
Abstract
A retrospective study was undertaken to determine the prevalence of different diseases in cats referred for investigation of chronic nasal disease, to identify historical, clinical and diagnostic features which may assist in making a diagnosis, and to provide information pertaining to outcome in these cats. Diagnoses included neoplasia (30 cases), chronic rhinitis (27), foreign body (8), nasopharyngeal stenosis (5), Actinomyces infection (2), nasal polyps (2), stenotic nares (2), and rhinitis subsequent to trauma (1). The most common neoplasia was lymphosarcoma (21 cases), with a median survival of 98 days for cats treated with multiagent chemotherapy. Cats with neoplasia were older on average than the other cats, and were more likely to be dyspnoeic and have a haemorrhagic and/or unilateral nasal discharge than cats with chronic rhinitis. Cats with neoplasia were more likely to have radiographic evidence of nasal turbinate destruction, septal changes, or severe increases in soft tissue density than cats with chronic rhinitis. It was unusual for cats with diseases other than neoplasia to be euthanased as a result of their nasal disease.
Introduction
Chronic nasal discharge and other signs of chronic nasal disease are frequently encountered in feline practice. A number of different underlying causes may be responsible for chronic nasal disease and establishment of a specific diagnosis is crucial to appropriate management. Clinical features and diagnostic investigations are used to make a definitive diagnosis but little information is available as to their value and accuracy. Common causes of nasal disease include infections (most commonly viral) which can lead to chronic rhinitis, neoplasia, trauma, foreign bodies, anatomical defects such as stenotic nares or cleft palate, oronasal fistula and dental disease (Levy and Ford, 1994). Nasopharyngeal conditions such as polyps or nasopharyngeal stenosis may lead to similar clinical signs, in particular stertor, and should be included in the differential diagnosis (Allen et al., 1999).
Diagnosis of specific nasal diseases relies on a combination of techniques including radiography, rhinoscopy, cytology, bacterial and fungal culture, and histopathology of biopsy samples. Suitable samples for histopathology can be obtained by a variety of techniques such as nasal flushes or mucosal brush, blind biopsies, endoscope-guided biopsies, and rhinotomy. Palpation and direct examination of the nasopharynx by endoscopy are considered useful techniques when investigating signs indicative of lesions in this region (Hunt et al., 2002).
There is little information available concerning the relative frequency of the different diseases, or the value of different diagnostic techniques. One study compared clinical signs in cats with nasal and nasopharyngeal disease (Allen et al., 1999), and other studies have provided information regarding the usefulness of specific diagnostic investigations for nasal disease (Caniatti et al., 1998, Michiels et al., 2003; O'Brien et al., 1996; Willard and Radlinsky, 1999).
The aims of the present study were to determine the prevalence of different diseases in a population of cats referred for the investigation of signs indicative of chronic nasal disease; to identify historical, clinical and diagnostic findings which may assist the clinician in making a diagnosis; and to provide information pertaining to outcome in these cats.
Materials and methods
Case records of cats referred to the University of Bristol for the investigation of nasal disease between 1997 and 2001 were reviewed. Inclusion criteria for the study were the availability of complete medical records, presence of signs of nasal disease for at least 3 weeks, and a definitive diagnosis. Seventy-seven cats were suitable for inclusion in the study.
Case records
Information was extracted from the case histories regarding signalment, environment, vaccination status, duration and type of clinical signs, response to any previous treatment, results of diagnostic investigations (including haematology, biochemistry, virology, radiography, endoscopy, and histopathology), diagnosis and treatment. Follow-up information was obtained by re-examination or by telephone contact with the referring veterinary surgeons or the cats' owners.
Virology
FeLV antigen and FIV antibody testing were performed in 66 cats (Petchek; Idexx). Virus isolation by cell culture for feline herpes virus 1 (FHV-1) and feline calicivirus (FCV) was performed in 22 cats using oropharyngeal or nasal swabs.
Radiography
Nasal radiographs were taken in 73 cases and were available for review in 71 cases. Radiographic views varied between cases but in most instances an intra-oral view of the nasal cavity was obtained. Other views were performed at the discretion of the attending clinician. For the purposes of the study radiographs were reviewed by one of the authors (KB), blinded to the final diagnosis. A grading system was used to determine the presence, absence and severity of radiographic changes. Changes in soft tissue density and turbinate destruction were recorded as unilateral or bilateral; mild, moderate or severe; and focal or diffuse. Septum and sinus changes were recorded as present or absent.
