
Abstract
A 4-year-old, male castrated European shorthair cat was presented with a firm mass palpable on the right caudal rib cage. Lateral and ventrodorsal radiographs of the thorax revealed a 4×3×2 cm large, expansile and radiodense mass originating from the distal part of the 13th rib. After removal of the tumour, which was histopathologically confirmed as feline osteochondromatosis, the diaphragm, omentum, external abdominal oblique and latissimus dorsi muscles were used to reconstruct the defect. Feline osteochondromatosis is induced by retroviruses, eg, feline leukaemia virus, for which the cat tested positive. The tumour was removed for palliative reasons, because such tumours have the tendency to transform into osteosarcomas. Six months after the surgical excision the cat showed no clinical signs of reoccurrence.
Thoracic wall tumours that have been most commonly reported are chondrosarcoma, osteosarcoma, and fibrosarcoma or other spindle cell tumours, such as haemangiopericytoma or malignant Schwannoma (Pirkey-Ehrhart et al 1995). We found a rare case of feline osteochondromatosis originating from the 13th rib in a cat. Reconstruction of the thoracic wall after trauma or surgical removal of a neoplasia can be a challenge. We describe the reconstruction of the created defect without any implants, using only the adjacent musculus obliquus externus abdominis and musculus latissimus dorsi.
A 4-year-old, male castrated European shorthair cat was referred to the Department of Small Animals and Horses, University of Veterinary Medicine in Vienna, with a growing tumour attached to the last ribs on the right thoracic wall. It was discovered by the owner 3 weeks earlier and had increased in size.
At presentation the cat was bright and alert. The body temperature was 38.9°C. An extended clinical examination was unremarkable. The patient was not vaccinated, but was wormed on a regular basis.
A lateral and ventrodorsal radiograph of the caudal thoracic wall, taken by the referring veterinarian 1 week previously, revealed a 4×3×2 cm large, expansile mass originating from the distal part of the 13th rib on the right side. The mass had a non-homogeneous bone density and smooth margins. The transition zone to the non-affected rib was short. There was no periosteal reaction at the level of the non-affected rib. Based on the radiographic appearance, the tentative diagnosis of an osteoblastic bone tumour was made. Differentials were osteochondroma, osteoma, chondrosarcoma, and cartilagenous exostosis. To rule out pulmonary metastasis thoracic radiographs were taken in right and left lateral and dorsal recumbency. No radiological signs of metastasis were found (Fig 1).

Lateral and ventrodorsal view radiographs of the caudal thorax. There is well-marginated, expansile skeletal mass, arising from the distal part of the 13th rib on the right side. The mass is of non-homogeneous bone density and shows smooth margins. The lesion blends smoothly with the non-affected rib. There is no periosteal reaction at the level of the non-affected rib; the transition zone to the non-affected rib is short.
A blood sample for haematology and chemistry was taken. The haematology revealed mildly elevated eosinophilic granulocytes with 16.9% (reference value<4%) and 1335.10/μl (reference value<800/μl), which was interpreted as of unspecific origin. Blood chemistry showed a total protein of 77.4 g/l (reference range 60–75 g/l), renal and liver enzymes were within normal limits. A fine needle aspirate from the mass was taken with a 20 gauge needle and a 5 ml syringe under negative pressure. The cytology results were inconclusive.
A biopsy was taken under general anaesthesia. Butorphanol-tartrate (Alvegesic, 0.2 mg/kg, Alvetra Werft AG, Vienna) and medetomidine (Domitor, 10 μg/kg, Orion Pharma, Finland) were used as premedication. The anaesthesia was introduced with propofol (Propofol 1% Fresenius, 0.1 mg/kg, Fresenius Kabi, Graz) intravenously and after intubation maintained with isoflurane (Isoflurane, 1–2 vol%, Abbott Laboratories, UK) as inhalation anaesthesia.
A small, 5 mm, skin incision was made centrally above the mass and a Jamshidi needle (VI Jamshidi, 16G×2 in.-50 mm, Veterinary Instrumentation, UK) was introduced to obtain the biopsy. This procedure was repeated twice in different directions through the same skin incision. The samples were fixed in 10% formalin solution and subjected to histological examination. Pathohistological diagnosis of the biopsy samples was a well-differentiated chondrosarcoma. Surgical resection due to the relatively low metastatic rate was recommended (Hunt 2005).
