
Abstract

Introduction
Brachycephalic cats such as Persian or Exotic shorthairs enjoy great popularity. This is perhaps not surprising; the head of these animals shows child-like characteristics and most people are instinctively attracted by this. An infant's face with full curves is associated with purity, sincerity, honesty and vulnerability. This immediately provokes a protective instinct in us. 1 The skull of brachycephalic cats is characterised by a round shape, which is attributed to a reduction in the length of the face and brain case. 2 Brachycephalic heads show various additional characteristics of young animals. 3
As a result of the head conformation, there is a high prevalence of associated disease. Both brachycephalic airway obstruction syndrome and chronic epiphora are potentially of clinical significance.4–8
Reasons for epiphora might be insufficient drainage of the excretory nasolacrimal system, stenosis of the proximal drainage system or nasolacrimal duct, congenital atresia of the lacrimal puncta as a genetic or spontaneous anomaly, aplasia of the nasolacrimal duct, atresia of the nasolacrimal drainage system (NDS), or an undersized lacrimal sac.7–9 Epiphora might also develop if masses obstruct the drainage, or hairs and entropion irritate the cornea. 5
In human medicine, investigation of the NDS using computed tomography (CT), either with or without contrast medium, plays an important role in the investigation of chronic epiphora, facial trauma and swellings of the periorbita; as well as in estimating the dimension of tumours, and evaluating surgical approaches in this region.10–13
Diagnostic evaluation of the NDS is occasionally required in veterinary medicine.5,8 While CT and MRI are the imaging modalities of choice in human medicine for this region, most veterinarians still rely on conventional radiography,6,8,14,15 which has been used for the diagnosis of stenosis, ectasia, atresia, fistula, inflammation, obstructions, agenesis of the lacrimal ducts, constrictions and tumours.8,14 To the authors' knowledge, CT examination of the brachycephalic feline NDS has not been described to date.
Overt differences in brachycephalic cats compared with normal (mesocephalic) cats include the missing external nose (Fig 1) and discoloured hairs caused by an overflow of tears (Fig 2). When researching the special anatomical features of brachycephalic heads, only a few descriptions of the NDS were found in the literature.6,16 Investigations using conventional radiography and corrosion casts have reported that the nasolacrimal duct of brachycephalic cats shows a right-angled or even acute-angled course. 6

Radiographs of a mesocephalic cat (a) and a severely brachycephalic cat (Exotic shorthair) (b). Note the length and the tip of the nose and nasal bone, the dorsally rotated hard palate, nasal airways and jaw, the compressed and dislocated conchae, and the elongated and thickened soft palate in the brachycephalic cat

To account for the range in phenotypic appearance, a classification system with four degrees of brachycephalia - from mild (I) to severe (IV) - is recommended. The main features on which this classification is based are the dorsal displacement of the maxillary canine teeth and the dorsorotation of the jaw. Note that drainage discoloration of the skin starts in moderately affected cats; and that the tip of the nose is located at a higher level than the lower eyelid in profound and severe degrees of brachycephalia
The objective of this study was to evaluate the influence of head conformation on the course of the NDS in brachycephalic cats using CT. To create an anatomical basis for clinical evaluation, corrosion casts and three-dimensional (3D) models would be developed using CT-dacryocystography (CT-DCG) datasets. Additionally, it was planned to compare the results with those obtained from mesocephalic domestic cats.
Materials and methods
This study is based on a total of 46 cats (29 euthanased, 17 anaesthetised), which were examined using CT and/or various anatomical techniques. Exclusion criteria were severe nasal disease and a history of skull trauma. Brachycephalic cats showing mild nasal discharge (8/31) were admitted to the study if no destruction of conchal tissue or other structures was detectable using CT. Three different breeds were represented: domestic shorthair cats (15), Persian cats (27) and Exotic shorthair cats (4). Ages ranged from 3 months to 13 years (mean 6 years), and the study population comprised 26 males and 20 females.
To assess specific influences on the course of the NDS, the head conformation of brachycephalic cats (31/46) was compared with that of mesocephalic cats (15/46). Due to the range in phenotypic appearance, all brachycephalic cats were divided into four groups (Fig 2) based on the following criteria:
Alignment of the upper canine teeth and rotation of the jaw;
Development of the facial bones;
Conformation of the ‘stop’ (bend at the junction of the nasal and frontal bone);
Characteristics of the neurocranium.
