
Abstract
Multilobular tumour of bone is a rare neoplasm of the skull in middle-aged, medium-to-large breed dogs even if a few cases have also been described in cats and one horse. The aim of the present paper is to show both the computed-tomography features and the pathological findings of the above neoplasm affecting the thoracic wall of a cat. To the best of the authors' knowledge, such anomalous tumour localisation has never been reported and imaged in feline medicine.
Multilobular tumour of bone (MLTB) – also known by other names such as multilobular osteochondrosarcoma, multilobular osteoma, multilobular chondroma, multilobular osteosarcoma, chondroma rodens, calcifying aponeurotic fibroma, or cartilaginous analogue of fibromatosis – is a rare, slow-growing but potentially malignant, mesenchymal tumour generally occurring in the skull of dogs (Straw et al 1989, Hathcock and Newton 2000, Lipsitz et al 2001, Thompson and Pool 2002, Yildiz et al 2003).
Histogenesis of the MLTB is still controversial. However, it has been suggested that it derives from altered periosteal elements of the chondrocranium and viscerocranium sharing the same embryologic origin (Slayter et al 1994, Thompson and Pool 2002).
The gross MLTB appearance is of a hard, nodular mass with a faint border covered by a tough fibrous membrane or by a thinner layer of intact epithelium or meninges, depending whether it projects into the soft tissues of the skull, the nasal sinuses or the cranial vault. On the cut surface, the neoplasm comprises numerous tiny, grey, gritty nodules and a few intersecting bands of fibrous tissue containing blood vessels (Thompson and Pool 2002).
The characteristic MLTB histological appearance consists of multiple oval-to-irregular cartilaginous islands, or osseous or osteocartilaginous islands surrounded by poorly defined bands of mesenchymal tissue and mature fibrous lamina at the periphery (Hathcock and Newton 2000, Yildiz et al 2003).
Although it is encountered more commonly in middle-aged, medium-to-large breed dogs, and specifically involving the flat bones of the skull (Losco et al 1984, McCalla et al 1989, Dernell et al 1998, Stoll et al 2001, Banks and Straw 2004) and orbital bones (McCalla et al 1989, O'Brien et al 1996), some cases have been reported in cats (Morton 1985, Yildiz et al 2003) and one in a horse (Richardson and Acland 1983).
In this report we aim to describe the computed tomography (CT) features and the pathological findings of an MLTB affecting the thoracic wall of a 7-year-old, spayed male, domestic short-haired cat.
The patient was referred to the ‘San Marco’ Veterinary Clinic for a CT examination and characterisation of a thoracic mass with abundant pleural effusion causing dyspnoea. The CT scanning parameters are summarised in Table 1.
Computed-tomography scanning parameters
Visipaque® 320, Amersham Health, Princeton, NJ, USA.
Envision CT Injector System, Medrand, Indianola, PA, USA.
On physical examination the cat was found to be strongly dyspnoeic and depressed. A right-sided thoracentesis allowed removal of about 35 ml of a haemorrhagic fluid, with subsequent respiratory improvement in the patient. The minimum basic data were unremarkable with the exception of a slight anaemia and hypoproteinemia, considered to be consistent with the pleural haemorrhagic effusion.
The patient underwent a whole-body CT examination. The non-enhanced series showed a large (approximately 10 cm at max diameter), well-defined mass extending from the subcutaneous tissues into the thoracic cavity, occupying the dorso-caudal part of the right hemithorax and also involving some ribs (VII–X). The mass was round in shape with a non-homogenous hyperdense appearance and coarsely stippled mineralised opacities; it was surrounded by a small amount of effusion (Fig 1). The trachea and the oesophagus were displaced. Ipsilateral lung lobes were atelectatic but not involved, whereas some ribs of the contralateral costal arch showed areas of erosion with discontinuation similar to those of the involved side (Fig 1B). Although a mild enhancement of the non-mineralised tissue could be observed, the enhanced scan series did not bring any additional useful information, with the exception of a moderate regional limphadenopathy.

(A) Three-dimensional maximum-intensity projection image. Dorsal view showing the mass displacing the thoracic tract of the oesophagus. A small amount of fluid is also visible (arrow). S=spleen; St=stomach; L=liver. Both kidneys and the left adrenal gland are also present. (B) A special workstation (ADW® 4.1, GE Medical Systems, Milwaukee, WI, USA) was used to generate a three-dimensional volume-rendered image. Arrows show different areas of erosion with discontinuation of both left and right ribs. The large mass is visible within the right hemithorax.
