
Abstract
An 8-year-old domestic shorthair was admitted with non-weight bearing left forelimb lameness. Examination and radiographs revealed dorso-medial antebrachiocarpal luxation with palmar luxation of the distal radio-ulnar joint. Primary repair was performed and stabilised using an arthrodesis wire and type Ia Kirschner-Ehmer (K-E) external skeletal fixator (ESF). The cat regained excellent pain-free limb function by 14 weeks with only minor reduction in range of movement. This is the first case report of a cat with distal radio-ulnar joint luxation associated with antebrachiocarpal luxation. Primary repair of carpal luxation in the cat should be considered before arthrodesis.
This report describes a case of dorso-medial antebrachiocarpal luxation with distal radio-ulnar luxation in a cat. The anatomical implications of such an injury and how this relates to treatment are discussed.
An 8-year-old domestic shorthair cat was presented to the Queen's Veterinary School Hospital (QVSH) with a 24-h history of severe left forelimb lameness and carpal swelling of unknown aetiology. Prior to referral the cat received carprofen (Rimadyl; Pfizer, 4 mg/kg). There were no other signs of trauma. A general clinical examination was unremarkable. An orthopaedic examination confirmed a non-weight bearing lameness of the left thoracic limb associated with marked pain and swelling of the left carpus and dorso-medial displacement of the distal limb. Following admission, opioid analgesia (buprenorphine, Vetergesic; Alstoe Animal Health, 0.01 mg/kgIMq6h) was administered before sedation and radiography.
Survey thoracic radiography was carried out following pre-medication with acepromazine (0.05 mg/kg), methadone (Physeptone; Martindale Pharmaceuticals, 0.2 mg/kg) and ketamine (Vetalar; Upjohn, 5 mg/kg). No significant abnormalities were detected. General anaesthesia was induced using alphadolone acetate and alphaxalone (Saffan; Mallinckroft Veterinary) and maintained with isofluorane (Isoflo; Abbott Animal Health) via an endotracheal tube on a modified T-piece non-rebreathing circuit. Peri-operative fluids (Hartmann's solution) were administered throughout anaesthesia (Aquapharm No 11; Animalcare, 10 ml/kg/h). Radiography confirmed dorso-medial luxation of the left antebrachiocarpal joint with palmar displacement of the distal ulna and accessory carpal (AC) bone (Fig 1). The accessory carpal bone had separated from the remaining carpal bones. Closed reduction was difficult, and was achieved by distal distraction of the carpus and application of dorso-palmar pressure on the radial–carpal bone with the carpus slightly flexed. The carpus was straightened as the radial–carpal bone engaged the distal radius. Following reduction, mild dorsal instability of the antebrachiocarpal joint (similar to a cranial drawer sign), lateral carpal instability and luxation of the styloid process of the ulna remained. The radio-ulnar luxation was characterised by dorsal and palmar movement of the distal ulna relative to the radius. It was not possible to demonstrate carpal hyperextension or re-luxate the carpus following closed reduction. Palpation of the flexor carpi ulnaris tendon revealed no significant abnormality or loss of integrity.

(a and b) Dorso-palmar and mediolateral radiographs of the left carpus showing dorso-medial antebrachiocarpal luxation and caudal luxation of the radio-ulnar joint. The accessory carpal bone has remained associated with the distal antebrachium. (c) Lateral radiograph of the normal right carpus for comparison. A cephalic intravenous catheter and associated bandage artefact is present.