For surgery, the same anaesthetic regimen as described above was used with nerve block anaesthesia of the intercostal nerves of the 11th, 12th, and 13th rib using lidocaine (Xylanest purum 1%, 5 mg for each nerve, Gebro Pharma, Fieberbrunn). The skin was incised in a square and the subcutaneous tissue dissected perpendicularly to the skin with a 2 cm margin from the tumour in all directions until the thoracic wall was reached. Care was taken to maintain the dimension of the surgical margin. At the cranial and dorsal margins of the incision parts of the latissimus dorsi muscle and at the caudal and ventral margins parts of the abdominal external oblique muscle were removed. At the 11th intercostal space thoracotomy was performed. While the thoracic cavity was open, the cat received intermittent positive pressure ventilation. The thoracotomy revealed the intrathoracic component of the tumour, which was evaluated and due to the size of the tumour it was decided to extend the resection one rib further cranially to provide adequate surgical margins. The intercostal arteries of the 11th, 12th and 13th rib to be removed were cauterised and the ribs were cut at the dorsal and ventral extents of the excision with bone cutters. To reconstruct the caudal thoracic defect, the diaphragm was advanced cranially for attachment with the distal remnants of the 11th rib and intercostal muscles of the 10th rib with simple continuous sutures (Biosyn 2/0, Glycomer 631, Syneture, Neustadt/Donau). The omentum was placed as a double layer into the defect and sutured with preplaced simple interrupted sutures (Biosyn 2/0, Glycomer 631, Syneture, Neustadt/Donau). Cranial to the defect, the remnant of the latissimus dorsi muscle was separated from its origin at the thoracolumbar fascia and rotated caudoventrally to close the defect partially. Caudally from the defect, the lumbar abdominal external oblique muscle was undermined by blunt dissection. The first