
Abstract
A 12-year-old neutered male oriental shorthair cat was referred to the Animal Health Trust for investigation of pleural effusion. Ultrasonography revealed marked irregular thickening of the pleural surface of the cranial and caudal mediastinum. Cytological examination of the pleural fluid and fine needle aspirates of the thickened pleura suggested a diagnosis of mesothelioma. Following complete drainage of the thoracic cavity under ultrasound guidance, 180 mg/m2 carboplatin diluted in 60 ml sterile water was infused into the pleural space (30 ml in each hemithorax). This resulted in complete resolution of clinical signs for 34 days (having required thoracocentesis on four occasions in the preceding 4 weeks). The procedure was repeated using 200 mg/m2 carboplatin, and there was a further 20-day period where the cat was free of clinical signs. Further treatment was declined and the cat was euthanased 120 days after initial presentation. This is the first report of successful palliative chemotherapy for suspected feline mesothelioma and suggests that intracavitary carboplatin could be considered in tumours affecting the pleural cavity.
Mesothelioma is a rare usually malignant tumour arising from the mesodermal cells lining the pleural surfaces, peritoneum or pericardium. In humans, the major recognised risk factor for the development of mesothelioma is exposure to asbestos fibres, which is thought to account for 70–80% or more of cases (McDonald and McDonald 1996, Tomek and Manegold 2004), and as exposure is primarily by inhalation, the pleural form of disease is more common than the peritoneal form. Mesotheliomas are rarely reported in dogs and cats, and although some canine cases have been linked with asbestos exposure (Harbison and Godleski 1983, Glickman et al 1983), to date no predisposing causes have been identified in cats.
From an extensive literature search, the authors have been able to find nine previously reported cases of feline mesothelioma (Andrews 1973, Tilley et al 1975, Sugiyama et al 1977, Raflo and Nuernberger 1978, Akiyama et al 1982, Suzuki et al 1985, Schaer and Meyer 1988, Umphlet and Bertoy 1988, Kobayashi et al 1994), with a brief mention of three additional cases (Creighton and Wilkins 1975, Rostami et al 1994). Of the nine cases detailed, five were domestic shorthair cats and four were Siamese, with an age range of 18 months to 17 years (mean 8.4 years, median 9 years). In 10 cases the site of the mesothelioma was described and in contrast to humans, six of the 10 were the peritoneal form, three affected the pleura and one the pericardium. With the exception of a single case described as a ‘benign mesothelioma’ which may in fact have been benign mesothelial proliferation (Schaer and Meyer 1988) where repeated abdominocentesis was palliative for approximately 28 months, all the other cases described had a very short clinical course of disease with death or euthanasia occurring within days to a few weeks of the diagnosis, and clinical signs relating primarily to the rapid accumulation of fluid. Other than simple palliation with prednisolone (in two cases) and/or repeated fluid drainage, no treatment was attempted in these cats. In humans, this tumour also carries a poor prognosis, with treatment being regarded as palliative in most cases, and median survival times in the region of 5–17 months being reported (Boutin et al 1998, Tomek and Manegold 2004). There is no ‘standard’ treatment for human mesotheliomas, and therapy may include surgical resection, radiation therapy, and chemotherapy either alone or in various combinations. Attempted chemotherapy of feline mesothelioma has not been reported, although successful palliation has been reported in dogs (Moore et al 1991).
A 12-year-old neutered male oriental shorthair cat was referred to the Feline Unit at the Animal Health Trust for investigation of a 2-week history of progressive inspiratory dyspnoea and hyperpnoea accompanied by inappetence, lethargy and weight loss. Thoracic radiography undertaken by the referring veterinary surgeon had confirmed the presence of a pleural effusion, which had been drained on three occasions in the 2 weeks before referral. Fluid analysis had revealed a total protein of 43.3 g/l and an albumin content of 23.5 g/l. On physical examination at the time of referral the respiratory rate was 52 with mild inspiratory dyspnoea evident. Cardiac rate, rhythm, and auscultation were unremarkable and there was no pulse deficit. However, there were reduced lung sounds ventrally on auscultation and thoracic percussion revealed resonance ventrally. Results of routine haematology and serum biochemistry were all within normal limits, and screening tests for FeLV and FIV were negative. Radiography and ultrasonography were performed under general anaesthesia—this confirmed the presence of a bilateral pleural effusion and on ultrasonography there was extensive, severe irregular thickening of the cranial and caudal mediastinal pleura and surface of the pericardium, with numerous papillary-like projections from the mesothelial lining. The heart was within normal limits except for the changes on the surface of the pericardium. Thoracocentesis was performed and yielded a serosanguinous fluid with a total protein of 58 g/l, and fine needle aspirates were obtained from the thickened pleura.