The cat was placed in dorsal recumbency. Clavulanate potentiated amoxicillin (Augmentin; Smith Kline Beecham, 20 mg/kg IV) was administered and the leg prepared for surgery. The foot was covered with an adherent occlusive dressing (Op-Site Incise; Smith and Nephew) and included in the draped surgical field. Surgery was performed via a dorsal approach to the carpus allowing exploration of both collateral ligaments (Piermattei and Johnson 2004). A grade 2 medial collateral ligament sprain was identified and repaired with two horizontal mattress sutures using 2-metric (3/0) polypropylene (Prolene; Ethicon). The lateral collateral ligament was found to be intact with persistent residual lateral instability caused by luxation of the distal radio-ulnar joint. This was stabilised using a 0.9 mm trocar-tipped arthrodesis wire (‘A-wire’; Veterinary Instrumentation) placed latero-medially through the ulnar styloid process into the distal radius. The extensor retinaculum was then incised and the common digital extensor and lateral digital extensor tendons were retracted in order to facilitate repair of the dorsally ruptured joint capsule with a continuous cruciate suture of 2-metric (3/0) polypropylene. The retinaculum was repaired using a continuous cruciate pattern of 2-metric (3/0) polydioxanone (PDS-II; Ethicon). The carpus was assessed as stable through a normal range of motion with no evidence of pin entry into the joint.
The repair was protected by placement of a Type 1a trans-articular Kirschner-Ehmer (K-E) external skeletal fixator (ESF). Two Ellis pins (2.0 mm) were inserted into the cranio-medial aspect of the radius following pre-drilling with a 1.5 mm drill bit. Two ‘A’-wires (1.1 mm; Veterinary Instrumentation) were inserted mediolaterally into the proximal metacarpal bones and the frame assembled using standard techniques. Following saline irrigation the dorsal skin incision was closed with a simple continuous subcutaneous layer of 2-metric (3/0) polyglecaprone-25 (Monocryl; Ethicon) followed by a continuous intra-dermal layer of the same material.
Postoperative radiography confirmed satisfactory implant placement although a small radiolucent area was visible at the medial cortex of the second Ellis pin (Fig 2). This may have been caused by failure to locate the pre-drilled hole. The surgical wound was covered with a non-adhesive semi-occlusive dressing (Melolin; Smith and Nephew) and sterile foam pads placed between the ESF bars and the leg to limit postoperative swelling before completing the bandage.
