioral changes can be subtle and easily missed. In people, questionnaire based outcome measures have been developed, validated and reasonably well accepted. Subjective outcome measures are less well developed in veterinary medicine, although progress has recently been made in canine medicine in relation to DJD.14–18 Little work on the assessment of osteoarthritic pain has been performed in cats. 56 However, it appears from early work that an approach similar to that in dogs is likely to be most successful — that is, based assessments.
Multimedia
Video recordings of cats with DJD are included in the online version of this article at doi:10.1016/j.jfms.2010.01.003
Video 1 shows how an older cat with DJD may change its strategy for reaching a kitchen counter top because of a reduction in the height it can jump.
Video 2 shows a senior (12-year-old) cat, with radiographic changes in both hip joints, exhibiting an array of behaviors suggestive of DJD (eg, stiff gait, reluctance to sit).
Video 3 shows the stiff gait of cat with bilateral elbow, stifle and hip DJD.
In order to guide owners in assessing their cat's mobility, we need to know what activities are altered by DJD-associated pain. A study of 28 cats with osteoarthritis showed that overt lameness was not the most common clinical feature. 5 Instead, features like jumping up, jumping down, height of the jump, general movement, ‘grumpiness’ on handling and seeking seclusion were found to better indicate mobility impairment due to DJD-associated pain. 5

Another study used an objective measure of activity — an accelerometer — and concluded that owners do know when their cat is more, or less, mobile. 6 In this study, owners were asked to pick the activities they felt were impaired as a result of the DJD. Of those they selected, the ones that showed an improvement when an NSAID was administered compared with a placebo were:
Jumping up/down;
Playing (toys, cats);
Running (to food, from dog);
Lying down;
Moving up stairs;
Walking;
Sharpening claws;
Grooming;
Using the litter tray;
Hunting.
Owner-assessed activity impairment
Activities that owners considered to be significantly impaired in cats with DJD, compared with cats without DJD, 19 are shown on the right. These activities can be graded or scored by owners to determine the level of mobility impairment and to monitor the efficacy of treatment. These activities have not been validated as being appropriate activities to assess, although work is ongoing to evaluate these activities, as well as some other activities and behaviors considered possibly indicative of DJD-associated pain.
Walking
Running
Ability to jump up
Ability to jump down
Climbing stairs
Descending stairs
Playing with other pets
Rising from a resting position
Chasing objects
Ability to stretch
Eating
Seeking seclusion
Height of jumping up
Height of jumping down
Sleeping
Playing with toys
More recent work by the same research group has shed further light on activities that may be appropriate to ask owners about when assessing DJD pain in cats (see box above). 19
Performance tests
DJD-associated pain results in impaired mobility, which can be evaluated through performance tests. While these can be challenging to conduct in the clinic with untrained cats, some simple tests are to:
Place the cat down and allow it to move across the room;
Encourage jumping off a chair;
Encourage jumping up to get into a carrier.
Evaluating how the cat performs such tasks can, in some cases, give valuable information as to where the impairment is. For example, cats are generally very willing to jump off an examination table. When they are reluctant to do so, this may be due to painful joints, especially fore limb joints. A cat with painful elbows, say, may be very reluctant to jump down, resisting all attempts to encourage this. When it does jump, it may land very harshly, bringing its hind limbs to the ground very quickly, or landing simultaneously on its fore limbs, chest and hind limbs.
The authors do not suggest forcing a cat to do any particular activity if it is reluctant to, but such observations can provide useful clues as to the impaired area.
Multimedia
Orthopedic examination
Guidelines on how to perform a productive orthopedic examination are scarce for the dog, and virtually non-existent for the cat. A few pointers for optimizing the clinical examination process are given in the sister article on long-term pain. For an orthopedic examination specifically, it is important to include every joint and the whole axial skeleton. In fractious cats, begin by examining the areas suspected to be affected.