Both macerated and 3D-reconstructed skulls were assessed. In the case of euthanased cats, which were not used for other anatomical methods, the macerated skulls were classified. In all other cases, 3D reconstructions of the skull were made from the CT datasets.
Categories of brachycephalia

In the background a skull of a domestic cat and a brachycephalic cat (category II, moderate) are illustrated. Superimposed on these is a skull with a severe (category IV) degree of brachycephalia. Note the highly shortened facial skull, and the cumulative effects of this reduction within the area of the nose. There is no nasal bone and reduced maxillary bone, and it would seem impossible for all teeth to be accommodated. The viscerocranium and the mandible are dorsally rotated also, and the canine tooth is almost horizontal in position. The whole lacrimal bone is reduced to a prominent process (processus frontalis of the lacrimal bone). Drawing courtesy of Gisela Jahrmärker
CT examination
Computed tomography examinations were carried out in 37 of 46 cats. A HiSpeed DX/j Plus (General Electric) scanner, an Mx8000 Brilliance multislice spiral CT scanner (Philips Medical Systems, Hamburg, Germany) and a Tomoscan M/EG/Compact (Philips Medical Systems, Hamburg, Germany) were used to acquire the CT images. The cats were positioned symmetrically in sternal recumbency on the scanning table. The beam projection was directed perpendicularly to the hard palate or to the nasal bone. The slice thicknesses depended on the CT scanner and were set to 0.6, 1 or 2 mm, respectively.
To identify the whole course of the NDS, and to mark it out for further 3D reconstructions, CT-DCG was performed after non-contrast CT in five cases. One mesocephalic and four brachycephalic cats were used (one category II [moderate], two category III [profound], one category IV [severe]). Two of these cats were anaesthetised and a 2 ml syringe was filled with a mixture (1:2) of contrast medium (iopentol [Imagopaque; Nycomed Imaging]) and hydroxypropyl methylcellulose solution (Adatocel; Bausch & Lomb Surgical) for ocular application. Using an intravenous catheter (Neocan Medikit 24G, external diameter 0.6 mm, length 19 mm) the mixture was injected into the lower lacrimal punctum and a contrast CT examination followed (using the same settings as for non-contrast CT). The remaining three cats were euthanased and their NDS was infused with silicon rubber and barium sulphate (Micropaque; Wolf & Co, Vienna, Austria), serving as both a casting and contrast medium. These latter investigations were carried out at the Department of Pathobiology (Anatomy), University of Veterinary Medicine in Vienna, using an established method. 6
All CT-DCG datasets were used to build 3D models of the different feline heads employing VGStudio MAX 1.2 software (Volume Graphics, Heidelberg, Germany). Due to differences in the density value of tissue and contrast medium, segmental works were performed on the bones, soft tissue and the NDS.
To create an anatomical basis for clinical evaluation the following methods were employed (Table 1): corrosion casting of the NDS (3/46), maceration (13/46), dissection work (3/46), sheet plastination (6/46) and sheets preserved with polyethylene glycol (5/46). In all corrosion casts the NDSs were milled according to the 3D model. The preparatory works, as well as the CT and CT-DCG images obtained, were evaluated to determine anatomical landmarks of the NDS within the nose and the surrounding structures.
Summary of methods employed in the 46 cats
Results
Concomitant with an increased degree of brachycephalia, the facial and neurocranial bones were shortened, the cumulative effects of this reduction being seen within the area of the nose (Fig 1). With respect to the jaw, a dorsal displacement (so-called dorsorotation) was obvious. In particular, the os maxillare, os incisivum, os nasale, os conchae nasalis ventralis (Fig 4), os palatinum, os ethmoidale and os mandibulare were dorsally displaced. The main criterion distinguishing a dorsally rotated jaw (and thus used for the classification of brachycephalia) was the alignment of the upper canine teeth. Whereas in mild degrees of brachycephalia the upper canine teeth were nearly vertical, in severe degrees of brachycephalia these teeth showed a rotation to an almost horizontal position (Figs 2 and 3, Table 2).