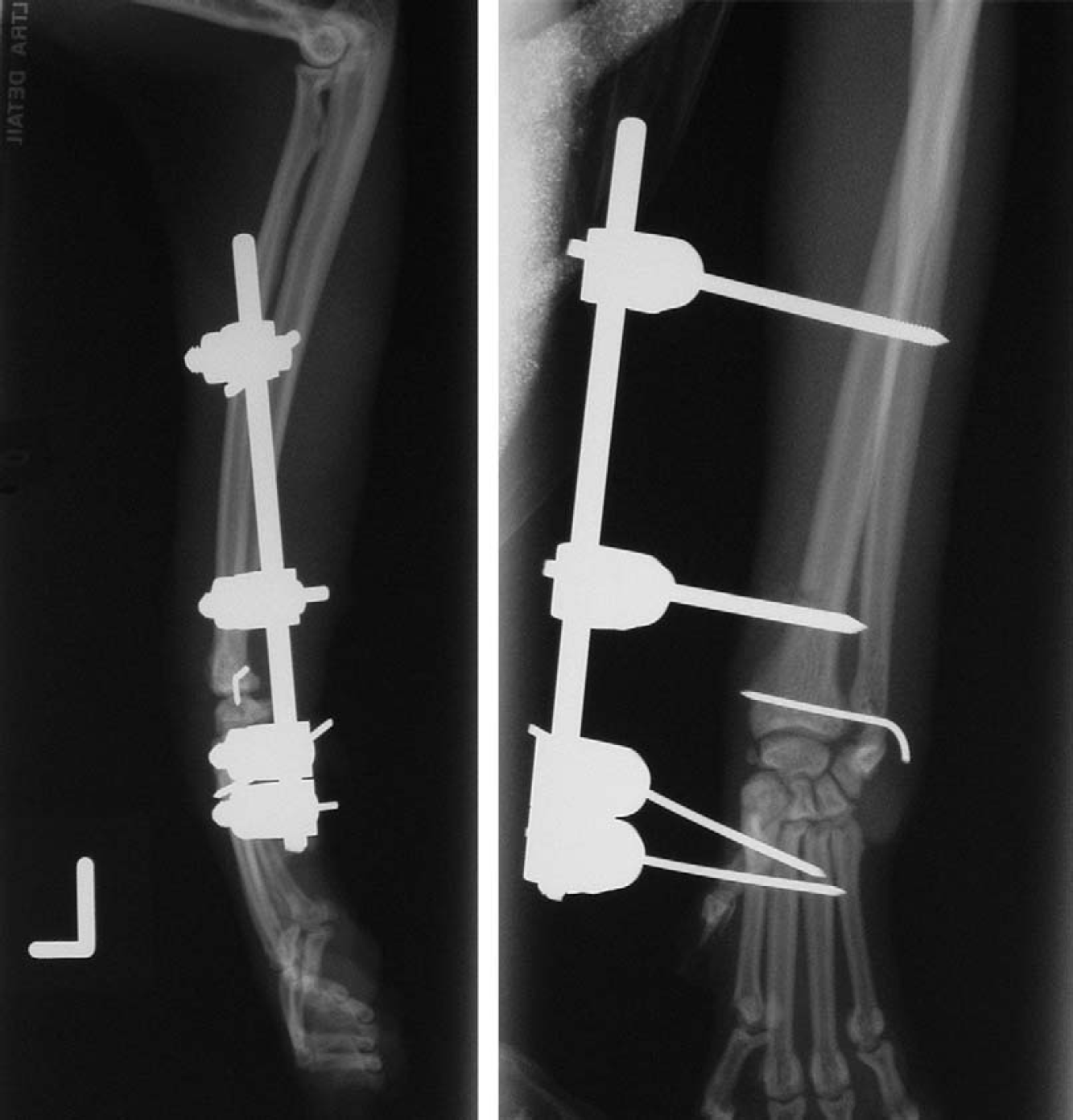
Mediolateral and dorso-palmar postoperative radiographs. There is slight radiolucency associated with the distal Ellis pin in the medial radial cortex.
Postoperative analgesia was maintained with methadone (0.2 mg/kgq3h) for 18 h followed by buprenorphine (0.01 mg/kgSCq8h) for 36 h. Potentiated amoxicillin was continued for 3 days orally (Synulox; Pfizer, 16 mg/kgq12h). The dressing was removed 24 h postoperatively under sedation using acepromazine (0.3 mg/kgIM) with medetomidine (Domitor; Pfizer, 0.03 mg/kgIM) and the clamps were checked for tightness and wrapped with adhesive bandage to cover sharp pin-ends. The cat was discharged 48 h postoperatively with instructions for confinement to a cage at home. The cage was of a similar size to those in veterinary catteries and provided enough space for a comfortable bed area, litter tray and bowls for food and water. There was enough space for limited movement but no jumping or climbing.
At follow-up examination 5 weeks after surgery, there was moderate left forelimb lameness (3/10) with no significant ESF related complications. Radiography under sedation with medetomidine (0.05 mg/kg) and ketamine (5 mg/kg) revealed a slight radiolucency around the distal radial Ellis pin and the radio-ulnar ‘A’-wire was noted to have bent slightly. Following ESF removal the carpus was palpably stable. The cat was discharged with the recommendation to continue cage rest for a further 14 days as described postoperatively.
Following ESF removal, the cat's lameness was scored as 9/10 for 48 h but no further treatment was necessary. At re-examination 14 days later (7 weeks post surgery) the cat was found to be 4/10 lame on the left forelimb. The carpus remained stable with mild reduction of carpal flexion. Radiography under sedation was unremarkable and the radio-ulnar ‘A’-wire was removed. One skin suture was placed using 2-metric (3/0) monofilament nylon (Monosof; Syneture). There was no evidence of carpal instability following pin removal. The cat was discharged with the recommendation of continued cage rest for 2 weeks with periods of supervised activity out of the cage each day. Over the following 4 weeks, the cat was allowed access to a single room and then the whole house before access to the garden was made available.
An intermediate follow-up was carried out by telephone 12 weeks postoperatively. The owner described good left forelimb use with occasional non-weight bearing following an active day. Continued house rest was advised until the next scheduled visit.