incisions to free the muscle were dorsally along the thoracolumbar fascia and ventrally along the direction of fibres of the lumbar abdominal external oblique muscle, taking care not to damage the cranial branch of the cranial abdominal artery. The muscle was transposed cranially. A U-V-tension relieving incision was necessary at its aponeurosis that inserts at the linea alba. The incision extended 2 cm proximal and 2 cm craniocaudal from the caudoventral corner of the muscle.
Abdominal external oblique muscle and latissimus dorsi muscle were sutured together with simple interrupted sutures (Fig 2). Dorsally these muscles were sutured to the abdominal longissimus dorsi muscle, leaving a triangular gap on the dorsal margin of the wound, which was only covered by omentum. Because of its proximity and size of 2×1×1 cm no implant was used to close the defect further (Fig 3). A bilateral advancement flap was used to close the skin wound, the skin being surgically elevated below the cutaneous trunci muscle to preserve the subdermal plexus responsible for the cutaneous blood supply.
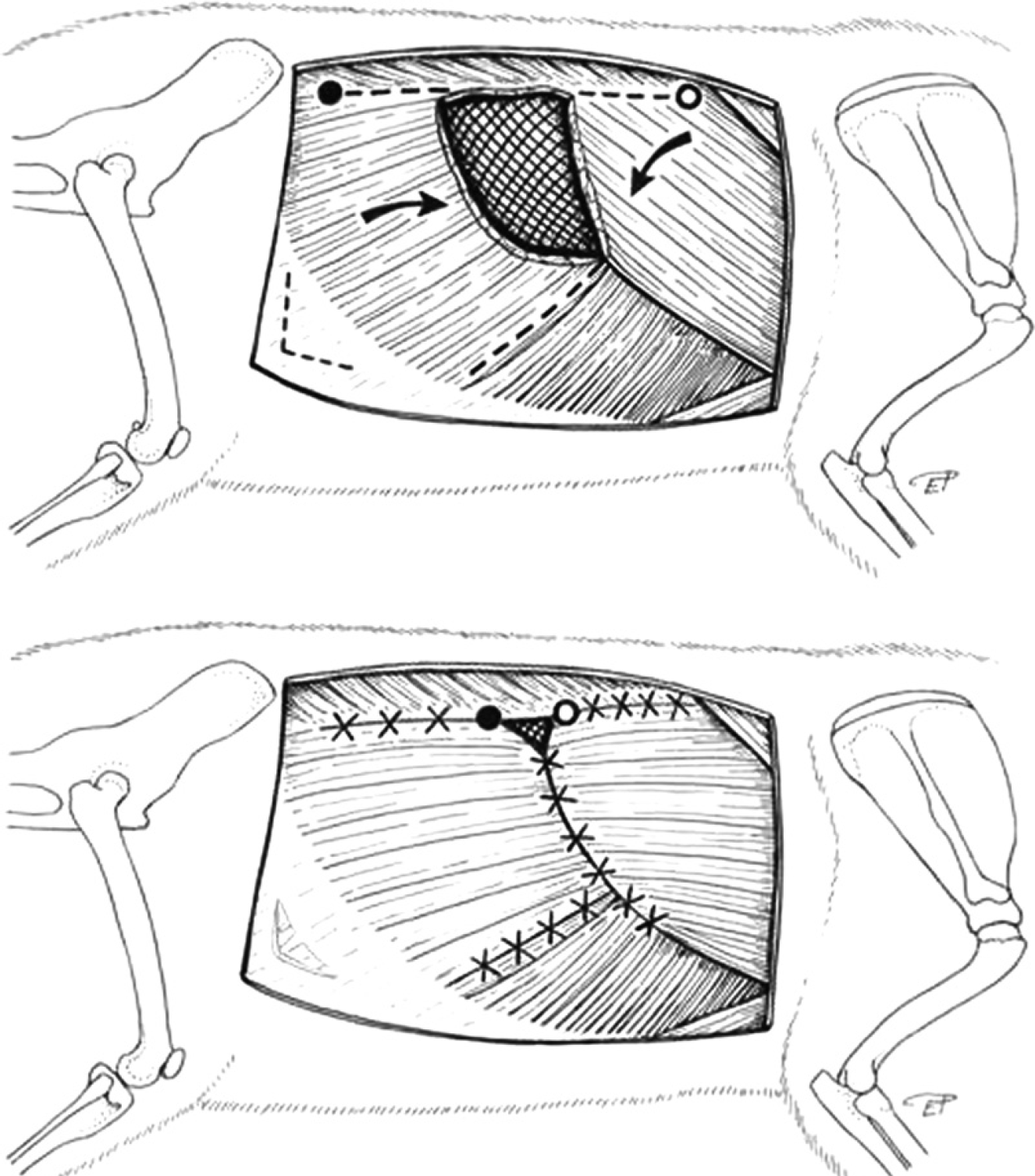
Line drawings of the muscular flaps after removal of the neoplasia and the following reconstruction; the arrows indicate the advancement of the external abdominal oblique muscle and the rotation of the latissimus dorsi muscle in a dorsoventral direction. Caudoventrally on the fascia of the musculus obliquus externus abdominis the U-Y releasing incision was left unsutured. The circles show the extent of the shift towards the created wound. The crosses stand for the placed simple interrupted sutures.
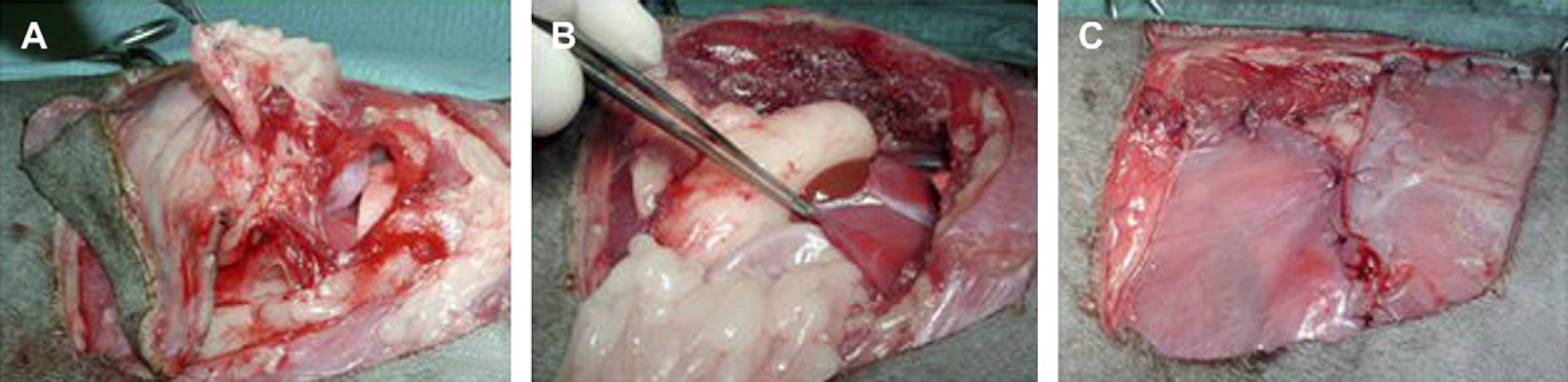
(A) Osteochondroma by thoracotomy at the 11th intercostal space. (B) Advancing the diaphragm (forceps) cranially to close the thoracal cavity. (C) Cranially (right): latissimus dorsi muscle, dorsally: longissimus dorsi muscle and caudally (left): external abdominal oblique muscle.