Radiography
Orthogonal views of painful joints should be obtained. However, if radiographic signs consistent with DJD are not seen, DJD should not be ruled out. As discussed earlier, there appears to be only moderate overlap between the joints that appear painful clinically, and those that have radiographic signs of degenerative disease. At the moment the reasons for this are unclear, but the mismatch between clinical signs and radiographic features is well recognised in other species.
There are many methods for sedating cats for radiography, and clinicians should use the drugs and combinations they are most familiar with. The authors most commonly use a sedative cocktail of 5 mg/kg ketamine (maximum of 20 mg), 0.5 mg/kg butorphanol and 10 μg/kg dexmedetomidine. This is dosed on lean body weight, and administered intramuscularly. These doses are altered on an individual basis as determined through a physical examination and evaluation of blood work when available. This combination will provide approximately 45 mins of good sedation. In cats with clinically detectable cardiac disease, a combination of opioid and acepromazine is used.
Goniometry
The reliability and reproducibility of goniometry has been well documented in human and canine patients.20–25 This clinical modality is frequently used by orthopedic surgeons and physical rehabilitation clinicians in human and veterinary medicine to evaluate the severity of joint injuries and to monitor the progression of joint disease and the response to treatment.26–28 In dogs, goniometry has been used to assess several joints. It appears to be a valid tool in the cat, 29 but only one study has used goniometry in this species, probably because of the difficulty of defining pain reactions in cats. 30
No studies have yet evaluated goniometry as a tool for assessing joint pain-free range of motion (ROM). Nonetheless, the normal ranges of joint motion in the cat have been defined, 29 and there is unpublished data from one of the authors BDXL) to indicate that decreased ROM is significantly associated with radiographic evidence of DJD.
Do cats with musculoskeletal pain need to be treated?
Treating pain associated with feline DJD
Evaluating mobility impairment and assessing the efficacy of treatment
To evaluate the level of impairment, and to assess whether or not treatment is having a positive effect, a validated form of assessment is needed. As discussed earlier, progress has been made in canine medicine by using the owners as assessors. As yet, there is no validated scoring system or owner-completed questionnaire available for cats. Dr Javier Benito is currently working in Lascelles' laboratory further developing and testing an instrument (questionnaire) for owners of cats with DJD-associated pain. The only placebo-controlled, blinded, cross-over study that has looked at owner questionnaires used a ‘client-specific outcome measures’ (CSOM) questionnaire (briefly described on page 7). 6 Although this has not been evaluated to determine if it is a valid approach, it did seem to distinguish between placebo and NSAID treatments.
Environmental and activity modulation
There is little information on what a preferred environment is for cats, but it is generally accepted that access to height is important. Cats appear to like to rest on beds, sofas and window ledges, and so the ability to access these areas is likely to be important. Owners can modify the environment by moving furniture to provide ‘stepped’ access to any beds, sofas, window ledges, etc, that their cat likes to get to (Fig 5). Additionally, access to food and water should be considered in mobility-impaired cats.