A final examination was carried out 14 weeks postoperatively. There was no detectable lameness at the walk, trot or following small jumps in the consulting room. The carpus was found to be non-painful and without crepitus. Range of movement was good with loss of approximately 10° of both flexion and extension compared to the other leg. The cat retained the ability to supinate the paw normally and had been noted to do this voluntarily while playing and grooming at home. At the time of writing (30 weeks postoperatively) there have been no further problems reported and the cat has returned to normal levels of exercise.
To the authors' knowledge this is the first report of radio-ulnar luxation associated with antebrachiocarpal luxation in the cat. Two previous reports documenting carpal luxation in cats reported successful treatment by primary repair (Pitcher 1996, Voss et al 2003). In the absence of carpal hyperextension injury primary ligament repair offers significant advantages over arthrodesis (Voss et al 2003) and should be considered whenever possible.
Following reduction, significant lateral carpal instability remained. This may have been as a result of the grade 3 radio-ulnar ligament sprain allowing luxation of the distal radio-ulnar joint (Fig 3). The radio-ulnar joint is a synovial joint whose capsule represents a proximal extension of the antebrachiocarpal joint. The fibrous capsule of the joint is essentially part of the interosseous membrane and is short and tight. The joint represents the distal pivotal joint for the rotational movement permitted between the radius and ulna (Evans 1993). Sufficient tissue for primary repair of the radio-ulnar ligament was not identified and a single ‘A’-wire was chosen to temporarily transfix the ulnar styloid process in position using a similar technique to that described for radial–carpal bone luxation (Pitcher 1996). The lack of damage to the lateral collateral ligament in this case is likely to have been due to the rupture of the radio-ulnar ligament allowing displacement of the distal ulna. The lateral collateral ligament in the cat has the same arrangement as that described in the dog (Evans 1993) (Fig 4).
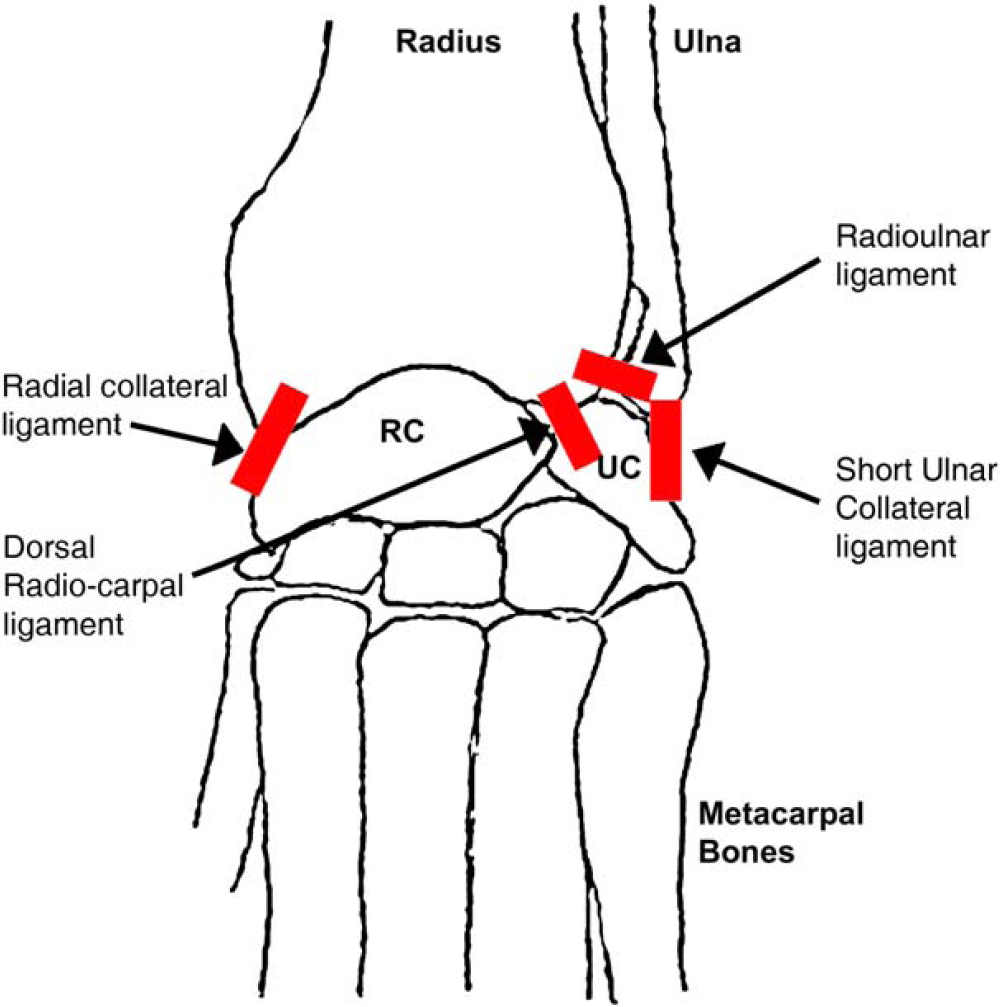
Dorsal antebrachiocarpal ligaments (modified from Evans 1993).