During the postoperative period intravenous maintenance fluid (Elo-mel OPG, Fresenius Kabi, Graz) at a rate of 2 ml/kg/h was applied for 24 h. When the cat was fully awake a bandage was applied to protect the wound. For pain management buprenorphine (Temgesic, 0.01 mg/kg IV, AESCA Gesmbh, Traiskirchen) was used every 6 h and carprofen (Rimadyl, 2 mg/kg IV, Pfizer, Vienna) every 24 h for 3 days. Cefazolin (Cefazolin Sandoz, 20 mg/kg IV, Sandoz, Kundl) was given as an antibiotic every 12 h for 3 days. The cat was released 3 days postoperatively with tramadolhydrochlorid (Tramal, 1 mg/kg PO for 5 days, Grünenthal, Brunn am Gebirge) and carprofen (Rimadyl, 2 mg/kg PO for 3 days, Pfizer, Vienna) as pain management.
The surface of the lobulated mass was covered partly with irregularly thick cartilage, partly with periosteum-like connective tissue. The majority of the mass were composed of trabecular bone (Fig 4). The marrow spaces contained predominantly adipocytes, but also loose fibrous connective tissue and islands of haematopoietic tissue. The cartilage tissue showed slightly irregular growth and mild cellular pleomorphism. Mitoses were not found. The osseous tissue was well differentiated. The surface was smooth and showed no signs of infiltrative growth. Based on the biphasic pattern of the neoplasm a diagnosis of feline osteochondroma/osteochondromatosis was made.

Histological section of the neoplasm: note focal chondroid caps (asterisks) covering parts of the tumour mass; the centre of the neoplasm is composed of well-organised lamellar bone. Bar=7.5 mm.
Feline leukaemia virus (FeLV) antigen was detected in the serum using a commercially available enzyme-linked immunosorbent assay (ELISA) (Snap FeLV Antigen Test, Idexx laboratories, USA). Paraffin embedded sections of the neoplasm were deparaffinised essentially as described by Sorg and Metzler (1995) and Benetka et al (2004) and nucleic acids were extracted using the QIAamp viral RNA Kit (Qiagen, Austria). The nested polymerase chain reaction (nPCR) assay for FeLV proviral DNA (Hofmann-Lehmann et al 2001) gave a positive result. The sample was processed twice in parallel along with a negative control of water through all laboratory procedures. To avoid contamination, the amplification product of the first round was added to the nPCR reaction mix in a separate laboratory and an airflow unit both used only for this purpose.
