
Abstract
A synovial cyst of the fifth digit of the left forelimb in a 15-year-old cat was diagnosed. Radiographs showed severe osteoarthritis of the interphalangeal and metacarpophalangeal joints with soft tissue swelling. An ultrasound examination of the digit revealed a cystic structure. Following amputation of the digit, the cyst recurred 3 months later palmar to the carpus and metacarpus. The aetiology of synovial cysts is discussed.
Synovial cysts are a rare occurrence in cats. Of the reported cases, all were localised to the medial aspect of the elbow joint and were associated with degenerative joint disease. 1–3 Synovial cysts of the phalanges have not been described in cats. Synovial cysts have been reported affecting the pulp of the little finger of people. 4 These cysts originate from leakage of synovial fluid from the wrist joint into the flexor synovial sheath in the digit.
A 15-year-old domestic shorthair cat presented with a 3-day history of mild lameness in the left front limb and a cystic swelling palmar to the distal phalanx of the fifth digit. The swelling extended laterally and proximally to the middle of the metacarpal area. Manipulation of the interphalangeal and metacarpophalangeal joints was slightly painful. Radiographs of the distal front limb taken at the time showed a soft tissue swelling around the fifth digit with osteophytosis of the metacarpophalangeal, proximal interphalangeal and distal interphalangeal joints. The cat was treated with a broad-spectrum antibiotic and the swelling decreased over the next 2 weeks. Four weeks later the cat returned with a more pronounced swelling of the fifth digit (Fig 1) and the lameness was more severe. The cat showed signs of pain on manipulation of the fifth digit. Aspiration of the cystic swelling produced a pinkish viscous fluid, which proved to be characteristic of synovial fluid with multiple lymphocytes, large monocytes and macrophages, several neutrophils, and individual epithelial cells with a large nucleus in cytology. A cell count was not performed. During the next 6 months, the cat returned to the practice every 3–4 weeks for aspiration of 2–4 ml of fluid from the swelling to alleviate the pressure. After 7 months, radiographs of the distal left forelimb showed