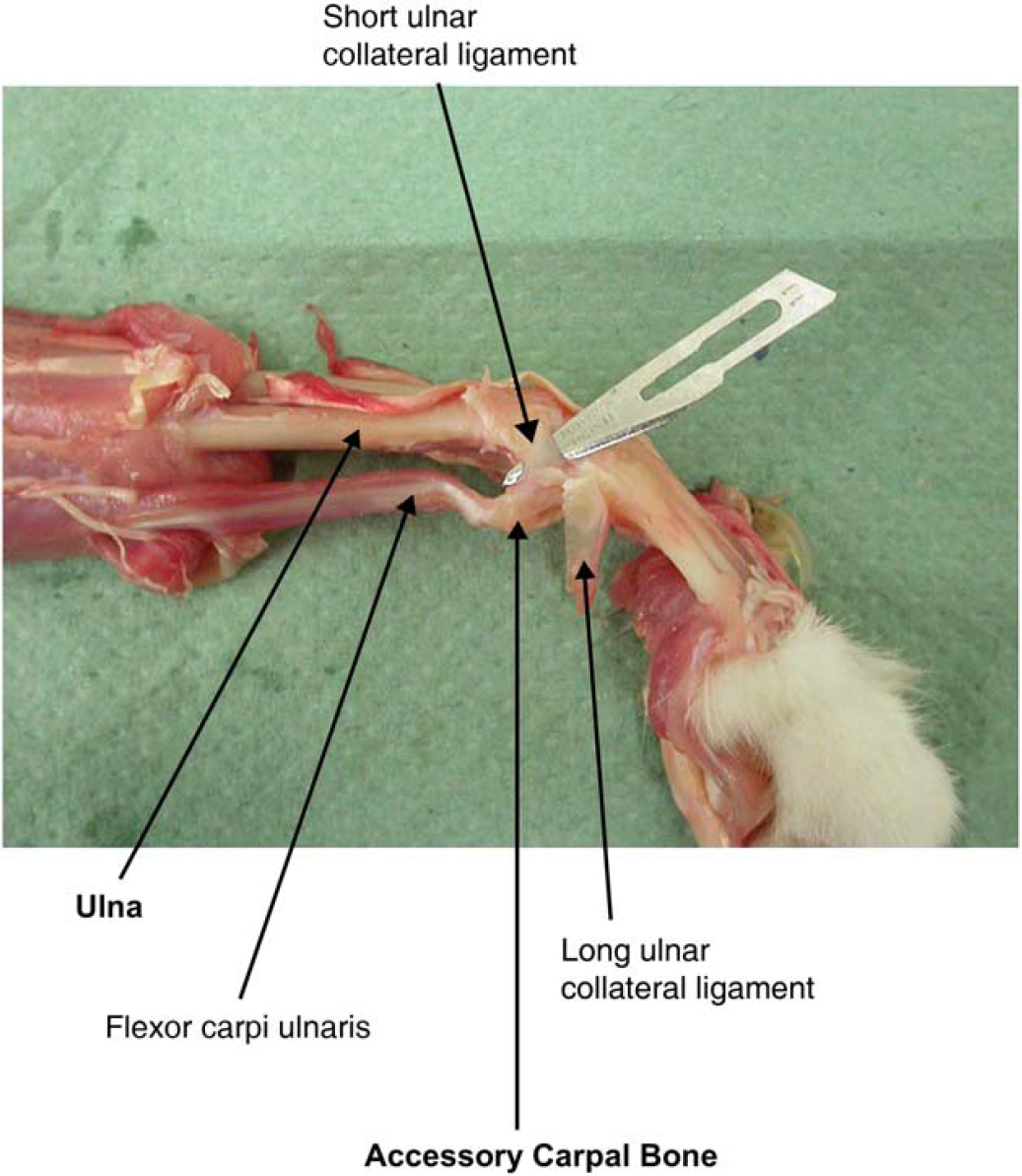
Anatomical dissection of the lateral collateral ligaments of the feline carpus (labelled according to Evans 1993).