Endoscopy
Endoscopy was performed in 63 cases. Anterior rhinoscopy was performed where appropriate with a 2.7 mm diameter forward-viewing rigid endoscope (Panoview 8672.431; Wolf). Retroflexed views of the nasopharynx were obtained where appropriate using either a fibreoptic bronchoscope (BF 3C40, Olympus Keymed) or a 6.5 mm paediatric gastroscope (GIF-N30; Olympus Keymed).
Nasal flushes
Nasal flushes were performed in 18 cases by flushing of one or both sides of the nasal cavity via the nostril. A variety of techniques were used depending on clinician preference. Samples were submitted for cytology in 9 cases, for routine bacterial culture in 4 cases and for both procedures in 3 cases. In one case a foreign body was dislodged during the procedure.
Histopathology
Biopsies were obtained in 60 cases. Cup forceps were inserted into the nasal cavity either blindly, under endoscopic control adjacent to the rigid scope, or via the biopsy channel in the flexible endoscope. Nasal tissue was obtained at post-mortem in five cases. All samples were fixed in 10% neutral-buffered formalin, processed and embedded in paraffin wax. A four-micron section stained by haematoxylin and eosin was prepared for histopathological evaluation. Histopathological specimens were reviewed by one of the authors (MJD).
Diagnostic criteria
Neoplasia and polyps were confirmed histologically in all cases. Foreign bodies were identified radiographically or endoscopically and/or were retrieved from the cat. Nasopharyngeal stenosis was identified endoscopically. A diagnosis of stenotic nares was made on clinical examination. Criteria for a diagnosis of chronic rhinitis included a histopathological diagnosis of rhinitis with no evidence of a definitive underlying cause for the disease (e.g. neoplasia, trauma, foreign body, Actinomyces infection).
Statistical analysis
For descriptive purposes the cats were divided into five groups (neoplasia, chronic rhinitis, foreign body (FB), nasopharyngeal stenosis (NPS) and miscellaneous). For comparative purposes NPS cats were included in the miscellaneous group.
Statistical analysis was performed using a commercially available package (SPSS for Windows; SPSS Inc). One-way ANOVA was used to compare continuous variables with a normal distribution. Chi-squared or Fisher's exact tests were used to compare sex, breed, clinical signs, and results of diagnostic tests between groups. Results were considered significant when P<0.05.
Results
The cats ranged from 6 months to 19 years of age (mean 7.7±4.1 years). There were 34 female cats and 44 male cats. Fifty-seven of the cats were non-pedigree (48 domestic short-haired, 9 domestic long-haired). Twenty of the cats were pedigree, of which the most common breeds were Siamese (8 cats) and Persian (4 cats). Duration of clinical signs prior to presentation ranged from 21 days to 10 years with a median of 120 days.
The most common diagnosis was neoplasia (30 cases) (Fig. 1). The second most common diagnosis was chronic rhinitis (27 cats). Eight cats were diagnosed with foreign bodies, 5 cats with nasopharyngeal stenosis, 2 with rhinitis associated with Actinomyces infection, 2 with nasal polyps, 2 with stenotic nares, and 1 with rhinitis as a consequence of trauma.

Aetiology of nasal disease in 77 cats.
The most common clinical signs associated with the different diagnoses are summarised in Tables 1a and 1b. Haematological and biochemical findings were generally non-specific and did not help differentiate disease conditions (data not shown).
Neoplasia
Cats with a diagnosis of neoplasia ranged from 4–19 years (mean 10.3±3.2 years). Sixteen of 30 cats were female. Twenty-six of 30 cats were non-pedigree and 4 were pedigree (3 Siamese and 1 Havana). Duration of clinical signs varied from 28–540 days (median 60 days). Twenty-nine cats had previously received treatment with antibiotics, glucocorticoids or both. Antibiotics were reported to have been helpful in 7 cases, glucocorticoids in 5 and both in 3 cases. Three of 25 cats were antibody positive for FIV and one of 25 cats was antigen positive for FeLV. No cat was co-infected with FIV and FeLV. All six cats tested were negative for FCV and FHV-1. Clinical signs are summarised in Tables 1a and 1b.