The ventral nasal bone (VNB) of a mesocephalic cat (left) and brachycephalic cat (category II, moderate) (right) is displayed from a dorsomedial view; the conchae ethmoidales and nasal septum have been removed. The maxillary canine tooth markedly influences the course of the nasolacrimal drainage (marked in red). Compared with mesocephalic cats, the VNB in brachycephalic cats is dorsally rotated (mobile point). The drainage streams adjacent to the basal lamina of the ventral nasal bone (1) and is therefore also characterised by an increased angle and a steeper course
Relationship between the rotation of the maxillary canine teeth, the nasodrainage system and the severity of brachycephalia
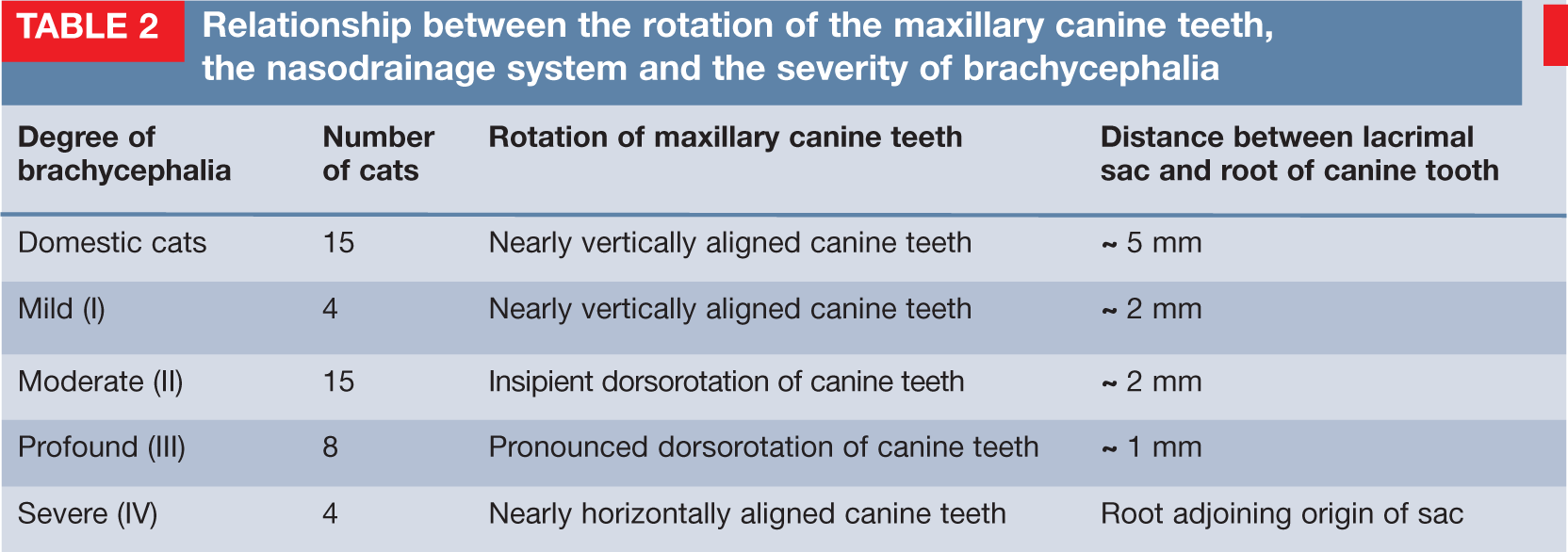
All four Exotic shorthair cats were classified in the severe category (IV) of brachycephalia. Persians showed mild (4/31), moderate (15/31) and profound (8/31) degrees. The higher the degree of brachycephalia and dorsorotation, the narrower the nasal cavity, nasal airways and nares. Associated with these observations were a displacement of the ethmoidal bone (including the conchae ethmoidales) and dorsorotation of the ventral nasal concha. The increased upright position of the ventral nasal concha led to a steeper course of the respiratory meatus (meatus nasi ventralis) and nasolacrimal duct (Fig 4).
NDS of mesocephalic cats
The NDS of mesocephalic cats started with a descending portion (upper and lower lacrimal canaliculi and lacrimal sac) and continued in a horizontal portion (nasolacrimal duct, see Fig 9). This horizontal part was situated parallel to the hard palate and was directly influenced by the ventral nasal concha and the canine tooth. In mesocephalic cats the distance from the lacrimal sac to the root of the canine tooth was approximately 5 mm. The nasolacrimal duct passed medially into the nasal cavity within this 5 mm gap.
