
Abstract
High sodium diets have been shown to enhance water intake and urine output, a potential benefit in the management of lower urinary tract diseases. However, one study suggested that high salt (sodium chloride) diets might have adverse effects on the kidneys [Kirk CA, Jewell DE, Lowry SR. Effects of sodium chloride on selected parameters in cats. Vet Ther 2006;
Lower urinary tract diseases (LUTDs) are considered to be common in cats. 2,3 While there are many types and causes of LUTDs, urethral obstruction, urolithiasis, and idiopathic cystitis are the three most commonly recognized forms of LUTDs in cats. 4,5 The underlying causes are unknown, so management of these conditions remains symptomatic. One aspect of the long-term management of these conditions is common for all three – a recommendation to increase water intake so as to increase urine volume. The principal is to dilute out calculogenic or inflammatory substances, and promote their excretion. In vitro and clinical studies in human stone formers have confirmed the importance of increased water intake, urine volume and urine dilution on the prevention of stone recurrence. 6,7
Canned foods are frequently recommended as a means to increase water intake in cats. In one study, cats with a history of recurrent LUTD that were fed a canned therapeutic diet had a greater decrease in recurrence rate, compared to similar cats fed a dry therapeutic diet. 8 Most canned foods contain between 70 and 82% water. Normally, cats consuming dry foods will drink more water than cats consuming canned foods, but total water intake can be greater in cats fed canned foods. 9,10
Some cats will not eat canned foods, or their owners prefer not to feed canned foods. Thus, increased water intake must be approached from other means. Several studies have shown that increasing dietary salt (NaCl) can increase water intake and urine volume, and decrease urine specific gravity, 1,11–13 all which may be beneficial in cats with LUTDs.
Therapeutic diets intended for patients with LUTDs are available that leverage the effect of NaCl on fluid throughput. However, the safety of such products has been called into question, with the suggestion that increased sodium intake could increase blood pressure and aggravate kidney disease in cats. 1 Chronic kidney disease (CKD) is a common condition among middle-aged and older cats. 14,15 It has also been suggested that increased dietary sodium results in hypercalciuria and increased risk for calcium oxalate nephroliths and urocystoliths. 16–18
Under certain conditions, high salt diets can lead to hypertension and renal dysfunction. In salt-sensitive rats, for example, feeding diets containing 8.0% salt (dry matter (dm)) induced both hypertension and pronounced renal lesions. 19 In dogs with CKD deprived of drinking water and provided with only normal saline to drink, the saline apparently increased systemic blood pressure and increased renal lesions. 20 However, this may have been an example of water-deprivation toxicosis rather than an effect of salt per se.
Given the potential concern regarding high sodium diets, the objective of this study was to assess the effects of feeding a high salt (1.11% sodium and 1.78% chloride, dm) diet to cats over a 6-month period. The study tested the hypothesis that dietary sodium would not alter blood pressure, markers of renal function, bone mineral content (BMC), or urinary calcium concentration in healthy adult cats. High sodium diets are not currently recommended for cats diagnosed with CKD. However, as it has been suggested that older cats might have clinically silent, or undiagnosed, CKD that might be affected by high sodium diets, we chose to conduct this study with a population of mature cats (mean age 7.0 years).
Methods
Animals
Twenty-four healthy adult domestic shorthair cats (mean age 7.0±1.2 years) were selected and allocated to two groups equally matched for gender, age, and body weight. Groups were randomly assigned to receive either the control diet or a high sodium diet. Water was available at all times. Cats were housed in an indoor facility with a 12 h light/dark cycle. Housing and access to environmentally enriched activity rooms were equivalent for both groups.
Diets
All cats were fed the control diet during a 2-week adaptation period prior to the start of the 6-month study. Following baseline evaluations, cats were fed either the control diet (CON) or a high sodium (NaCl) diet as their sole source of nutrition. The diets were formulated to be as similar to one another as possible except for their sodium and chloride content (Table 1). Food was provided daily in sufficient quantities to maintain body weight, and was available for approximately 16 h daily except when cats were fasted overnight prior to blood sampling or anesthesia.