Unlike the dog, conventional stressed radiographs and examination may not facilitate diagnosis of rupture of the feline medial collateral ligament (Voss et al 2003). Inward rotation of the paw and flexion of the carpus has been reported to cause palmar luxation of the carpus in the presence of medial collateral ligament insufficiency (Voss et al 2003). This difference may be a result of the absence of a straight medial collateral ligament in the cat (Fig 5). The dog possesses both straight and oblique medial collateral ligaments separated by the abductor pollicus longus muscle tendon (Voss et al 2003). No medial instability was present following reduction suggesting that the medial collateral ligament remained functional, although the possibility of a low-grade sprain, as was discovered at surgery, could not be excluded. Horizontal mattress sutures were used to stabilise the medial collateral ligament sprain as has been reported previously (Pitcher 1996).
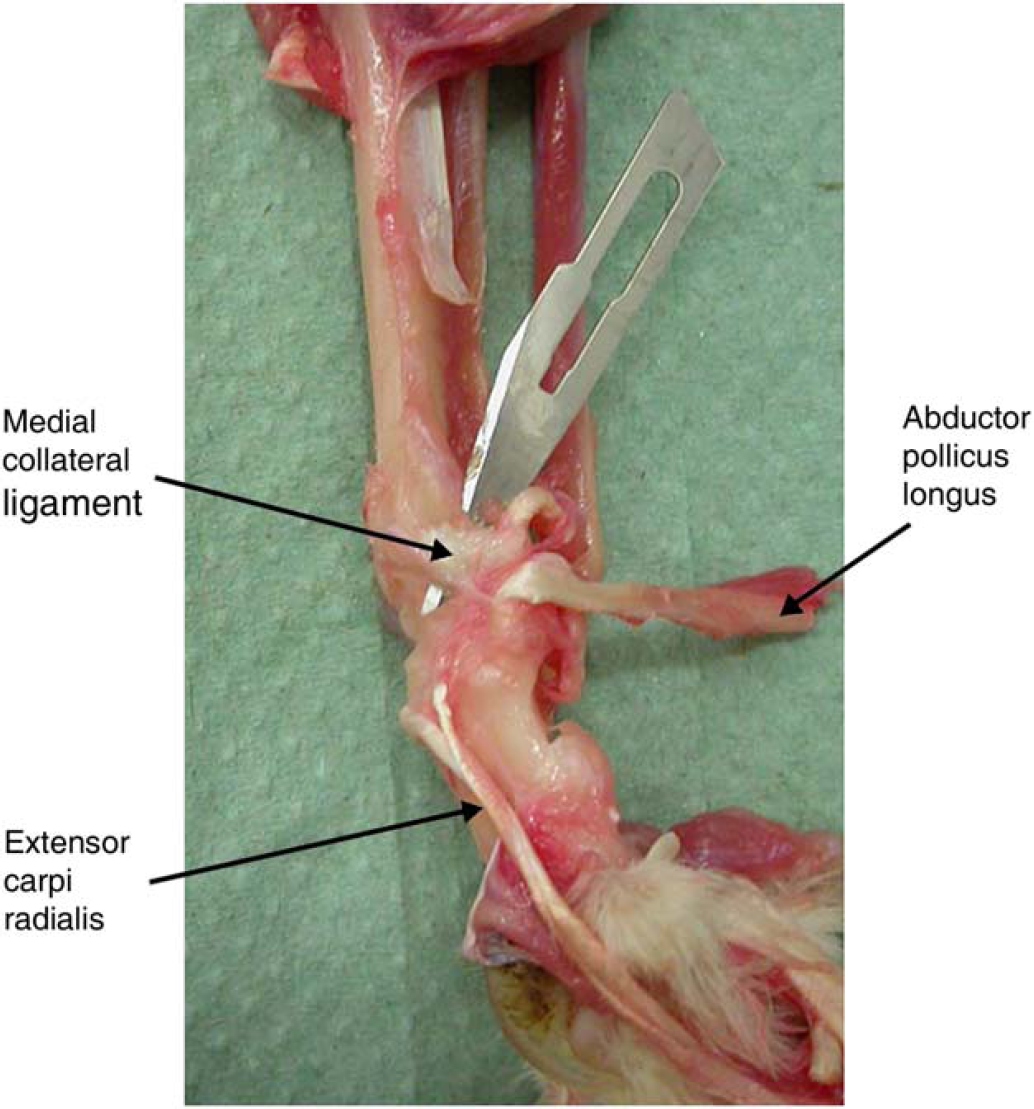
Anatomical dissection of the medial collateral ligament of the feline carpus. The straight collateral ligament present in the dog is absent in the cat. The abductor pollicus longus muscle tendon runs across the oblique medial collateral ligament and has been reflected in this dissection (labelled according to Evans 1993).
The presence of a ‘cranial-draw’ type motion and the direction of luxation suggested damage to the dorsal joint capsule (Voss et al 2003) with potential involvement of the dorsal radio-carpal ligament (Fig 3). The absence of carpal hyperextension suggested that damage to the palmar carpal ligaments was not severe, but low-grade sprains could not be ruled out.
The palmaro-lateral position of the accessory carpal (AC) bone following the dorso-medial antebrachiocarpal luxation in this case suggested damage to the ligaments between the AC bone and the proximal carpal and metacarpal bones (accessoro-metacarpal ligaments) (Fig 6). The flexor carpi ulnaris tendon remained intact and is likely to have contributed significantly to the maintenance of the AC bone's latero-palmar position with respect to the other carpal bones. Precise details of the severity of the accessoro-metacarpal ligament sprains were not obtained at surgery. Published information specific to the carpal ligaments of the cat is sparse and further work comparing the ligamentous anatomy of the feline carpus with that of the dog is warranted.