NDS of brachycephalic cats
With increasing degrees of brachycephalia, the entire NDS became shorter and steeper, and the distance from the root of the canine tooth to the lacrimal sac decreased (Table 2). In cats in the mild and moderate groups, that distance was reduced to approximately 2 mm (Fig 5). Profoundly brachycephalic cats showed a distance of approximately 1 mm.
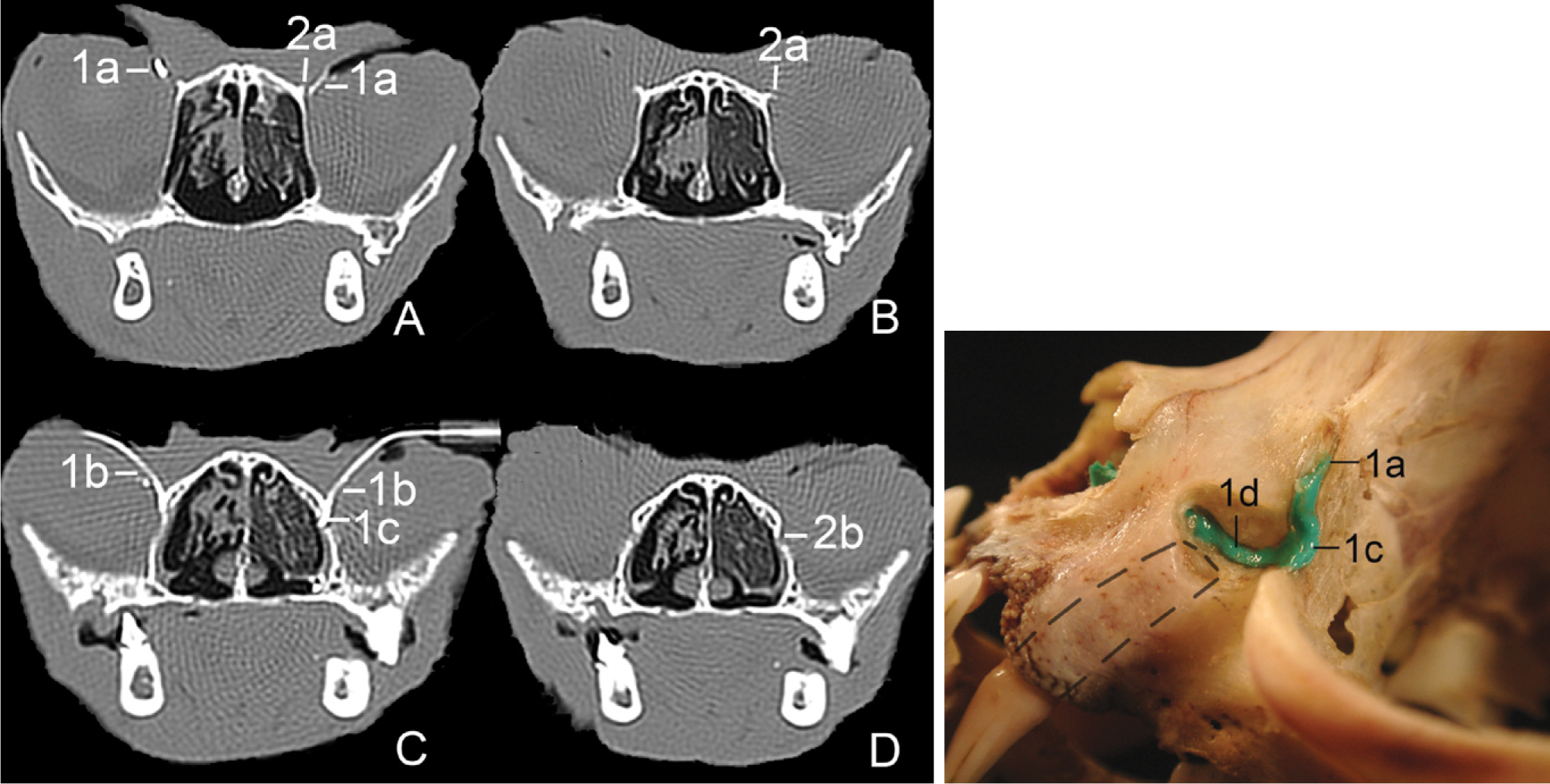
Comparison of transverse contrast CT images (A and C) and transverse non-contrast CT images (B and D) of moderate (category II) brachycephalia. The cast within the skull of this cat displays the course of the NDS and its topographic location compared with the canine tooth. The distance between the root of the tooth (indicated by the dashed line) and the nasolacrimal sac is 2 mm. Lateral to the processus frontalis of the lacrimal bone (2a) is the upper lacrimal canaliculus (1a). 1b = lower lacrimal canaliculus, 1c = lacrimal sac, 2b = fossa sacci lacrimalis, 1d = nasolacrimal duct
In severe stages of brachycephalia, the canine teeth were displaced in a horizontal position and the roots adjoined the nasolacrimal sac.