Nutrient composition of diets

CON=control diet.
NaCl=test diet with increased sodium and chloride.
ME=metabolizable energy.
Experimental Design
The study protocol was approved by, and all procedures were performed in accordance with the Nestlé Purina Pet Care Animal Care and Use Committee Guidelines. Baseline evaluations included complete physical examination with body weight and body condition score (BCS), 21 serum biochemical profile, hematology, urinalysis, and indirect systolic blood pressure (SBP). Dual-energy X-ray absorptiometry (DEXA) was used to measure body composition, including BMC as a marker of potential calcium loss, and lean body mass (LBM) as an indicator of water retention. 22 Food intake was measured daily, while body weight was recorded weekly. Serum biochemistry, hematology, clinical urinalysis, and DEXA were repeated after 3 and 6 months. Blood pressure was recorded monthly.
Prior to DEXA analysis, cats were fasted overnight. Cats were sedated or anesthetized in order to prevent movement during the scan. Cats were scanned in standard sternal recumbency, using a LUNAR Prodigy Model 8743 with enCore 2003 software (Lunar Corp, Madison, WI).
Blood pressure was measured on the left foreleg using a Doppler blood pressure unit (Hadeco; Jorgensen Labs), with an 8 MHz transducer and a 2.5 cm cuff. The cuff size was selected to assure that the width would be between 30 and 40% of the forearm circumference of all cats in the study. Cats were held in a sternal position with the leg kept at the level of the heart. To reduce stress, measures were taken with minimal restraint in a quiet environment. For each cat at each sampling period, the arithmetic mean values were determined by taking 3–5 measurements of SBP excluding any values that deviated by 10 mmHg or more. If any cat appeared to become stressed during the procedure, the process was stopped, and repeated at another time. Only SBP was recorded as systolic hypertension is most commonly linked with organ damage, and because diastolic measurements are considered unreliable when assessed using a Doppler method. 23–27
Statistical Methods
Data were plotted and the resulting histogram visually evaluated to confirm normal distribution. Among parameters evaluated, only serum creatinine was not normally distributed. Creatinine data were log transformed (natural log) to stabilize the variance before the statistical analysis. The data were then analyzed with a mixed analysis of variance (ANOVA) model appropriate for a repeated measures experiment to detect effects of treatment and time, as well as interactions. In order to detect differences among a subset of cats with initially high serum creatinine, a separate two-factor, repeated measures ANOVA was used. Differences were considered significant at P<0.05. Data are presented as means with standard error of the mean (SEM).
Results
All cats completed the 6-month study. Dietary sodium had no impact on average food intake (40.8 versus 39.4 Kcal/kg body weight for CON and NaCl, respectively). Body weight and body condition remained stable over the 6-month period. Likewise, body composition measured by DEXA, including BMC and LBM, a marker of water retention, were unchanged and unaffected by diet over the 6-month period (Table 2). SBP varied by month (P<0.05), but was unaffected by dietary treatment (Table 3).
Effects of diets differing in dietary sodium and chloride on body composition of cats

CON=cats (n=12) fed the control diet.
NaCl=cats (n=12) fed the test diet with increased sodium and chloride.
BMC=bone mineral content.