Cytological examination of the pleural fluid sampled before referral, and at the time of referral (which contained nucleated cell counts of 6.0 and 2.9×109/l, respectively), and of the fine needle aspirates of the mediastinum, all revealed a similar population of abnormal cells (Figs 1 and 2). There were clusters of large pleomorphic round, oval or polygonal mesothelial cells displaying anisocytosis (diameters 4–12 times that of an erythrocyte). The nuclei, which were round-oval and eccentric, showed frequent anisokaryosis with variably coarse and clumped chromatin, there were some binucleate cells and mitoses evident, and a variable nuclear:cytoplasmic ratio (increased in some). Nucleoli were prominent and large (measuring greater than one erythrocyte in diameter). Samples of pleural fluid contained approximately 60% of these abnormal cells, with the remaining cells being a mixture of neutrophils, lymphocytes and macrophages. The appearance of the abnormal cells, the similar population of cells in the pleural fluid and fine needle aspirates of the thickened mesothelium, and the ultrasonographic appearance of the mesothelium all strongly suggested a diagnosis of pleural malignant mesothelioma.

Cytological appearance of the pleural fluid (stained with Giemsa)—see text for a description of the cells.

Cytological appearance of the pleural fluid (stained with Giemsa)—see text for a description of the cells.
Based on one previously published report involving three dogs with mesothelioma that suggested intracavitary cisplatin provided useful palliative therapy, extending both duration and quality of life in the dogs treated (Moore et al 1991), intracavitary carboplatin therapy was given, following thoracocentesis on two further occasions due to recurrent dyspnoea (Fig 3). Under general anaesthesia, bilateral thoracocentesis was performed with ultrasound guidance to remove as much of the pleural effusion as possible. Two sterile 18 g intravenous catheters were then placed transcutaneously into each hemithorax. A total of 48 mg of carboplatin (180 mg/m2) was diluted in 60 ml sterile water (from an initial concentration of 10 mg/ml) and 30 ml of the carboplatin solution was infused into each hemithorax. Following this the catheters were removed, and the cat was rolled gently to distribute the carboplatin solution. Supportive intravenous fluids were provided during anaesthesia and for 24 h afterwards. Following this therapy, the cat had complete remission of clinical signs for a 34-day period and gained more than 10% bodyweight (from 4.6 kg to 5.3 kg). However, dyspnoea recurred during the fifth week following therapy, and after thoracocentesis on two further occasions, carboplatin administration was repeated as above except that a total of 55 mg carboplatin (200 mg/m2) was administered. This produced a further complete remission of clinical signs for a 20-day period. Following this, the owners declined further intracavitary carboplatin therapy. Thoracocentesis was repeated on three further occasions before the cat was euthanased at the owners' request 120 days after initial presentation. Figure 3 shows the times and volumes of fluid removed from the cat by thoracocentesis. Results of blood samples collected from the cat before each of the two doses of carboplatin and 10 days afterwards all had normal haematology and serum biochemistry.
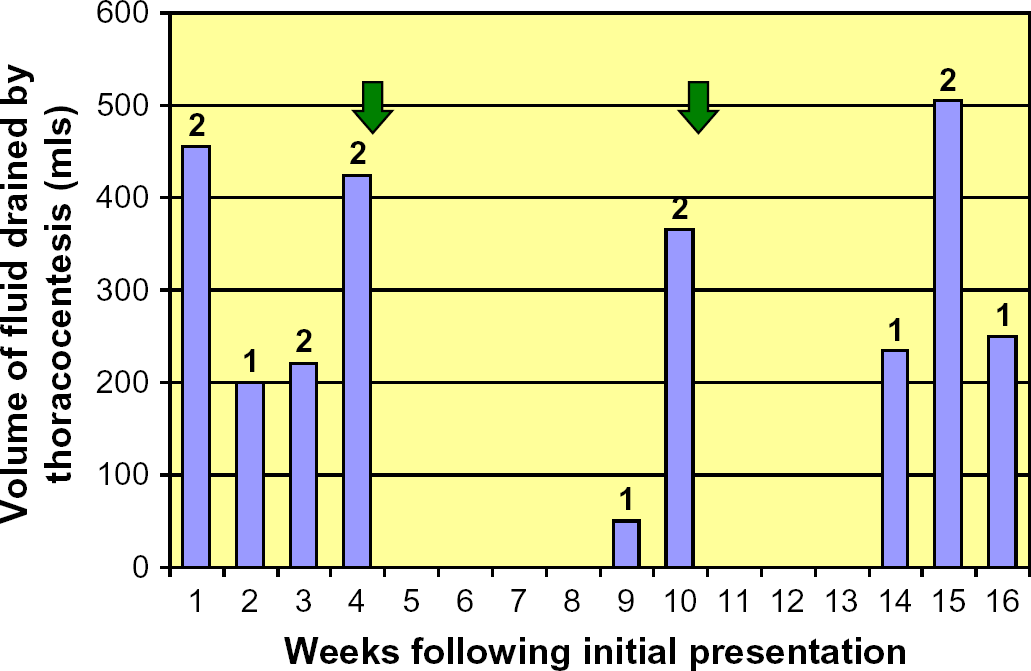
Weekly progress of the cat from presentation to euthanasia (120 days after initial presentation) volumes of fluid removed by thoracocentesis. Arrows indicate times that carboplatin was administered. Numbers above columns indicated number of times thoracocentesis was performed.