This hindered the direct passage of the nasolacrimal duct from its origin to the nasal cavity. Rather, the nasolacrimal duct was forced to pass below the canine teeth (Fig 6) to drain into the nose, adopting a V-shaped course (Figs 6 and 8) in the process. Furthermore, in profound and severe degrees of brachycephalia the tip of the nose, and therefore the nasolacrimal ostium, was higher than the level of the lower lacrimal punctum.

Comparison of a transverse contrast CT image (left) and a transverse non-contrast CT image (right) of severe (category IV) brachycephalia. To drain from the lacrimal sac (1c) into the nose, the nasolacrimal duct (1d) is forced to pass below the root of the canine tooth (c). The root of the canine tooth (indicated by a dashed line) is situated directly adjoining the nasolacrimal sac (1c). Note the prominent frontal process of the lacrimal bone in the left-hand image (2a). The cast within the skull of this cat is hidden by the canine tooth root
Anatomical landmarks on CT and CT-DCG image analysis
On examination of the CT images, osseous structures delimiting the NDS were easily recognisable. For specific detection of the NDS without contrast medium the following anatomical landmarks were useful (Fig 5): the processus frontalis of the lacrimal bone (situated close to the upper lacrimal canaliculus), the fossa sacci lacrimalis (containing the lacrimal sac), the basal lamellae of the ventral nasal bone (bordering part of the nasolacrimal duct) and the basal fold (containing the third part of the nasolacrimal duct).