Effects of diets differing in dietary sodium and chloride on SBP (Systolic blood pressure) in cats
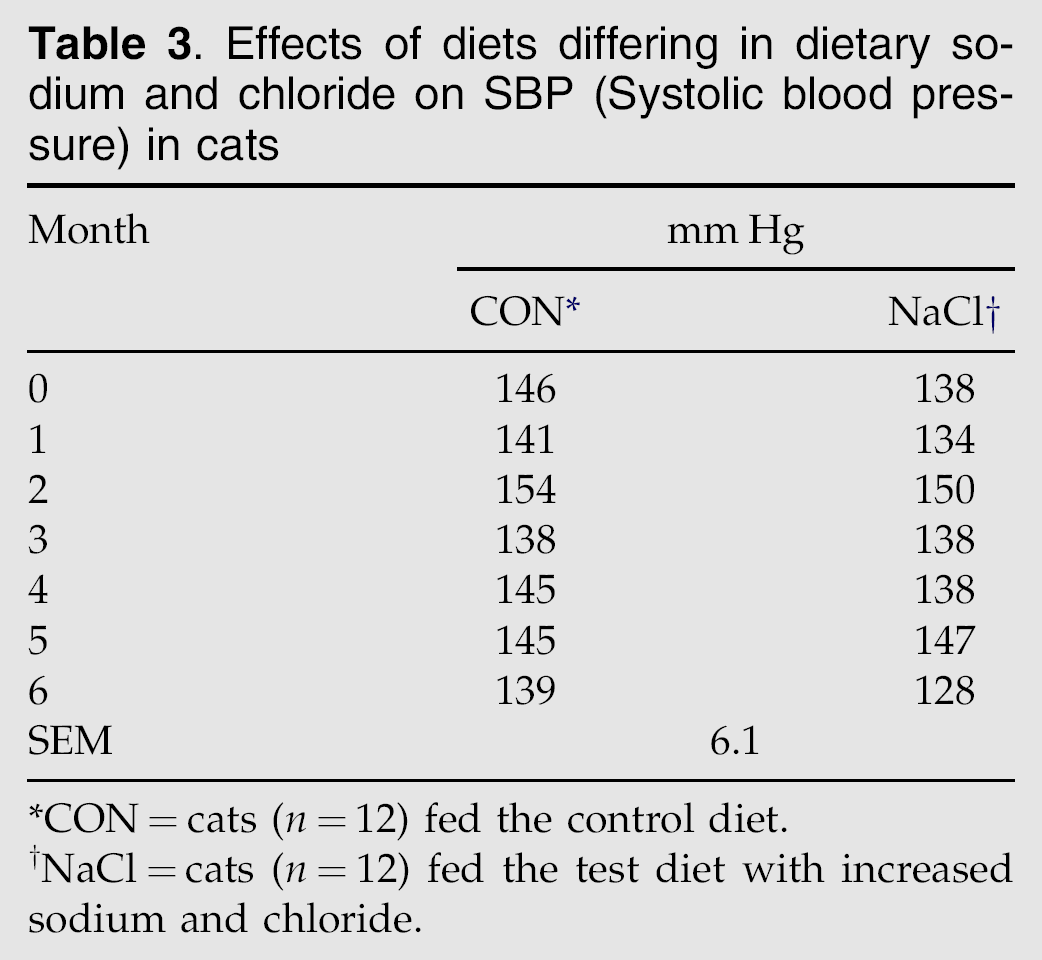
CON=cats (n=12) fed the control diet.
NaCl=cats (n=12) fed the test diet with increased sodium and chloride.
Significant differences by diet group were observed for serum cholesterol, triglycerides and albumin, which were significantly higher in NaCl cats. A time by diet interaction was observed for several blood values so that they differed between groups at individual time points only (Table 4). The change from baseline differed significantly between diets only for cholesterol at 3 months and creatinine at both 3 and 6 months.
Effects of diets differing in dietary sodium and chloride on key blood values

ALT=alanine transaminase, SAP=serum alkaline phosphatase, MCV=mean corpuscular volume.
CON=cats (n=12) fed the control diet.
NaCl=cats (n=12) fed the test diet with increased sodium and chloride.
Treatment means differed significantly independent of time, P<0.05.
Within time period, P<0.05.
Within time period, P<0.10.
Urinary sodium and chloride were significantly higher while urine protein was lower in NaCl cats at the 3-month time period (Table 5). Urine calcium, oxalate, and citrate concentrations were unaffected by diet. The urine protein to creatinine (UPC) ratio did not differ significantly by diet.