Clinical signs in cats with different categories of nasal disease

Percentage of group affected shown in brackets.
P values <0.05.
Nature of nasal discharge in cats with nasal disease
Percentages of cats in each group shown in brackets.
P values <0.05.
Type of discharge not recorded in 1 cat.
Side of discharge not recorded in 1 cat.
Nasal radiographs were performed in 27 cases and were available for review in 26 cases. Abnormalities were noted in all 26 cases and are summarised in Tables 2a and 2b. Endoscopy was performed in 23 cases. No abnormalities were noted in one case, and discharge obscured the mucosa in 2 cases. Hyperaemia was noted in 4 cases and a mass was seen in 16 cases (Fig. 3). Flushing was performed in 5 cases; cytology was suggestive of rhinitis in one case and of lymphoma in another. In 2 cats with lymphoma a mass was dislodged during the flushing process and was submitted for histopathological examination. In the fifth case flushing failed to dislodge any tissue and no samples were submitted.
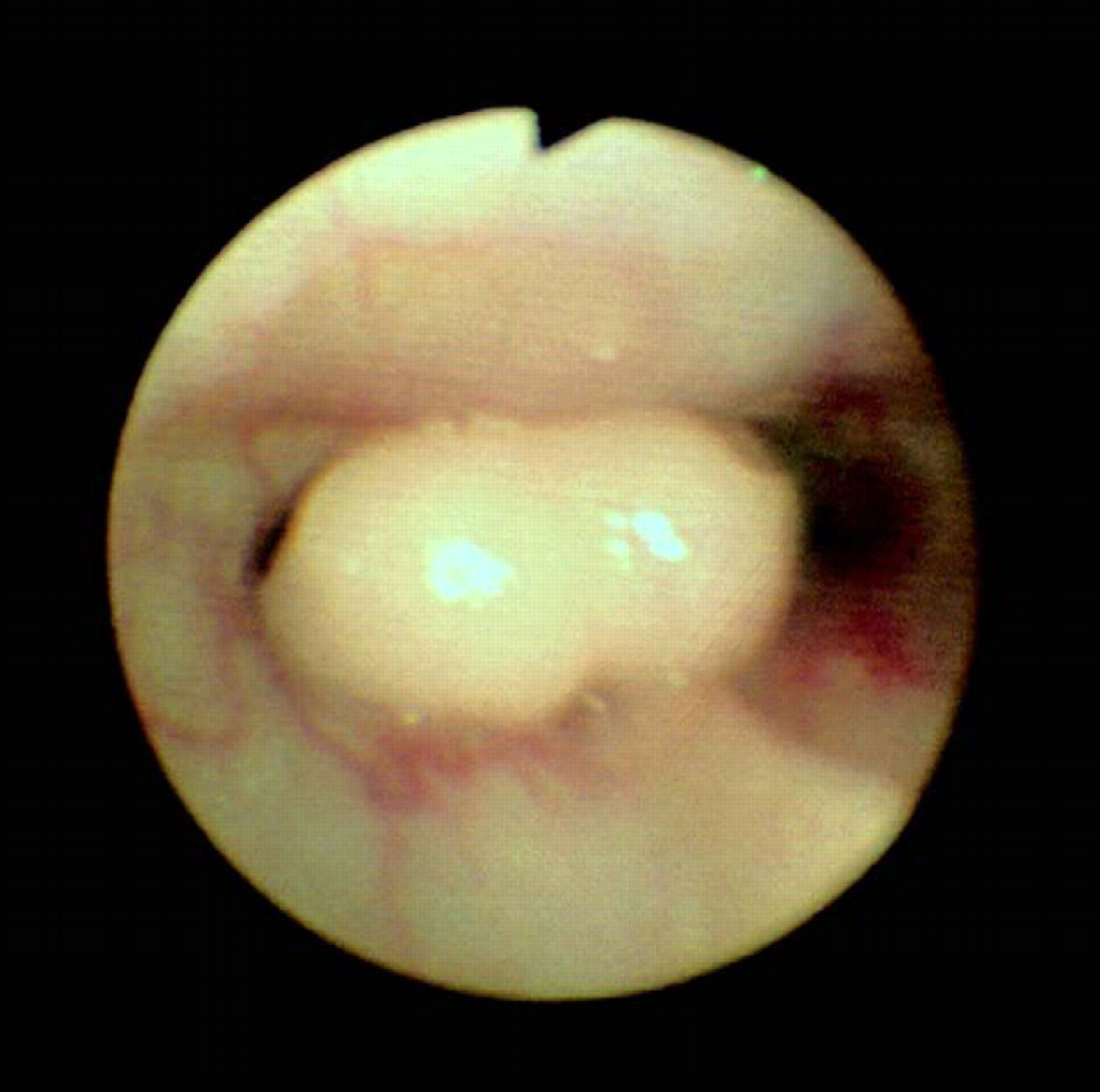
Endoscopic view of nasal lymphoma in a cat, obtained by retroflexing the endoscope in the nasopharynx.