On analysis of the CT-DCG images, the upper lacrimal canaliculus was identifiable lateral to the processus frontalis of the lacrimal bone (Fig 5). In brachycephalic cats an increased frontal process of the lacrimal bone was visible (Fig 6). In cats with profound and severe brachycephalia the upper lacrimal canaliculus was not detectable.
The lower lacrimal canaliculus showed huge differences between normal and brachycephalic breeds in terms of its position relative to the canine tooth (Figs 7 and 8). With severe degrees of brachycephalia both canaliculi were located rostral to the origin of the nasolacrimal duct and at the same level as the root of the canine tooth (Fig 8).
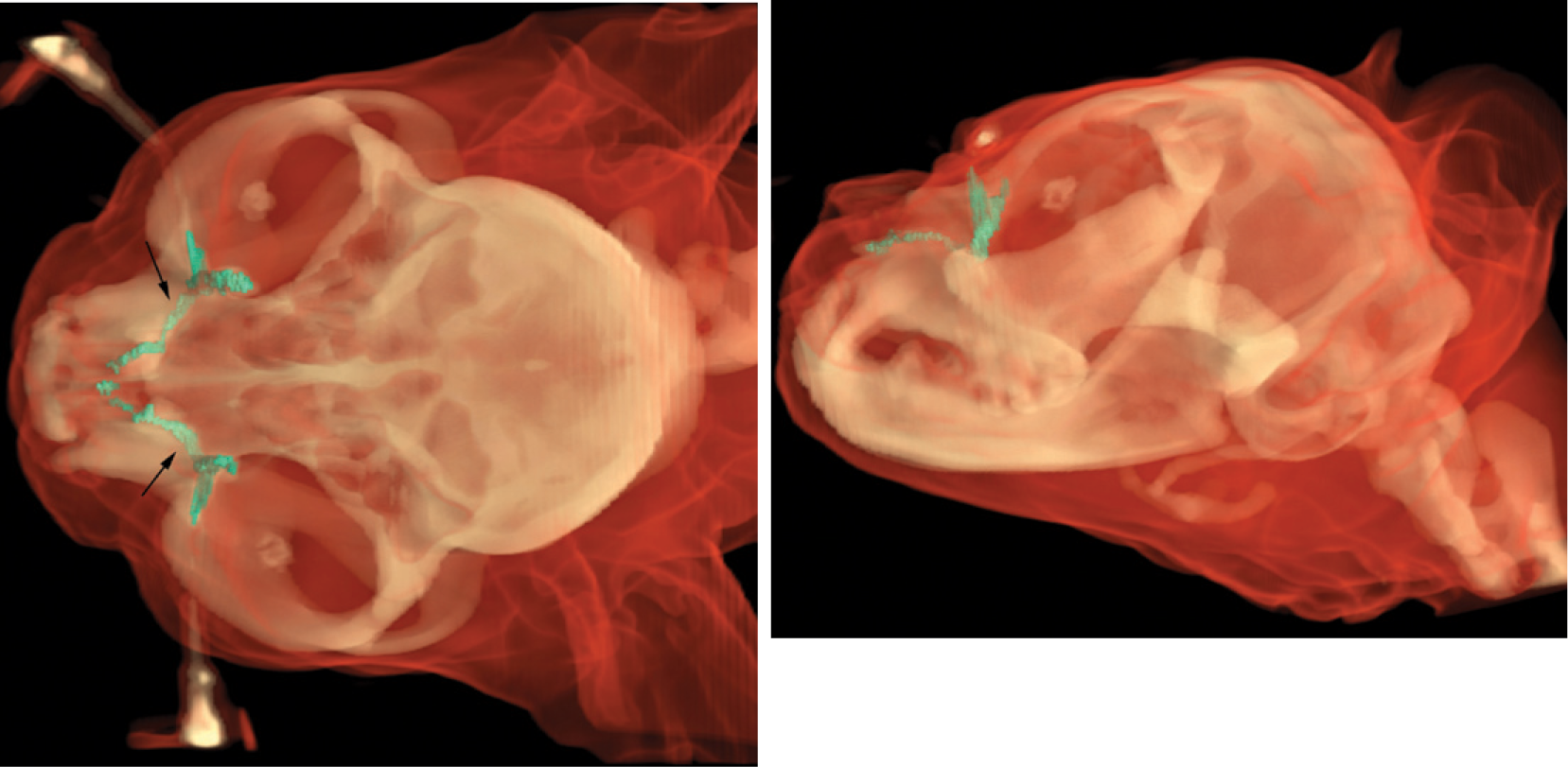
Three-dimensional models of the NDS in moderate brachycephalia; dorsoventral and laterolateral views. An acute angle and caudal-to-rostral course is visible. Arrows mark the position of the canine teeth

Three-dimensional models of the NDS in severe brachycephalia demonstrate the V-shaped course and reveal what is occult in the cast. Arrows mark the location of the canine teeth
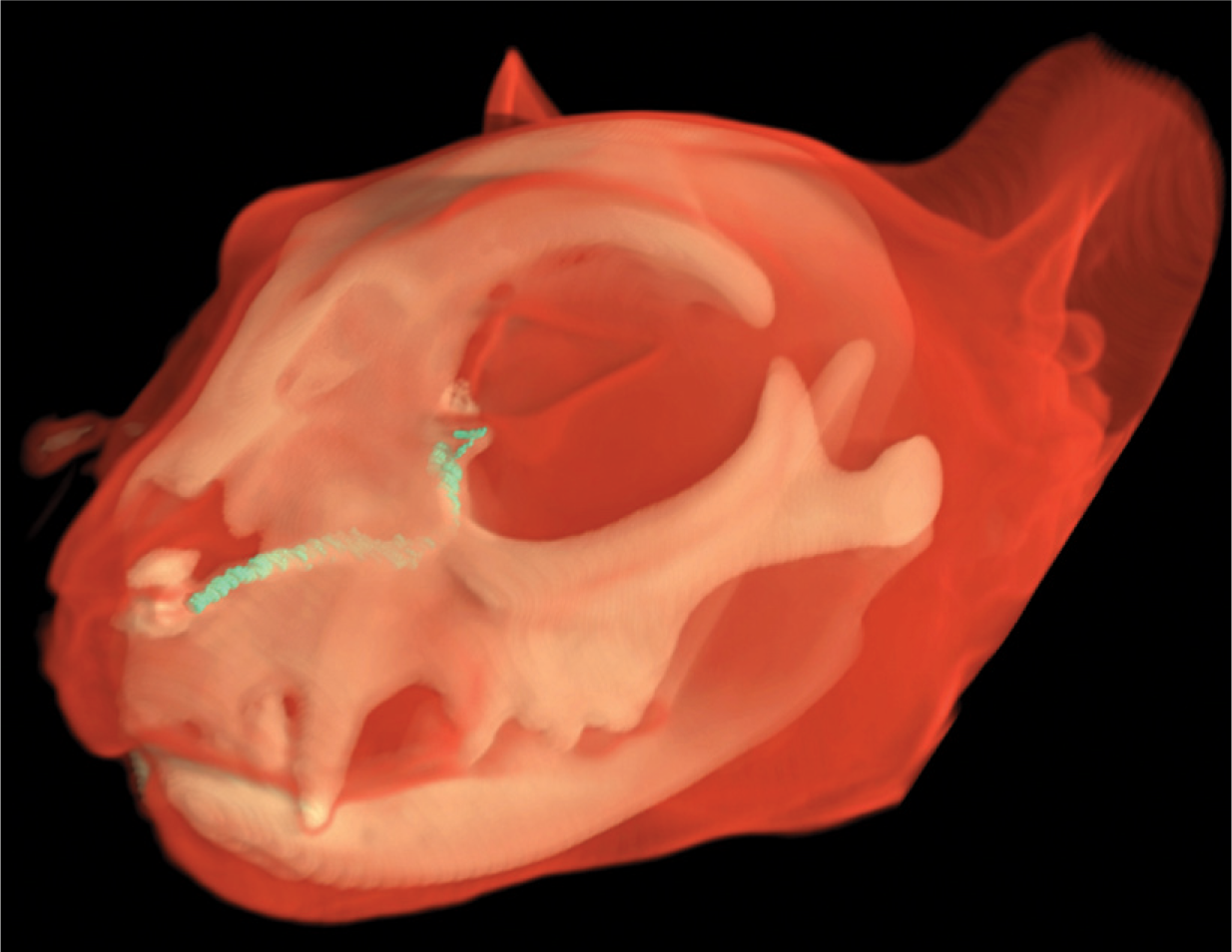
Three-dimensional model of a mesocephalic cat. Note the course of the nasolacrimal duct, which runs parallel to the hard palate and shows a right-angled alignment
Similar to mesocephalic cats, in brachycephalic cats the origin of the lacrimal sac was located at the level of the maxillary foramen of the infraorbital canal. The bony fossa sacci lacrimalis contained the lacrimal sac and was a suitable anatomical landmark for identifying the saccus in mesocephalic, mildly brachycephalic and moderately brachycephalic cats (Fig 5). With profound and severe degrees of brachycephalia, identification of this bony structure was not possible (Fig 6). As the degree of brachycephalia increased, the distance between the root of the canine teeth and the lacrimal sac reduced (Figs 5 and 6).
With increasing brachycephalia, the nasolacrimal duct decreased in length (Figs 7 and 8) and was more difficult to identify. The three different parts of the duct corresponded to those in the mesocephalic cat. The origin was located at the same transverse level as the maxillary third premolar or fourth premolar, respectively. As in mesocephalic cats, the middle part of the nasolacrimal duct was situated ventral to the basal lamina of the ventral nasal concha. But the os conchae nasalis ventralis showed a dorsal displacement in brachycephalic cats, which influenced the course (Fig 4).
Discussion
To evaluate head conformation and its influence on the NDS, CT, CT-DCG, 3D models, corrosion casts and other anatomical techniques were used. The most important finding was that the NDS is forced to pass below the canine tooth and follows a V-shaped course if the nose is missing (ie, in the severe category of brachycephalia).
A rather acute-angled alignment of the nasolacrimal duct in brachycephalic cats was first recorded in the literature in 2003. Associated with this finding, a steeper alignment and attachment of the ventral nasal concha could be observed. In more severe cases, the main part of the duct ascended beyond the level of the lacrimal foramen. 6 These observations were confirmed in the present study, but no description of the nasolacrimal duct passing to the nasal cavity ventral to a horizontally positioned canine tooth could be found.