Primary bone tumours are uncommon in cats, with a reported incidence of 4.9 per 100,000 cases (Dernell 2003). The incidence of feline osteochondromatosis is less common than in canines and accounts for approximately 20% of primary bone tumours (Cullen et al 2002). Most cats are 2–4 years old at the time the exostosis is discovered first. Sites of skeletal involvement are the rib cage, scapulae, vertebral column, skull, pelvis, and bones of the limb. Clinically the nodular masses are asymptomatic unless they encroach muscles and tendons and lead to musculoskeletal problems (Thompson and Pool 2002). Radiographically, an osteochondroma can be indistinguishable from other primary bone neoplasia. Radiographs are, however, helpful in determining the site of the lesion, extent of involvement and therapy control. In humans, fine needle aspirate biopsy cytology is used with increasing frequency in the diagnosis of bone tumours and is associated with high diagnostic accuracy with values above 85% (Jorda et al 2000). Reinhardt et al (2005) reported that the diagnosis of osteosarcoma based on cytology alone is uncertain, especially in well-differentiated osteosarcomas. Furthermore, it is difficult to differentiate inflammatory or reactive bone proliferations and neoplasia based solely on cytological examination (Stockhaus and Teske 2002).
The initial histopathological diagnosis, which was based on biopsies, was a well-differentiated chondrosarcoma. The biopsy was taken following the guidelines of Wykes et al (1985). Multiple biopsies of the centre of the lesion penetrating through the medullary cavity were taken. Given the survival time of 250 weeks for chondrosarcoma surgical removal of the mass was recommended (Baines et al 2002). When the complete tumour underwent a histopathological examination the diagnosis of feline osteochondromatosis was made. In man, a large retrospective study on errors between biopsy and the excised mass (Mankin et al 2006) showed 60 (18.2%) major errors in diagnosis and 34 (10.3%) non-representative biopsies. Variation between the diagnosis made on the basis of the initial biopsy specimen and that made from examination of the tissue obtained at the subsequent definitive procedure occurred in 82 (25%) of the 329 patients. For chondrosarcoma the errors included diagnosis of osteocartilaginous exostosis, enchondroma and chondromyxoid fibroma (16.3%). The estimated number of unreported cases in veterinary medicine is most likely higher and further studies on this topic are urgently needed. The final diagnosis in the present case was feline osteochondromatosis. This term is deduced from osteochondroma, which is defined as a cartilage capped exostotic benign tumour arising from the surface of a bone. A solitary lesion is referred as osteochondroma, and the presence of multiple lesions is defined as multiple cartilaginous exostosis in human medicine (Green et al 1999), while in cats the condition is also known as feline osteochondromatosis. Although this term is well established in veterinary medicine, the name osteochondromatosis is misleading because osteochondromatosis in dogs and horses describes a developmental disturbance that ceases at skeletal maturity. Multiple cartilaginous exostoses are hereditary in dogs and histologically identical with the feline osteochondromatosis (Carrig 1983, Franch et al 2005). Osteochondromatosis in cats shows progressive enlargement, continuous growth throughout life, and a hereditary pattern has not been found (Pool 1993). Consistently viral particles causing feline leukaemia or transmissible feline sarcoma have been found in the neoplastic cartilage (Pool 1993, Thompson and Pool 2002), which creates a prerequisite for diagnosing this disease entirely. Only in one case report was the serological test for FeLV negative, but the neoplastic lesions and bone marrow were not tested for the presence of virus (Levitin et al 2003). In the present case with the help of PCR FeLV specific proviral DNA could be identified in the tumour, and an antigen blood test revealed a FeLV viraemia. FeLV is a retrovirus, which induces tumour growth over a considerable period of time. Approximately 20% of cats persistently infected with FeLV develop neoplasia (Cullen et al 2002). Osteochondromas may manifest at a single site or at multiple sites and have the tendency to a malignant transformation into osteosarcoma or chondrosarcoma (Pool 1993). These are usually reported as a result of a malignant transformation of a single exostosis in the dog, and a parosteal sarcoma has been described in the cat (Jongeward 1985, Pool 1993, Green et al 1999). Chondrosarcomatous transformation in humans is reported in 1–5% of solitary osteochondromas and 10–25% of patients with multiple cartilaginous exostoses (Quirini et al 1996, Kivioja et al 2000). The tendency to malignant transformation is an indication for removal of the feline osteochondroma. The life expectancy of feline osteochondromatosis is not longer than 1 year and lesions tend to occur at multiple sites of the skeleton throughout the course of the disease (Pool 1993).
