
Abstract
An 11-year-old female domestic shorthair cat with a previous history of having been spayed, presented with signs of abdominal distension, lethargy and anorexia of 1 week's duration. On the basis of radiological and ultrasonographic findings a tentative diagnosis of pyometra was made. Exploratory coeliotomy revealed a 900° left horn uterine torsion along the longitudinal axis. Ovariohysterectomy was performed without correction of the torsion. To the authors' knowledge this is the first case report of uterine torsion in a non-gravid cat.
Uterine torsion is defined as twisting of the uterus or uterine horn perpendicular to its long axis (Biller and Haible 1987). It is an uncommon problem in almost all domestic species other than cattle (Misumi et al 2000) and has been only rarely reported in cats (Thilagar et al 2005). Uterine torsion has been observed in cats in mid- to late gestation (Thilagar et al 2005). In other species, pregnancy is suggested as the main factor contributing to uterine torsion because the occurrence is higher in the gravid compared to the non-gravid animal (Misumi et al 2000). The aetiology of uterine torsion is unknown. Factors such as foetal movement, uterine contraction, rough handling during pregnancy, lack of tone of the pregnant uterus, lack of foetal fluids, flaccid uterine walls and a long flaccid mesometrium have been suggested as contributing factors (Biller and Haible 1987, Freeman 1988).
This report describes the clinical findings, surgical management and clinical outcome of a uterine torsion in a non-gravid cat.
An 11-year-old female domestic shorthair cat weighing 3.7 kg was referred to the Royal Veterinary College, London, for evaluation of abdominal distension, lethargy and anorexia of 1 week's duration. The owner reported that the cat had been obtained from a rescue centre 5 years previously and was reported to have been spayed. One year later, the cat developed signs of oestrus (vocalisation) and a second ovariohysterectomy was reported to have been performed, details of the technique used and findings at surgery were not available.
On physical examination the cat was quiet but alert. The abdomen was distended and there was pain on abdominal palpation. An approximately 6×3 cm fluid filled mass was palpable in the mid-abdomen. There was no vulval discharge. The reminder of the physical examination was unremarkable. The differential diagnoses at this time included splenic neoplasia, splenic torsion, intestinal neoplasia such as lymphoma, lymphadenomegaly, hepatomegaly, intussusception, intestinal volvulus, intestinal foreign body, left sided renomegaly or a pancreatic abnormality. Uterine involvement was not considered in view of the neutered status.
Haematology revealed a normochromic, normocytic, non-regenerative anaemia with a haematocrit of 16.6% (reference range 24–45%). Serum biochemistry and coagulation panel (prothrombin time and activated partial thromboplastin time) were within normal limits and the results of feline leukaemia and feline immunodeficiency virus enzyme-linked immunosorbent assay (ELISA) analysis were negative. Right and left lateral thoracic radiographs were within normal limits. Lateral and ventrodorsal radiographs of the abdomen revealed a 6 cm long, tubular, soft tissue opacity in the mid-ventral abdomen with dorsal displacement of the small intestines (Fig 1). Abdominal ultrasound revealed a large fluid filled viscous compatible in appearance with the uterus. Cysts within the right ovary and mild ascites were also visible. Abdominocentesis was not performed at this time. There was no evidence of pregnancy on abdominal radiographs or ultrasound. A presumptive diagnosis of pyometra was made.

Lateral abdominal radiograph: a tubular soft tissue opacity is visible in the mid and caudal ventral abdomen with dorsal displacement of the descending colon and cranial and dorsal displacement of the small intestine.
The cat was treated with intravenous (IV) crystalloid fluid (Hartmann's Aquapharm No 11, Animal Care) at a rate of 4 ml/kg/h and perioperative cefuroxime (Zinacef; GSK) at 20 mg/kg IV. Anaesthesia was induced with IV ketamine 5 mg/kg (Narketan 10; Vetoquinol) and IV midazolam 0.3 mg/kg (Hypnovel; Roche) and maintained with isofluorane (Isocare; Animalcare) in oxygen and nitrous oxide administered via endotracheal intubation and a non-rebreathing system. Methadone (Physeptone; Martindale Pharmaceuticals) was administered at a dose of 0.2 mg/kg IV.
Exploratory coeliotomy was performed via a ventral midline incision revealing the presence of a non-gravid distended uterus with a 900° torsion of the left uterine horn along its longitudinal axis. The affected section of uterus was grossly distended and congested (Fig 2). The right uterine horn was distended but had a normal appearance. A small volume of peritoneal fluid was observed and a sample was obtained for cytology, culture and sensitivity analysis. Right and left ovaries were identified caudal to the respective kidneys, multiple follicular cysts were observed on the right ovary, and the left ovary was grossly normal. There was no visible evidence of prior surgery. An ovariohysterectomy was performed using a standard technique; the torsion was not corrected prior to performing the ovariohysterectomy. The abdomen was copiously lavaged using 1 l of Hartmann's (Aquapharm No 11; Animal Care) and a standard midline closure was performed. The ovaries and uterus were sent for histopathology, aerobic and anaerobic culture and sensitivity tests. The cat made an uneventful recovery and was sent home 3 days postoperatively.