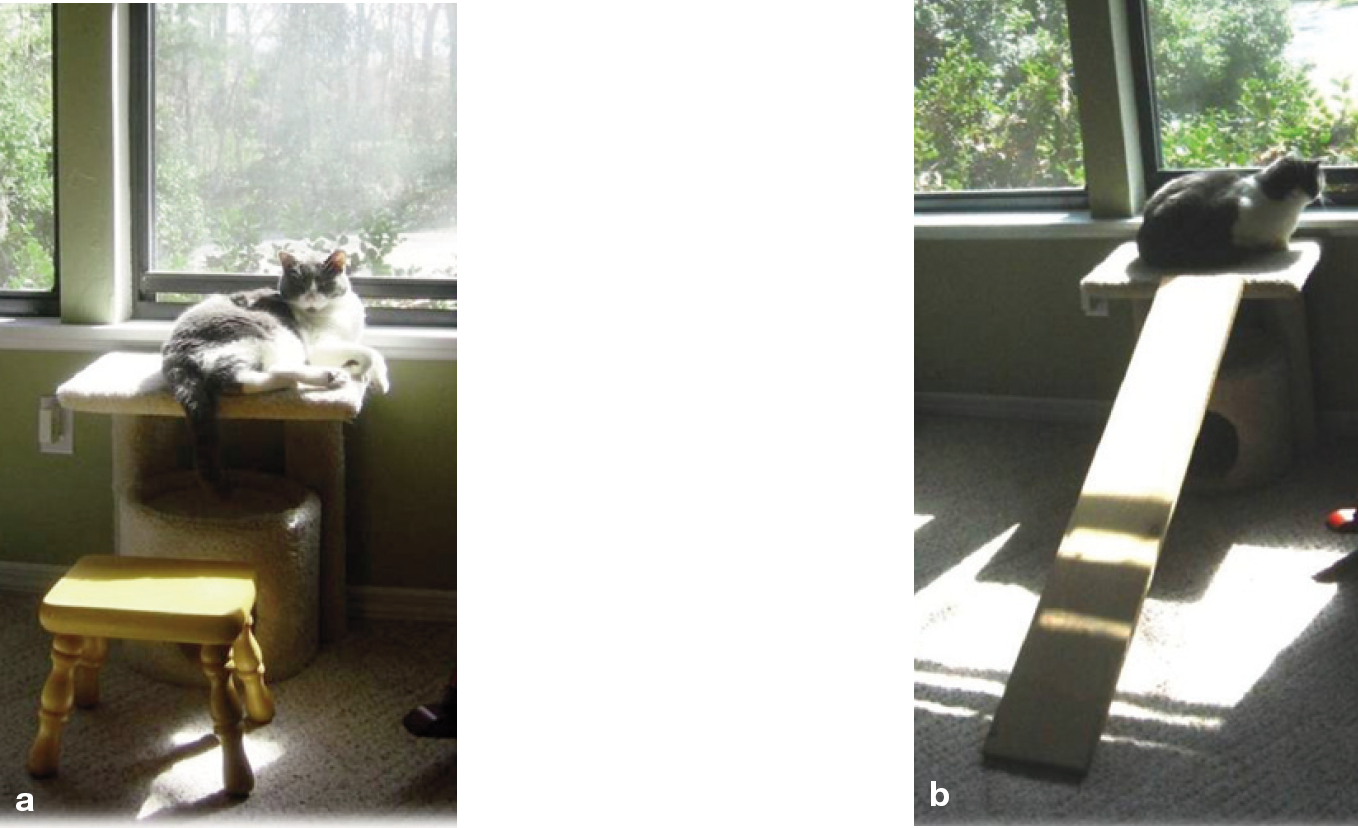
Access to favorite resting places can be made easier by providing ‘steps’ (a) or a ramp (b)
For indoor cats, access to litter boxes should be made as easy as possible (Fig 6). A more complex environment, with facilitated access to various areas and levels, is also likely to encourage more movement, which is known in other species to be important for maintaining muscle mass and tone, and minimizing pain associated with joint disease. Other methods to encourage movement are cat towers, toys, and hiding food and cat-nip to encourage foraging, hunting and playing behavior. Regular periods of gentle play stimulated with the use of toys, feathers and laser-pointers will also help increase exercise in these cats.

Access to litter boxes should be made as easy as possible for cats with impaired mobility Not every cat needs to be turned into an agile and active 6-month-old kitten! Discussions with the owner will determine how much of an improvement is needed, and this can be balanced against the cost and complexity of treatment.
Drug therapy
Table 1 lists drug information and suggested doses that may be useful in managing long-term pain in cats. It should be noted that the majority of these drugs are being used ‘off label’. There is ongoing work in this area, and the recommendations may well change as we gain information about efficacy and toxicity.