In this case, a post-mortem examination was not permitted and so the diagnosis of mesothelioma remained presumptive. However, although the difficulties in distinguishing reactive from neoplastic mesothelial cells are well known, in this cat the combination of ultrasonographic findings along with the fluid and fine needle aspirate cytologies were consistent with this diagnosis. Nevertheless, in the absence of tissue biopsy this remains a presumptive diagnosis, and it is conceivable that the apparent response seen in this cat was not in association with pleural mesothelioma.
In humans, treatment of mesothelioma is only considered palliative with generally poor responses irrespective of the treatment modality used (Tomek and Manegold 2004, Treasure and Sedrakyan 2004). Chemotherapy has been used extensively—systemic monotherapy with anthracyclines or platinum drugs generally produces response rates of up to 15% with median survival times of up to 8 months, and combination chemotherapy (using various regimes) does not generally appear to give substantially better results, with the possible exception of some newer regimes such as a combination of carboplatin or cisplatin and the anti-metabolite pemetrexed (Tomek and Manegold 2004). Surgery is rarely curative due to the widespread nature of the tumour, and has been used most commonly as a debulking procedure with the intention of improving the efficacy of other treatments, or in the palliative management of breathlessness. However, good evidence for the efficacy of surgery is lacking (Treasure and Sedrakyan 2004) and radical surgery can be associated with a high frequency of side effects. Although mesothelioma is a tumour that is radio-sensitive, its often widespread nature and proximity to structures such as the heart and spinal cord, make effective therapy using this modality problematic (Boutin et al 1998, Treasure and Sedrakyan 2004). Human mesothelioma is, therefore, a difficult tumour to treat, whatever therapeutic modalities are used, and there is a significant potential to compromise quality of life through inappropriate treatment (Treasure and Sedrakyan 2004).
In this case, we elected to offer intracavitary carboplatin as a trial therapy for the cat. This was based partly on the previous report of the use of intracavitary cisplatin in dogs with mesothelioma (Moore et al 1991), and partly on its use in humans with mesothelioma and other tumours (Markman et al 1986, Speyer and Sorich 1992). Although cisplatin has been used most widely for this purpose in both dogs and human beings, this drug is highly toxic to cats (Knapp et al 1987) and we therefore chose to use carboplatin, which has an established safety profile in cats (Hahn et al 1997, Fox 2000), and has also been used by this route in humans (Chambers et al 1997). A systemic dose rate of 200 mg/m2 has been recommended for clinical use in cats (Hahn et al 1997), but we reduced this dose by 10% for the first treatment in an attempt to avoid any adverse side-effects. For the second dose, having been extremely well tolerated initially, the full 200 mg/m2 was given. Based on knowledge of tumour biology and the experience of intracavitary chemotherapy in other species, this treatment was not given with curative intent, but with the hope of providing palliation and increased quality of life (Moore 1992). This is the first reported attempt to treat feline mesothelioma with chemotherapy, and to the authors' knowledge the first report of intracavitary chemotherapy in cats. Based on the complete remission of clinical signs seen following each administration of carboplatin (in comparison with the frequent thoracocentesis required prior to chemotherapy), the improved bodyweight, and the lack of side-effects associated with the treatment we conclude that palliation was achieved, albeit temporarily, and that intracavitary carboplatin should be considered for the management of mesothelioma or other tumours of the pleural cavity in cats.