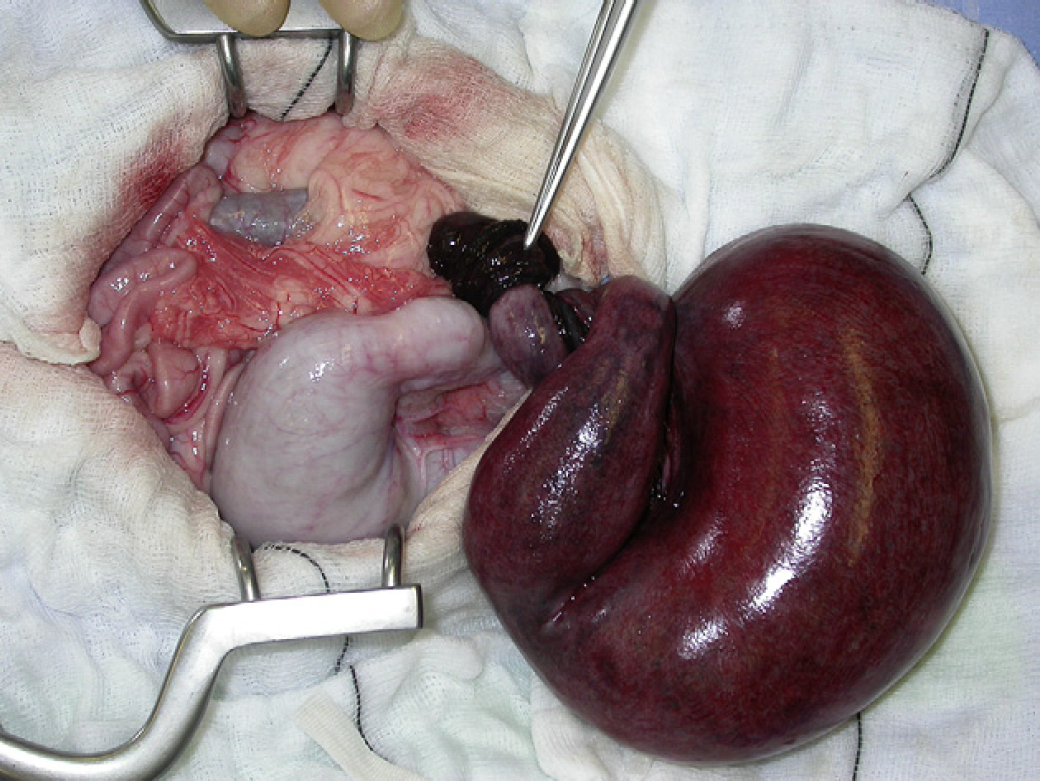
Intra operative photograph demonstrating left horn uterine torsion and the distension of the right uterine horn.
Cytology of peritoneal fluid was consistent with neutrophilic inflammation total white cell count 5.5×109/l, with a predominance of mildly degenerated neutrophils (88%), macrophages (7%), small lymphocytes (5%) and occasional mesothelial cells. Fluid protein was 42.4 g/l compatible with an exudate. No bacteria were noted on cytology and aerobic and anaerobic bacteriology were negative after 48 h incubation. On histopathological examination, the left uterine horn was oedematous and haemorrhagic with necrosis of the endometrium. The right ovary was cystic. No bacteria were cultured after a 48 h period of incubation from the uterine fluid or tissue. Based on these results a diagnosis of mucometra was made.
Seventeen cases of feline uterine torsion have been reported, all affecting pregnant queens (Freeman 1988, Ridyard et al 2000, Thilagar et al 2005). In dogs, uterine horn torsion has been reported in five non-gravid bitches, in three it was secondary to haematometra and two had pyometra (Misumi et al 2000). It has been suggested that a distended uterus, secondary to chronic endometritis, might rotate about the suspensory structures and the distension could enlarge further once torsion has occurred (Freeman 1988, Misumi et al 2000). In this case, the cat had a mucometra, therefore, the dilated uterus may have stretched the ovarian pedicle and broad ligament which might have made it more susceptible to torsion than a normal uterus.
Torsion of the uterus has been described as an acute abdominal condition that can be accompanied by severe metabolic and haemostatic complications (Misumi et al 2000, Ridyard et al 2000). In cats the degree of uterine torsion may vary from 180 to 900°. Previous literature suggests that this is an important factor in determining the severity and duration of clinical signs, and prognosis (Biller and Haible 1987, Thilagar et al 2005). Previously reported cats presented with acute severe clinical signs including peritonitis, septicaemia, endotoxaemia and disseminated intravascular coagulation. There has been one reported feline case with a 180° uterine torsion that presented with clinical signs of 5 days duration (Singer 1960). In the case presented here, clinical signs had been present for 1 week before examination. The longer duration of clinical signs and absence of cardiovascular compromise could have been due to the presence of a mucometra compared to a pyometra or foetal death.
An exploratory coeliotomy is indicated to make a definitive diagnosis and to correct uterine torsion. An ovariohysterectomy should be performed without correction of the torsion, as release of endotoxins and inflammatory mediators into the systemic circulation may lead to further compromise of the vital organs (Ridyard et al 2000). In those cases where the torsion was corrected intraoperatively, an unsuccessful outcome was reported (Pankhurst and Newman 1961, Young and Hiscock 1963). The prognosis for uterine torsion in the cat is favourable based on the outcome of the cases reported, where 12/15 cats survived following ovariohysterectomy (Freeman 1988). The literature suggests that in cats, a successful outcome not only depends on the degree of uterine torsion but also on effective pre- and postoperative medical supportive therapy and prompt surgical intervention.
The present case was unusual as the uterine torsion occurred in a non-gravid queen and she presented with mild clinical signs despite the presence of a 900° left uterine horn torsion. To the author's knowledge this condition has not been reported in a non-gravid queen. As a result, uterine torsion should be considered as a differential diagnosis for abdominal distension in intact, non-gravid, female cats.
Footnotes
Acknowledgement
The authors would like to thank Dr Sue P Gregory for her support and help in the preparation of this text. To Joan Rest for interpreting the histopathology samples of this case and to Panagiotis Mantis for the interpretation of the abdominal ultrasound images.