Suggested doses of analgesics for the alleviation of chronic pain, including DJD-associated pain, in the cat (continued on page 209)
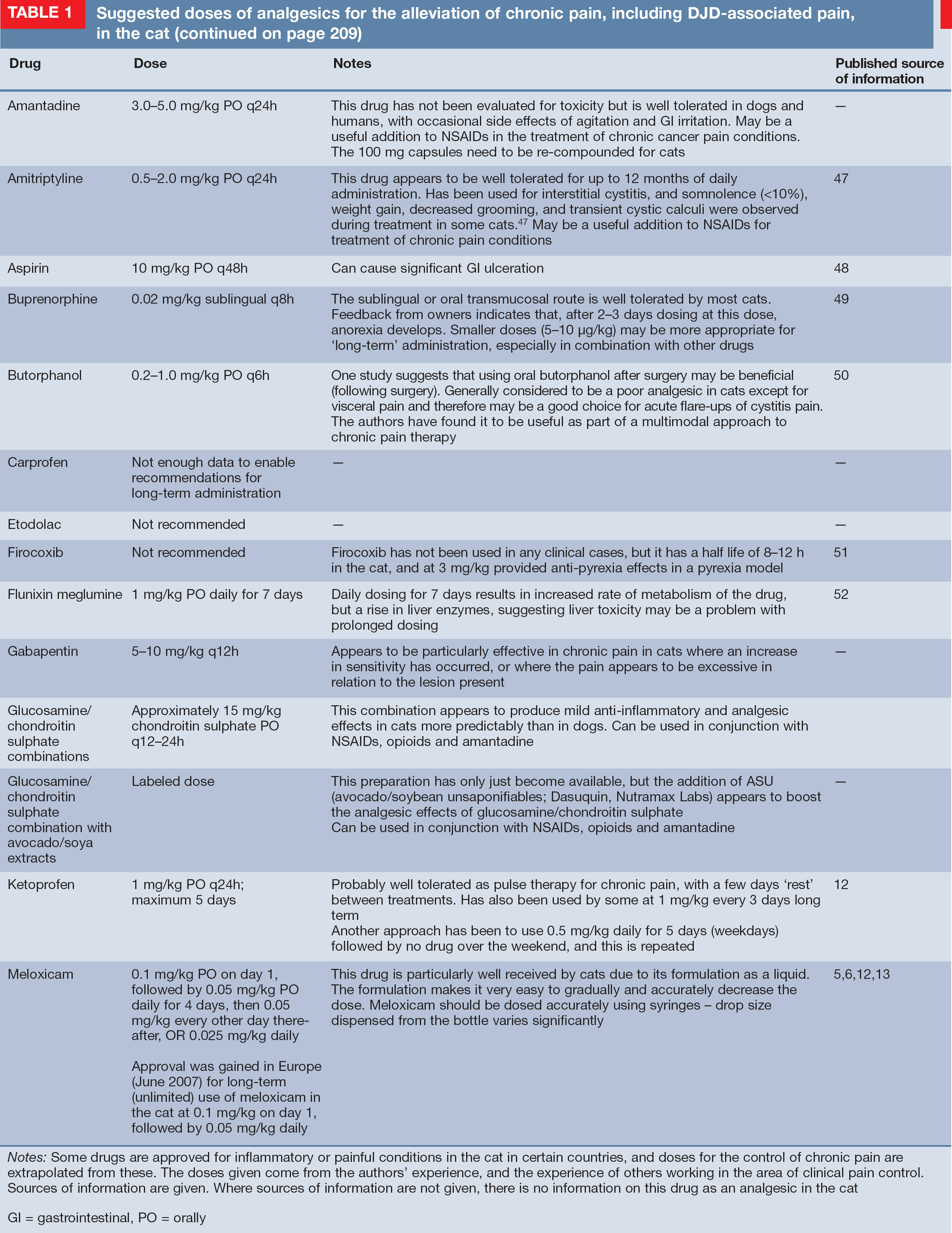

Notes: Some drugs are approved for inflammatory or painful conditions in the cat in certain countries, and doses for the control of chronic pain are extrapolated from these. The doses given come from the authors' experience, and the experience of others working in the area of clinical pain control. Sources of information are given. Where sources of information are not given, there is no information on this drug as an analgesic in the cat
PO = orally, SC = subcutaneously, PCV = packed cell volume, GI = gastrointestinal
At the present time, there is only published or presented evidence for NSAIDs having a beneficial effect (pain alleviating and mobility enhancing) in painful feline non-immune-mediated DJD.5,6,12 The level of evidence for a pain-alleviating effect of treatments varies from objective measures in clinical cases, 6 to open-label studies with non-validated subjective assessments in clinical cases.5,12 The use of NSAIDs in cats has been comprehensively reviewed. 31 Pertinent developments in the 3 years since that publication are the approval in Europe and other countries including Australia of meloxicam to treat chronic musculoskeletal pain. The approval is for an unlimited time at a dose of 0.05 mg/kg. An evaluation of 40 cats with DJD-associated pain suggested that a dose of 0.01–0.03 mg/kg once daily, with a mean treatment duration of 5.8 months, was well tolerated. 13 Gastrointestinal upset in 4% of cats was the only adverse effect noted. An additional development is that the first coxib class of NSAIDs, robenacoxib,32–34 has been granted approval in Europe for use in cats. In cats with musculoskeletal pain the indication is for up to 6 days therapy, at a dose of 1 mg/kg once daily.
Use of a ‘client-specific outcome measures’ scoring system for cats
The activities that are impaired as a result of DJD-associated pain are discussed with the owner (using the activities outlined earlier in this article to guide the owner and discussions).
The activities that appear to be most relevant to the owner and their pet, and appear to be most easily assessed, are written down. Three to five activities (that are frequently seen by the owner) are defined. The time and place where each activity is observed by the owner are noted down.