Anatomical dissection of the deep palmar ligaments of the feline carpus (labelled according to Evans 1993). The accessoro-metacarpal insertions on the proximal metacarpal bones IV and V are clearly seen.
Sutured ligament repairs require 3–6 weeks of rigid immobilisation in order to optimise healing (Frank et al 1983, Gomez et al 1989, Montgomery 1989). This was achieved by using a cranio-medial trans-articular type 1a K-E ESF as has been described in similar reports of carpal instability in the cat (Pitcher 1996). Mobilisation of the carpus by ESF removal was allowed at 5 weeks, which is similar to other reports (Pitcher 1996, Voss et al 2003). Following ESF removal, limb use deteriorated for several days. The authors commonly note a temporary deterioration in lameness for 24–48 h following unhinged trans-articular ESF removal. This may be the result of joint fibrosis and the discomfort caused by stretching of scar tissue with the sudden increase in range of motion.
The decision to leave the ‘A’-wire in place at 5 weeks was taken in order to maintain support during the maturation phase of healing of the unsutured radio-ulnar ligament in which suboptimal healing was expected. Removal of the ‘A’-wire at 7 weeks was performed in order to avoid possible implant breakage and/or migration and facilitate supination, which is considered an important component of normal feline limb function (Voss et al 2003).
To the authors' knowledge this is the first report of antebrachiocarpal luxation in the cat involving radio-ulnar ligament rupture. This case along with previous reports (Pitcher 1996, Voss et al 2003) suggests that severe palmar carpal ligament damage need not be associated with antebrachiocarpal luxation in the cat, and that primary repair of damaged ligaments may result in maintenance of carpal function.