The CT findings were considered to be consistent with a neoplastic soft tissue mass of the thoracic wall, involving some ribs. Differential diagnosis included a vaccine-associated sarcoma.
CT-guided fine-needle aspiration and core biopsies of the mass were performed.
The pleural fluid characteristics (total protein 3.5 g/dl; specific gravity 1019; total cell count 3 520 000/mmc; nucleated cell count 13 000/mmc) were consistent with a haemorrhagic effusion. Microscopic examination revealed granulocytic leukocyte admixed with macrophages showing erythrophagocytosis. Scattered erythrocytes were evident in the background.
Cytological examination of the mass revealed a moderate cellular sample consisting of plump spindle-shaped cells with moderate-to-abundant basophilic cytoplasm and irregularly oval nucleus with finely granular chromatin and 1–2 prominent nucleoli. Scattered granulocytic leukocytes and macrophages were present. The background was moderately granular with cellular debris and erythrocytes. Cytological findings were consistent with a mesenchymal neoplasia (sarcoma) associated with neutrophilic and macrophagic inflammation.
A CT-guided biopsy specimen from the mass showed only fibrous and adipose connective tissue and also failed to reveal neoplastic cells.
The surgical option was not advisable as the mass and its bilateral spreading was too large. The owner elected for euthanasia due to the severity of the clinical signs, imaging features, and pathological findings.
Necropsy revealed an infiltrating subcutaneous mass in the right emithorax involving the 7th to 10th ribs. On blunt dissection of the costal arch a 10×7×8 cm irregularly ovoid mass was isolated, causing focal lung compression. The mass was closely attached to the intercostal muscles and to the costal arch; it was greyish in colour and was stiff and gritty in consistency.
Multiple samples from the neoplasm and from major organs were collected in 4% buffered formalin, trimmed, embedded in paraffin wax, sectioned at 4 μm and stained with haematoxylin and eosin. Portions of the mass and adjacent ribs were decalcified in 10% nitric acid solution prior to sectioning.
The neoplasm consisted of irregularly shaped lobular structures poorly demarcated by thick septae of fusiform mesenchymal elements. Atypical chondrocytes and immature bone tissue forming the matrix of the neoplasm were visible in the centre of each lobule. Each lobule was surrounded by plump fusiform mesenchymal cells interfering with the outer layer of fibrous connective tissue (Fig 2).

(A) Closer view of a lobule showing a core of chondroid matrix with atypical chondrocytes embedded, circled by bone matrix with osteoblast-like elements and spindle mesenchymal cells (original magnification 40×). (B) Islands of osteoid and chondroid elements, embedded in abundant eosinophilic matrix and haphazardly arranged, intermingled with thick infiltrating bundles of spindloid elements. Hyperchromatic cells resembling osteoblasts formed cellular palisades around the central island of matrix (original magnification 20×).
Mitotic figures were detected involving all the three mesenchymal components of the neoplasm. Huge areas of necrosis were seen throughout the neoplasm. Decalcified rib sections revealed focally extensive involvement of the periosteum by spindle neoplastic cells.
On the basis of the previously reported literature, the above findings were considered consistent with a diagnosis of MLTB. In addition, differential diagnosis with vaccine-induced sarcoma was considered but the typical features such as cellular pleomorphism, lymphoid aggregates and blue–grey pigment laden macrophages were not found (Hendrick et al 1998, Thompson and Pool 2002, Gross et al 2005).
Histopathological examination of all other samples did not reveal any significant abnormality.
The MLTB was graded according to the six morphologic criteria established for canine species (Straw et al 1989, Thompson and Pool 2002): borders, size of lobules, organisation, mitosis/10 hpf, pleomorphism of cells, and necrosis. The neoplasm described was considered to be grade 2 (Table 2) on the basis of these criteria.