In its embryological development, the nasolacrimal duct evolves from the ectodermal nasolacrimal sulcus at an early stage, prior to tooth development.17–19 From this it can be presumed that the development of the canine tooth influences the already existing nasolacrimal duct and its course. Consequently, the NDS takes a V-shaped course in cats with higher degrees of brachycephalia. The steeper course forces the lacrimal fluid to drain dorsally. Such hindrance to the drainage might result in epiphora, a prominent and frequent sign in brachycephalic cats. The proximity of the NDS to the canine tooth may also lead to problems arising as a result of tooth extractions; complications in the cat - principally oronasal fistula - are most commonly associated with the canine tooth.8,20,21 Obstructions of the NDS in cats caused by dental roots are also mentioned in the literature. 5
Feline skull morphometry confirmed that brachycephalic skulls are quite heterogeneous. Thus, two tendencies - extreme forms and forms that are similar to mesocephalic cats-based on the proportions of the brain case are reported. 2 While these tendencies are confirmed by this study, they seem inadequate to describe the spectrum of changes observed. In dogs, measurements of the skull have revealed significant distinctions among three different brachycephalic breeds. 2 This led to four categories being defined on the basis of phenotypic appearance: mild and moderate on the one hand, and profound and severe on the other hand. Possibly the absence of morphometry to confirm the four categories of brachycephalia is one limitation of this study. However, earlier investigations showed that there is an agreement of 95.65% between the assignment on the basis of phenotypic appearance and the predicted group membership. 2
Nevertheless, a classification system in cats seems necessary to adequately describe the skull conformations associated with disease. Problems arise from increased dorsorotation and reduction of the facial bones, and these should be recognised and discussed with breeders, owners and veterinarians worldwide. Cats with profound and severe degrees of brachycephalia seem to be more predisposed to these problems than mild and moderate groups. In Germany, it is prohibited to breed from brachycephalic cats in which the tip of the nose is higher than the level of the lower eyelid, and which show other anomalies of the facial bones. 22 This is the case in profound and severe degrees of brachycephalia. For the purposes of first screening, the rotation of the upper canine teeth seems to provide a useful means of classifying brachycephalic breeds. To establish how the cat's clinical appearance relates to the rotated tooth, further investigations are necessary to identify discriminating parameters.
Dorsorotation of the upper jaw specifically has also been confirmed in another study of brachycephalic animals. 23 Normally this condition, referred to as an inclination between the face and brain case, is only evident in the early embryonic stages and decreases in older developmental stages. 18 This may explain why, in the literature, brachycephalia is also referred to as the ‘preservation of the neonate’. 3
Computed tomography is commonly used for investigating the NDS in humans,10,11,13 and plays an important role in the diagnosis of chronic epiphora,13,24 the obvious presenting sign in brachycephalic cats. In veterinary medicine the application of CT has already been described in mesocephalic cats, 25 dogs,12,24 and horses. 12 Osseous structures belonging to the NDS are easily recognisable in CT images, which are free from superimposition of other parts of the skull. 25 It is, therefore, possible to draw inferences about the course of the proximal and middle part of the nasolacrimal duct, even without contrast enhancement. Contrast-enhanced CT evaluation does, however, offer advantages, allowing accurate localisation of alterations, and rendering detailed information about the shape, diameter, extent and margin of these tubular structures. Methylcellulose mixed with contrast medium is useful for CT-DCG in anaesthetised cats. The higher viscosity of the fluid delays its passage in the nasal cavity and, thereby, detection on CT is improved.
The slice thickness and distance were set to 0.6, 1 or 2 mm, depending on the CT scanner. In other investigations using CT in the region of the feline nasal cavity these settings have varied exceedingly, from 2–10 mm.26–28 However, to adequately identify the tiny structures of the NDS and the inconspicuous osseous surroundings, a high resolution scan with the smallest possible slice thickness is necessary, allowing evaluation and 3D reconstruction. Three-dimensional models are suitable for gaining a better understanding of the complex anatomy of the head. Having created the 3D models it was easy to open the osseous canal (canalis lacrimalis) and to uncover the NDS using a milling cutter.
KEY POINTS
It is useful to classify brachycephalic breeds of cat because of the significant range in phenotypic appearance.
In severe and profound degrees of brachycephalia the drainage function seems to be inefficient.
The acute-angled and sometimes V-shaped course of the NDS is influenced by both the position of the canine tooth and the dorsorotation of the jaw. This hinders the drainage and might result in epiphora.
The authors recommend avoiding breeding from individual cats affected by profound and severe brachycephalia. Preference should be given to cats that show no dorsorotation of the jaw, an inconspicuous stop, and longer facial and neurocranial bones.
Rotation of the upper canine teeth seems to provide a provisional basis on which brachycephalia can be classified, and may be used by breeders and breeding judges for subjective classification and for selection of individuals for breeding.