Effects of diets differing in dietary sodium and chloride on urinary minerals, protein and creatinine concentrations
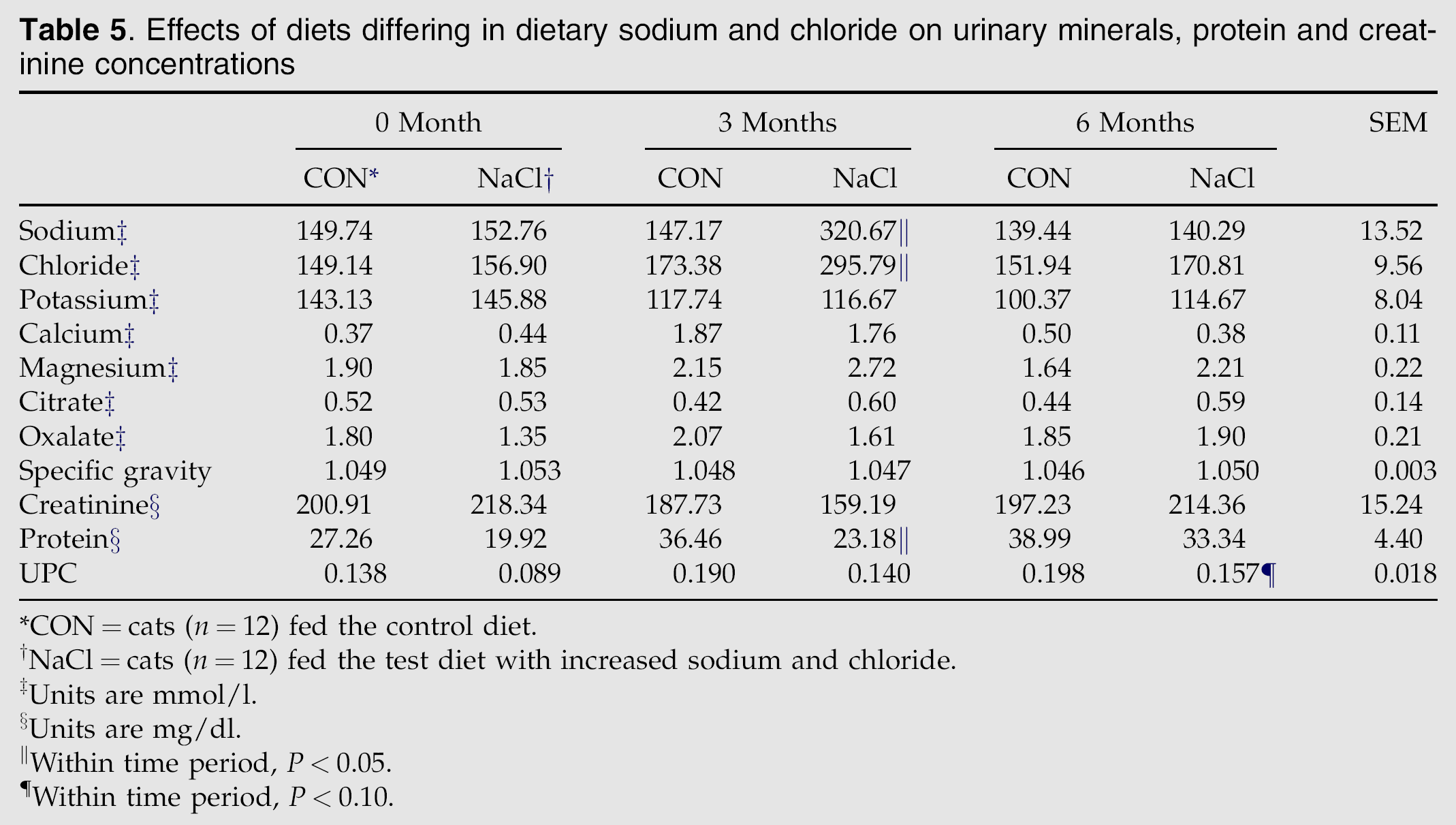
CON=cats (n=12) fed the control diet.
NaCl=cats (n=12) fed the test diet with increased sodium and chloride.
Units are mmol/l.
Units are mg/dl.
Within time period, P<0.05.
Within time period, P<0.10.
In order to more carefully evaluate the effect that diet might have on cats that may have subclinical kidney disease, the data were evaluated retrospectively to identify cats that had an initial serum creatinine above the upper limit of the reference range. Nine cats were identified that had an initial serum creatinine of 1.6 mg/dl or greater, including four CON cats and five NaCl cats. Key renal parameters 28 from these nine cats are shown in Table 6. No significant differences by diet group were detected although mean UPC increased (P=0.011) over time in this group of cats.