a more extensive large soft tissue swelling, palmar and lateral to the fifth digit extending to the carpus, with osteoarthritic changes of the metacarpophalangeal, proximal interphalangeal and distal interphalangeal joints (Fig 2a). Ultrasonography of the swollen digit revealed multiple almost confluent anechoic spaces with hyperechoic septae. Some echogenic particles were seen within the fluid. The branches of the superficial and deep flexor tendons of the fifth digit were visible within the fluid (Fig 2b).

Soft tissue swelling of the fifth digit of the left front limb.
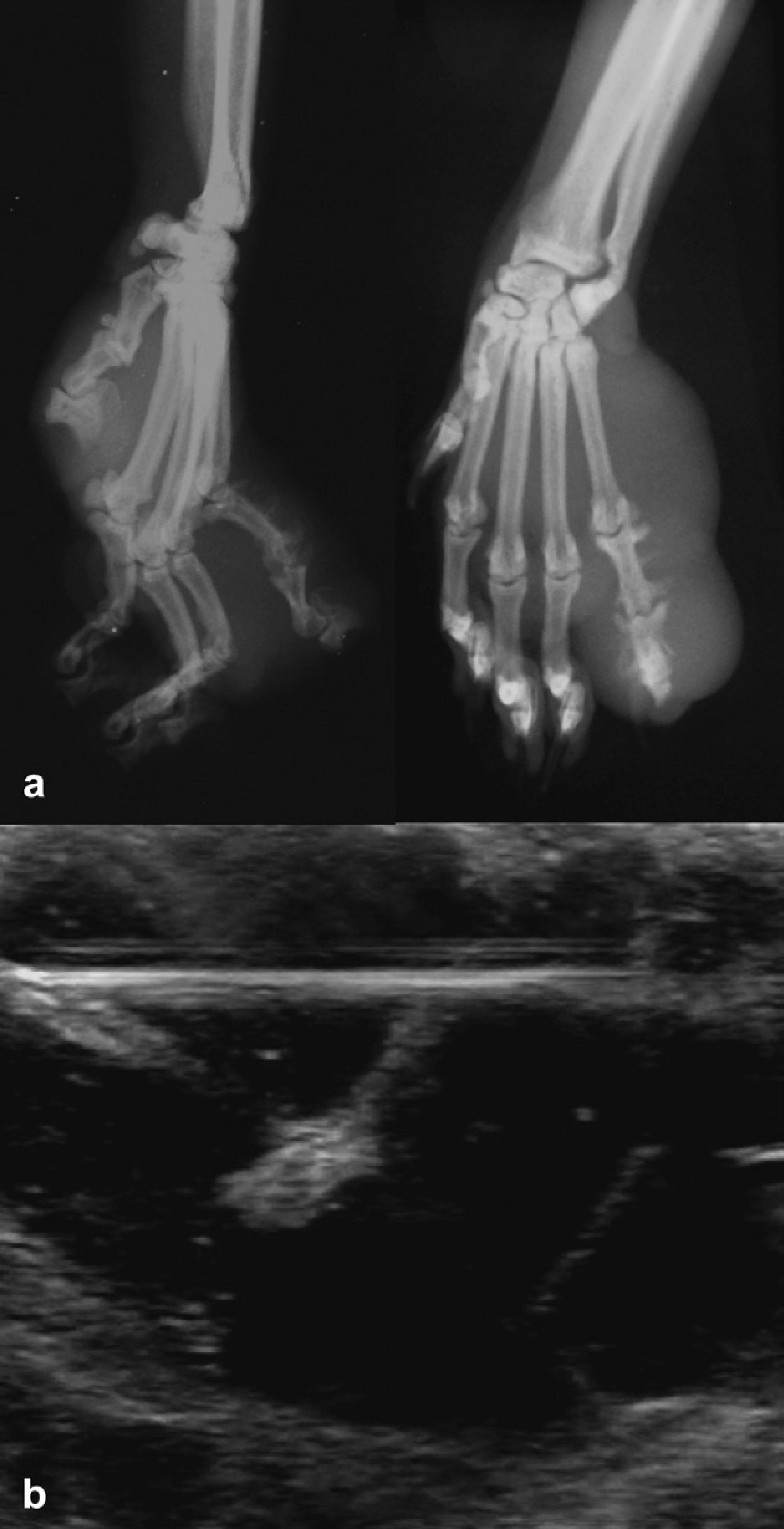
(a) Radiographs of the left carpus, metacarpus, and phalanges showing severe osteoarthritis of the metacarpophalangeal joint as well as the proximal and distal interphalangeal joints with soft tissue swelling. (b) Ultrasound image of the swollen digit with multiple anechoic spaces and hyperechoic septae.
Because the swelling was recurring more frequently with a more pronounced lameness and the osteoarthritis was severe, the fifth digit was amputated through the proximal fifth metacarpal bone. Three weeks later the cat presented with a small swelling at the surgery site, but showed no lameness. After 3 months, a swelling palmar to the carpus and metacarpus appeared which was aspirated. The cat was euthanased 16 months later due to renal failure. Radiographs taken of the cadaver showed marked soft tissue swelling palmar to the metacarpus, extending proximally to the carpus (Fig 3).

Radiographs of the left distal limb 3 months after amputation of the fifth digit. A marked soft tissue swelling is visible palmar to the carpus and metacarpus.
Histological examination of the lesion, which was temporarily frozen, revealed irregular artificially compressed synovial structures lined by collagenous connective tissues (Fig 4). Follicular lymphocytic infiltrates bordered the synovial membrane, which showed focal villous projections into the lumen. The diagnosis was a synovial malformation or sacculation due to chronic joint disease and caused by an overproduction of synovia and/or insufficient reabsorption.
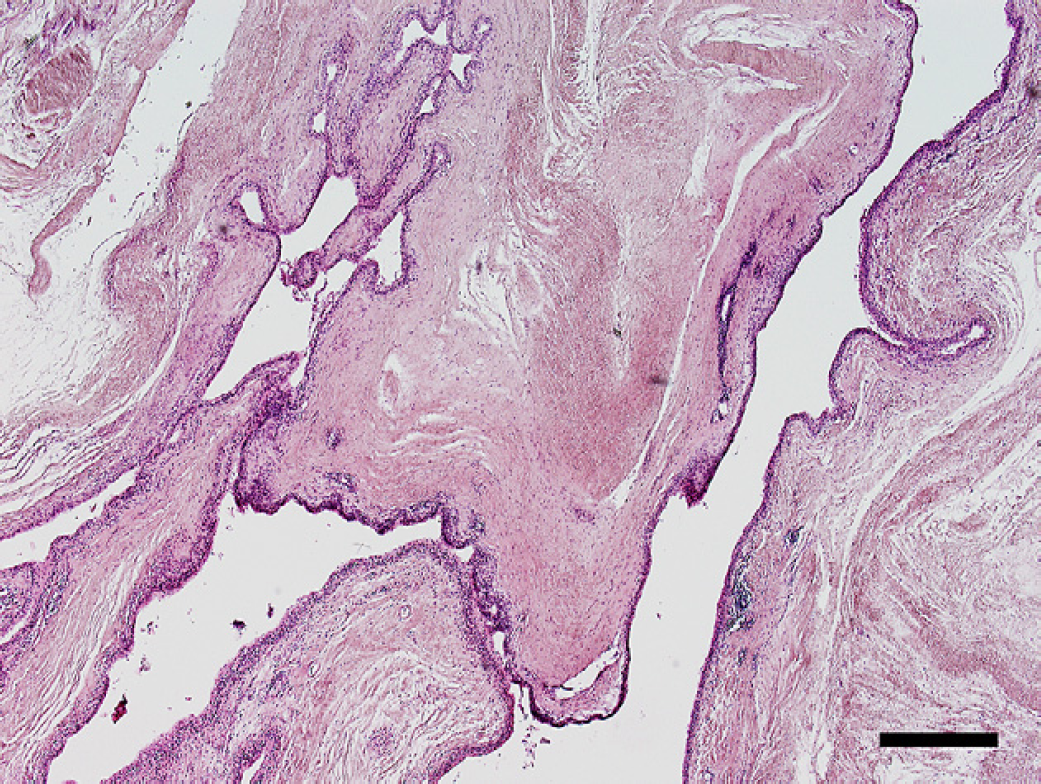
Irregular synovial cavities lined by collagenous connective tissues. Bar represents 250 μm.