Finally, the activities, including the time and place (eg, jumping onto the kitchen counter in the morning at feeding time), are recorded on the CSOM form, and the owner makes an assessment of how impaired each activity is by checking the appropriate box. Some owners prefer to grade the impairment based on a comparison with when their cat was not showing these signs; others prefer to compare the impairment with how they would expect a normal cat to be. It probably does not matter which way it is done, as long as a consistent approach is used in follow-up evaluations. A numerical value can be assigned to each activity (scoring ‘normal’ as 0, through to ‘impossible’ as 4) and a total CSOM score is determined. Then, at intervals during treatment, the same questions are asked of the owner, and the assessment scoring system completed. With improvement, the ‘check marks’ should be seen to move to the left ––- that is, the total CSOM score should decrease. At this point, it is important for the clinician to guide the owner as to how much of an improvement it is necessary or appropriate to aim for. The principles of goal attainment scaling of treatment (ie, the scaling of treatment to allow defined goals to be reached) come into play here ––- not every cat needs to be turned into an agile and active 6––month-old kitten! Discussions with the owner will determine how much of an improvement is needed, and this can be balanced against the costs and complexity of treatment.

A discussion of other drug classes can be found in the accompanying article on long-term pain.
Physical therapy
The benefit of physical therapy is just beginning to be defined in canine medicine, but has not yet been evaluated in feline medicine. However, it is likely the same basic principles and benefits will apply to feline patients. ROM and massage techniques can be taught to owners and these can help to alleviate muscle pain and also contribute to ‘environmental enrichment’ for the cat — through more interaction between the owner and cat. Similar to massage and ROM exercises, other modalities such as shock wave therapy, laser therapy, and heat and cold therapy may well be of benefit in certain circumstances in feline patients, but no well controlled scientific studies in cats have been published, and it is not known under which circumstances these therapies will be most useful.