Effects of diets differing in dietary sodium and chloride on renal parameters in cats with baseline serum creatinine greater than 1.5 mg/dl
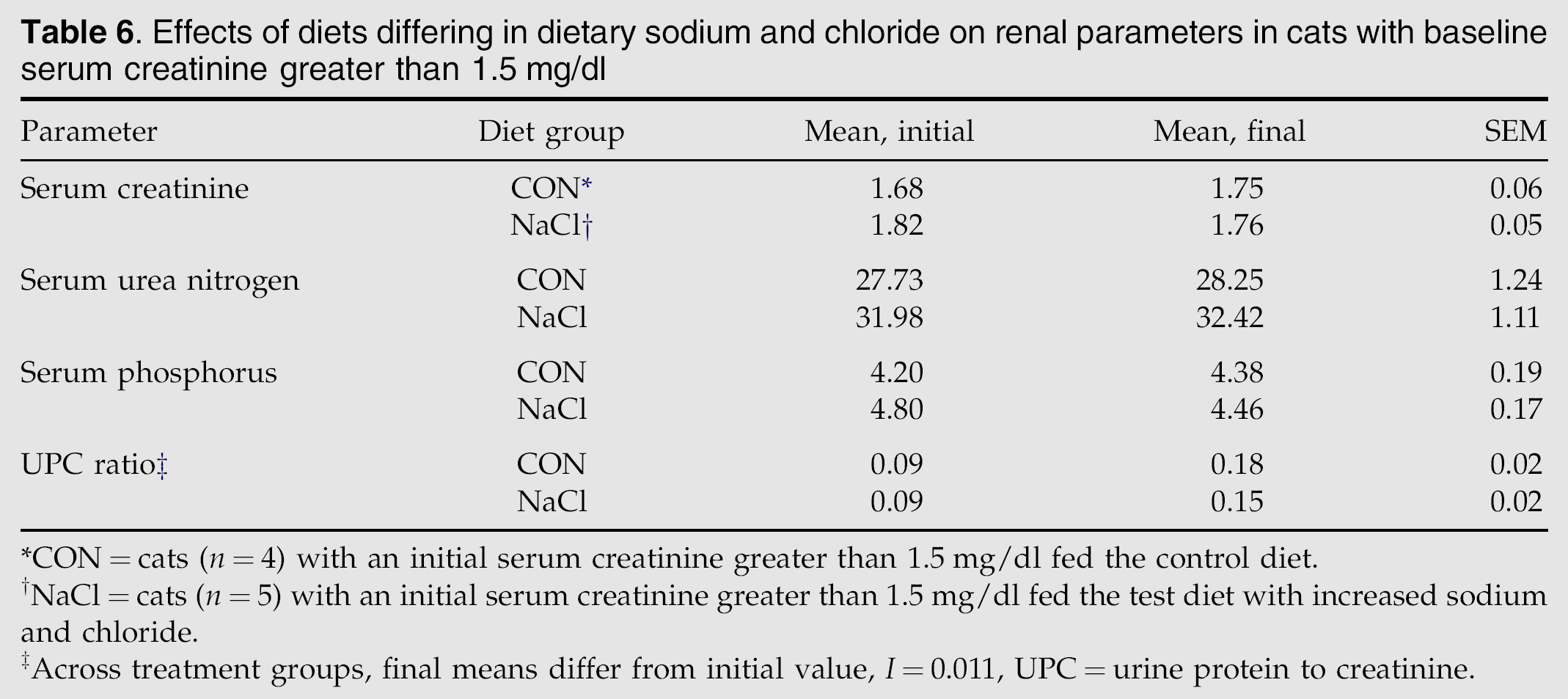
CON=cats (n=4) with an initial serum creatinine greater than 1.5 mg/dl fed the control diet.
NaCl=cats (n=5) with an initial serum creatinine greater than 1.5 mg/dl fed the test diet with increased sodium and chloride.