The age of the cat is similar to previously described cases. 1–3 All cats were over 10 years of age (range 10–16.5 years).
The location of the synovial cyst in the digit of the presented cat has not been described previously. Most synovial cysts in cats are found medial to the elbow joint and are associated with degenerative joint disease. 1,3 In three dogs reported by Prymak and Goldschmidt, 2 synovial cysts were found at the carpus. Synovial cysts have been reported palmar to the antebrachiocarpal joint in small breed dogs with chronic luxation and arthritis. 5 A case series of three elderly human patients describes synovial cysts in the pulp of the little finger, originating from the wrist joint. 4 The patients suffered from degenerative arthritis of the wrist or a degenerative perforation of the wrist capsule. The synovial cyst was formed from leakage of synovial fluid from the wrist joint into the ulnar bursa, passing distally along the flexor synovial sheath to form a cyst in the little finger pulp by escaping from the distal part of the flexor sheath. It is hypothesised that chronic joint disease stimulated excessive synovial fluid formation, which leads to an elevated intra-articular pressure and subsequent cyst formation. 5
In the present case, the lesion appeared to originate in the fifth digit. In humans, the flexor synovial sheath of the little finger may occasionally extend proximally into the ulnar bursa and flexor tendon sheath infections may spread more proximally than those of other fingers. 6 The cystic swelling was limited to the phalanges with degenerative joint disease present. It is presumed that tenosynovitis of the flexor tendon sheath of the fifth digit developed from interphalangeal and metacarpophalangeal joint disease in the present case. It is not clear whether the synovial cyst was caused by the tenosynovitis and spread to a joint or if the synovial cyst originated from a joint, similar to the cases presented by Wainwright and Burge. 4 Following amputation of the digit, a cystic swelling recurred palmar to the carpus and metacarpus. This may be because parts of the cyst wall were left behind and continued to secrete fluid.
Arthrography of the carpal joint is helpful to visualise a synovial cyst in humans. Iveson et al 7 described the arthrographic studies of rheumatoid wrist joints with cystic lesions. A fistulous tract was found to connect the midcarpal joint with the flexor tendon sheath. Diagnosis of the synovial cyst in our cat was made by plain radiography, ultrasonography, and aspiration cytology. Radiography showed severe osteoarthritis in the interphalangeal joints of the fifth digit. Arthrography was not considered at the time. According to Iveson et al, 7 the cystic swellings may be apparent before the radiographic or arthrographic appearance of arthritis. Ultrasonography is indicated for the diagnosis of wrist and hand lesions in humans. 8 We found the ultrasonographic examination of the swelling helpful to confirm its fluid contents and septae, although a connecting tract to a joint was not visible. Similar ultrasonographic findings of synovial cysts of the elbow joint in cats have been described by White et al. 3
Treatment of synovial cysts includes drainage or surgical excision. In three cats with synovial cysts of the elbow joint, the cysts were excised, but recurred within 1 year of surgery. 1 Based on their experience, Stead et al 1 recommend treating the underlying joint disease and aspirating the cysts to control their size. Children with synovial cysts of the wrists are treated with aspiration and injection of corticosteroids. 9 This treatment proved effective in reducing recurrence of the cysts. In our cat, aspiration of the synovial cyst improved the lameness, presumably by reducing intra-articular and soft tissue pressure. Analgesic treatment for the underlying degenerative joint disease with systemic or intra-articular corticosteroids should be considered, although this treatment may also cause further cartilage deterioration. 10
This case demonstrates synovial cysts as a differential diagnosis in swellings of the distal forelimb in cats. The exact aetiology is not clear but it appears that degenerative joint disease causes synovial cysts in cats. While arthritis is very common in cats, synovial cysts are rare and may be explained by additional lesions in the joints and tendons. Synovial cysts are presumably caused by excessive synovia production with degenerative joint disease, formation of bone spurs, which may cause tendinitis or tenosynovitis, and subsequent weakening or perforation of the joint capsule.