Histological grading system for multilobular tumour of bone (modified from Straw et al 1989)
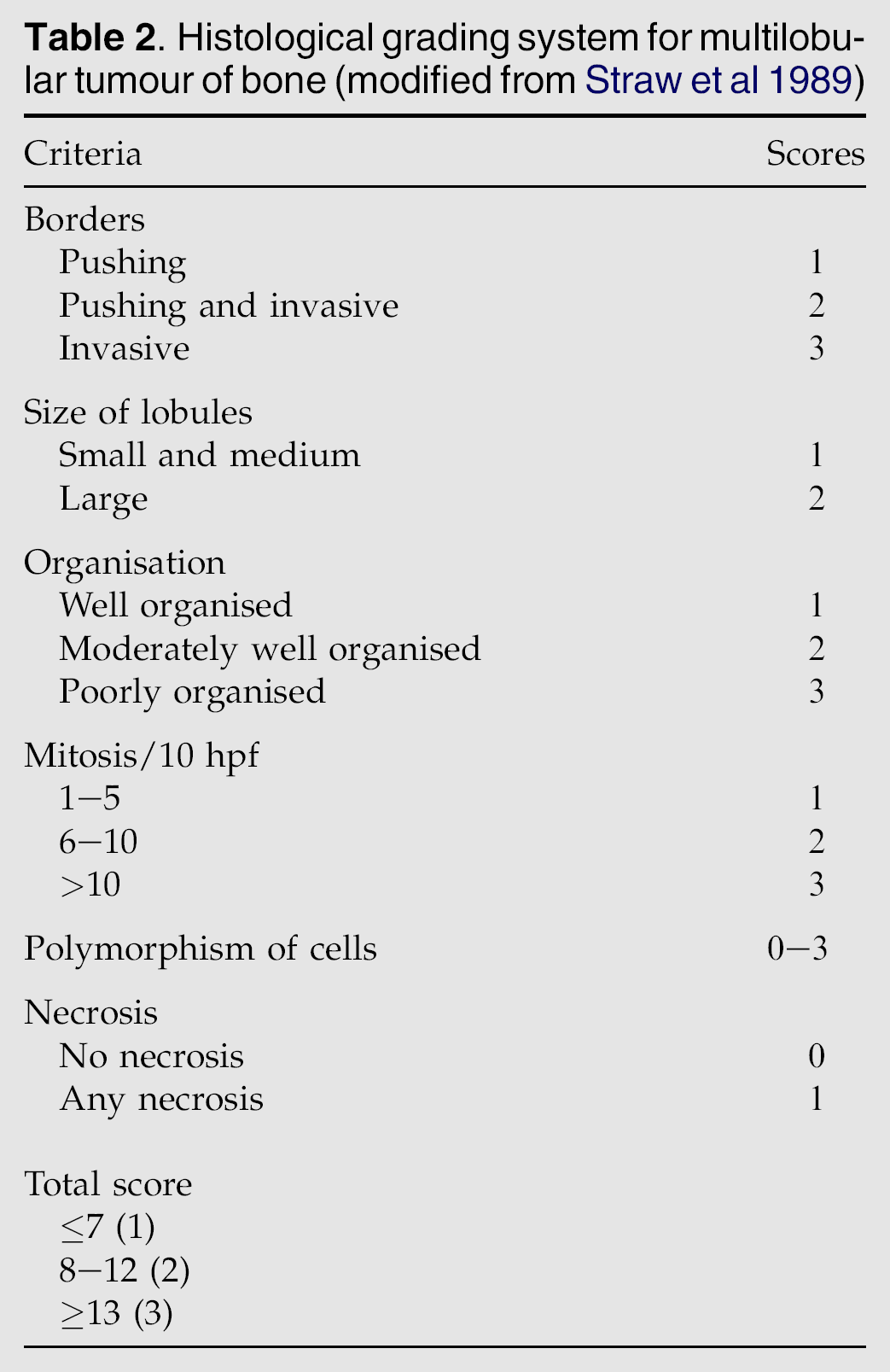
The grading system results indicate the presence of malignancy criteria in spite of the absence of metastasis to major organs and a preserved lobular structure. However, the presence of mitotic figures often implies malignant transformation (Thompson and Pool 2002).
Erosive lesions to some ribs of the contralateral costal arch were in fact detected on CT examination; unfortunately such erosions were not histologically analysed and so whether these were metastatic lesions or secondary primary neoplasms could not be determined. A previous paper described a zygomatic arch MLTB in a dog having another smaller mass in a parietal bone upon CT examination; the metastatic or secondary primary neoplastic origin was not established as well as in our reported case (Hathcock and Newton 2000). Local recurrences and pulmonary metastasis were reported secondary to malignant transformation of MLTB in a case series of 39 dogs (Dernell et al 1998). Local skull recurrence was also reported in a cat (Yildiz et al 2003).
According to the hypothesised histogenesis of the MLTB (Thompson and Pool 2002), the neoplasm in this patient seemed to arise from the periosteal elements of the ribs without infiltrating bone tissue.
To the best of the authors' knowledge this is the first reported and imaged case of an MLTB involving the thoracic wall of a cat.