The ability to gain complete, histopathologically confirmed resection is an important part of prognosis for primary rib tumours (Pirkey-Ehrhart et al 1995). This might lead to a large defect in the thoracic wall. Thoracic wall closure can be achieved by primary closure, polypropylene mesh, polypropylene mesh in conjunction with spinal fixation plates, omental pedicle flaps with polypropylene mesh and diaphragmatic advancement techniques (Aronsohn 1984, Pirkey-Ehrhart et al 1995, Hunt 2005). Autogeneous free rib grafts taken from the contra lateral side have been used experimentally for reconstruction of chest wall defects (Tuncozgur et al 1999). Pedicled muscle flaps used for thoracic reconstruction are rectus abdominis flap, abdominal external oblique muscle, latissimus dorsi and the deep pectoral muscle (Chambers 1999). With the removal of three caudal ribs reconstructive surgery to close the defect was indicated. The diaphragm attaches on the 13th rib, so the thoracic space was entered (Evans 1993). With the technique of diaphragmatic advancement the thoracic reconstruction was modified to an abdominal reconstruction. The lateral attachments of the diaphragm can be advanced to the level of the eighth intercostal space, without significantly compromising lung expansion (Aronsohn 1984). If the diaphragm needs to be advanced further cranially, partial or complete removal of the caudal lung lobe may be required (Orton 2002).
For closure of the remaining abdominal defect more than one approach was possible. Polypropylene mesh combined with a caudal superficial epigastric axial pattern flap could have been one possibility (Lidbetter et al 2002). The mesh is infiltrated uniformly with fibrous tissue to a 3–4 mm thickness at 6 weeks postimplantation. Synthetic materials have the advantages of being readily available and can be used in combination with different reconstructive techniques (Bowmann et al 1998). Because we aimed for primary closure with muscle flaps no mesh implant was used. For reinforcement and drainage of the cranial lateral abdominal wall a double layered omental pedicle flap was used. Muscles available for abdominal wall reconstruction were the latissimus dorsi and abdominal external oblique muscle. The latissimus dorsi muscle arises from the lumbodorsal fascia and thoracolumbar vertebrae and converges cranioventrally to insert on the proximal humerus (Hunt 2005). The thoracodorsal and lateral thoracic arteries supply the dorsal and ventral portions of the latissimus dorsi muscle (Pavletic 1999). The latissimus dorsi muscle was elevated from its thoracic insertion and rotated caudoventrally to close the cranial part of the defect. Because the caudal part of the square abdominal defect remained uncovered the external abdominal oblique muscle was used. The abdominal external oblique muscle consists of costal and lumbar components. The costal part originates from the fourth or fifth rib to the 13th rib. The lumbar part originates in the thoracolumbar fascia along the iliocostalis muscle (Evans 1993). The cranial branch of the cranial abdominal artery supplies the middle zone of the lateral abdominal wall and is accompanied by the cranial hypogastric nerve and a satellite vein. The deep branch of the deep circumflex femoral artery anastomoses with the cranial and caudal abdominal arteries and is the main supply to the caudodorsal fourth of the abdominal wall. It is accompanied by a satellite vein and is joined by the lateral cutaneous femoral nerve (Alexander et al 1991). In our case, a modified myofascial flap and not an island flap was created because we did not free the attachments of this muscle completely. A dorsal triangular gap of 2×1×1 cm remained and was not supported by a mesh. The dorsal location, just below the longissimus dorsi muscle together with the support by the omental pedicle flap and the myocutaneous muscle seemed to be sufficient.
The patient described here, so far, had only developed a single neoplastic mass. Follow-up examination 6 months after surgery did not reveal additional bone tumours. This seems to be an unusual course of feline osteochondromatosis which may also account for a more favourable prognosis than generally stated in the literature. Nevertheless a shorter life span of up to 5 years due to the FeLV infection has to be expected (Addie et al 2000).
Feline osteochondromatosis should be added to the differential list of skeletal tumours in cats. It is important to consider the viral aetiology for therapy and further management. If the tumour manifests at the thoracic wall, the latissimus dorsi muscle and the abdominal external oblique muscle are the muscles of choice to reconstruct the caudal thoracic wall, facilitating primary closure of a defect without implementing surgical mesh.
Footnotes
Acknowledgements
We would like to thank the Clinic of Anaesthesia and Perioperative Care and the Central Diagnostic Unit for their professional support, and the graphic artist Dr Eva Polsterer for her contribution.