Surgery
There have not yet been any published reports of total joint replacement in the cat (although several total hip replacements have been performed), and only sporadic reports of joint arthrodesis,35,36 with just one of these reporting the procedure for painful DJD. 36 There is one report of arthroscopic removal of osteochondral fragments from the elbow of a cat with DJD, which was suspected to have been caused by a fragmented coronoid process; 37 following arthroscopic surgery, the lameness resolved on subjective assessment. There are also a few reports of clinical signs of pain associated with lumbosacral DJD being abolished following surgical decompressive surgery.38,39
Stem cell therapy
There is an interest in ‘regenerative’ medicine for managing degenerative diseases such as DJD and also for poor or slow healing associated with some wounds or tendon injuries. One approach is to utilize autologous adult stem cells, which can differentiate into several tissue types and also supply trophic factors. Currently, autologous adipose-derived mesenchymal stem cell (AD-MSC) therapy is available to veterinarians in the United States (Vet-Stem, Poway, CA, USA) and in small animal practice has been used primarily for the treatment of osteoarthritis. Briefly, under anesthesia, adipose tissue is surgically harvested and sent for processing. Several days later, the stem cells are injected into the affected joints, although intravenous injection is also reported.
To date, two small studies in dogs affected with coxofemoral or elbow osteoarthritis have shown positive outcomes in some of the chosen outcome measures.40,41 The cellular basis of these improvements is unknown; however, it is unlikely to be ‘regeneration’ of joint tissues, although many people would wish it so! Although this treatment modality has been used in cats with osteoarthritis, with anecdotal reports of improvement, there are currently no published studies. With the costs for anesthesia, harvesting, processing and injection, this treatment is expensive (approximately $3000US, SG2200, £1900).
Dietary modulation
No studies of dietary modulation for feline osteoarthritis have yet been published, but diets containing high levels of the omega-3 fish oil, especially docosahexaenoic acid (DHA) and eicosapentaenoic acid (EPA), are likely to be beneficial. There are two aspects to the potential benefit of dietary modulation for DJD. One is the effect on the disease process itself, and the other is the pain-relieving effects. In dogs, unpublished data using an in vitro model has shown that EPA can reduce damage to cartilage and so can slow down progression of the disease by reducing the production and activity of one of the main enzymes (aggrecanase) involved in breaking down cartilage. Other studies in dogs have shown the benefit of fish oil in decreasing matrix metalloproteinases in naturally occurring stifle joint disease, 42 and the benefits of caloric restriction on the development of DJD in the hip, shoulder and elbow.43–45 One study has suggested a beneficial effect of a diet high in EPA and DHA on some postulated serum markers of joint disease in arthritic cats. 46
There are no published studies investigating the pain-relieving effects of ‘DJD diets’ in cats. However, one of the authors (BDXL) has recently completed a study evaluating a DJD diet (formulated by Royal Canin) containing high levels of DHA and EPA, together with chondroitin sulphate and glucosamine hydrochloride, and green-lipped mussel extract. The study was a placebo-controlled blinded study, and although the primary subjective outcome measures all indicated that both groups significantly improved by day 70, the primary objective outcome measures (activity monitoring) indicated that activity significantly decreased in the group fed the control diet and significantly increased in the group fed the DJD diet. Much work is still to be done in this area, but dietary modulation may be an effective means of treating DJD-associated pain in cats.
Key Points
Currently, a diagnosis of painful DJD should be based primarily on owner-assessed activity impairment, supported by painful joints on examination that have, or do not have, radiographic signs of DJD.
Radiography should be performed in all cases, and an appropriate minimum database obtained prior to initiating treatment.
Cats should be appropriately screened for other diseases that may be impairing mobility such as diabetes and neurological problems.
Treatment plans should make the most of non-drug therapy and incorporate drug therapy as appropriate.
Treatment should be followed up for efficacy and toxicity, and the cat continually re-evaluated for the need for multiple treatments.
Veterinarians should be aware that treatment recommendations may well change as we find out more about this disease and the most effective way to alleviate the pain.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.