Across treatment groups, final means differ from initial value, I=0.011, UPC=urine protein to creatinine.
Discussion
In this study of middle-aged and older cats, dietary NaCl (sodium 1.1% dm or 29 mg/100 Kcal) had no detectable effects on blood pressure or renal function. Total body water (TBW) also appeared to be unaffected by sodium in this study. Sodium is the principal cation of extracellular fluid and a major determinant of plasma osmolality. An acute increase in sodium increases plasma osmolality and initiates a chain of events resulting in increased water intake and sodium excretion. Short-term studies have shown that TBW increases perceptibly when sodium intake is increased over a low sodium intake. 29–31 However, adaptation to altered sodium intake takes some time, and no prior publications have reported the effect of chronic sodium intake on TBW among animals with free access to drinking water. In the current study, DEXA was used as an indirect measure of increased TBW. Measurement of LBM using DEXA is sensitive to changes in TBW as nearly all TBW is present in the LBM. 22,32 Therefore, an accumulation of TBW secondary to sodium load will lead to an erroneous increase in measured LBM. Such effects were not observed in the current study as LBM, hence TBW, remained nearly constant during the 6-month study regardless of dietary sodium intake.
The lack of adverse effects noted in this study is similar to most other studies in healthy dogs and cats, and those with CKD, wherein diets containing up to 3% NaCl had no adverse effects on blood pressure or kidney function, so long as sufficient water intake was allowed. 30,33–38 An epidemiologic study also supports the safety of dietary sodium. Rather than a risk factor, increased dietary sodium was identified as a protective factor against the development of CKD in cats. 39
To date, only one study in cats reported adverse renal effects from dietary NaCl. 1 Six cats with CKD, as well as 30 healthy cats, were enrolled into that study. The authors reported a number of changes associated with an increase in NaCl intake, including an increase in urinary calcium excretion, serum creatinine, serum urea nitrogen and serum phosphorus. Why this one study differed from all others is not clear. While the diets used in that study were similar in sodium and chloride to the diets used in the current study, protein, fat, calcium and other nutrients differed. It is unclear at this time if any of those dietary differences could have contributed to the different outcomes reported in these two studies.
In order to more directly compare the data from the current study with data from that prior study, all cats in the current study with initial serum creatinine concentrations of 1.6 mg/dl and above were identified and their data evaluated separately. Unlike the prior study, the cats in this study showed no adverse effects attributable to dietary NaCl.
Another concern associated with increased sodium intake is hypercalciuria or increased calcium excretion. 16–18 In humans, increased sodium intake can increase urinary calcium, which could contribute to osteoporosis, as well as to calcium oxalate urolithiasis. In this study, the NaCl diet had no effect on urinary calcium concentration or on BMC. These results are consistent with other studies in both cats and dogs showing that increased dietary sodium not only does not increase urinary calcium concentration, but also it reduces the relative supersaturation of calcium oxalate. 12,40–42 Further, epidemiological data suggest that higher sodium intake is a protective factor against calcium oxalate urolithiasis in cats and dogs. 43–46
In summary, this study showed that healthy mature cats demonstrated no adverse effects when fed a nutritionally complete and balanced diet containing 29 mgNa/100 Kcal over a 6-month period. These findings are in agreement with most prior research, as well as with the newest nutritional guidelines for cats published by the National Research Council (NRC). 47 According to the NRC, the safe upper limit (defined as the highest amount known to be safe) for sodium intake in healthy cats is greater than 1.5% of the diet dm, as no adverse effects due to sodium have been demonstrated. 47 The impact of dietary sodium in cats with CKD remains controversial, yet the great majority of data indicates no adverse effects even in cats with CKD. Veterinarians who prescribe diets containing increased sodium content to cats suspected to have CKD, heart disease, or other conditions for which sodium restriction has historically been recommended should re-evaluate those patients regularly to assure that the desired effect has been achieved. This advice applies for all patients with chronic conditions, regardless of the therapy recommended.
Footnotes
Acknowledgments
The authors wish to thank Wendell Kerr for his assistance with statistical analyses. This study was funded and conducted by Nestle Purina Pet Care Global Resources, Inc.