Nasal radiographic changes in cats with nasal disease
Percentages of cats in each group shown in brackets.
P values <0.05.
Severity of nasal radiographic changes in cats with nasal disease

Percentages of cats in each group shown in brackets.
P values <0.05.
Diagnosis was obtained by biopsy (27 cases) or by post mortem (3 cases). Twenty-one cats were diagnosed with lymphoma, four with adenocarcinoma, two with carcinoma, and one of each of squamous cell carcinoma, sarcoma and fibrosarcoma.
Of the cats with lymphoma, six were euthanased at the time of diagnosis, one received no treatment (following debulking by nasal flush), four received palliative prednisolone, and 10 received multiagent chemotherapy (typically a cyclophosphamide/vincristine/prednisolone protocol). Of the cats with other forms of neoplasia, two received prednisolone. Radiation therapy was later used in one cat with lymphoma when chemotherapy was no longer effective. At the time of writing three cats were still alive, 24 had died as a result of nasal disease, two had died due to other causes and one was lost to follow-up (Table 3). Median survival for cats with lymphoma which were treated with multiagent chemotherapy was 98 days (range 10 days to >1264 days) compared to 28 days (range 10–130 days) for cats who received no treatment or prednisolone alone. Median survival for cats with other forms of neoplasia was 100 days (range 0 days to >880 days).
Outcome in cats with nasal neoplasia

COP = cyclophosphamide, vincristine, prednisolone; WM = modified Wisconsin–Madison protocol; LMP = leukeran, methotrexhate, prednisolone
Chronic rhinitis
Twenty-seven cats were diagnosed with chronic rhinitis, ranging from 0.5–13 years in age (mean 6.4 years±3.7 years). Eighteen of 27 cats were male and 17 of 27 cats were non-pedigree. Pedigree breeds included three Siamese cats and two Persians. Clinical signs had been present from 42 to over 3600 days prior to referral (median 210 days). Clinical signs are summarised in Tables 1a and 1b.
All cases had received previous treatment with antibiotics, glucocorticoids or both. In 14 cases some response had been noted to antibiotic therapy. Response was not known in six cases. Two of 27 cats were FIV antibody positive, two of 11 cats were FCV positive, and two of 11 cats were FHV-1 positive. None was FeLV antigen positive, and there were no co-infections. Radiographic changes are summarised in Tables 2a and 2b. Endoscopy was performed in 25 cases. No abnormalities were found in 3 cases, excessive discharge prevented full examination in 5 cases, and signs of mucosal inflammation were noted in 17 cases. Masses were not seen in any cases. Nasal flushing was performed in 7 cases; cytology performed in 4 cases showed evidence of inflammation. Bacterial culture was performed in the other 3 cases; 1 was positive for Bordetella bronchiseptica and the other 2 had no growth on routine bacteriology. The latter 2 cases had been treated previously with antibiotics.
Cases were treated at the discretion of the attending clinician, most commonly with antibiotics (22 of 27 cases). The most commonly used antibiotic was amoxycillin/clavulanic acid (16 cats), with the remaining cats being prescribed a variety of other antibiotics including cephalexin, clindamycin, enrofloxacin and doxycycline. Two cats were discharged on no treatment, with recommendations that antibiotics be used if signs became more severe. One cat had previously responded to glucocorticoid therapy and was discharged on prednisolone—the cat was euthanased for reasons not pertaining to its nasal disease over 3 years later. One cat was euthanased due to a concurrent severe hepatopathy and one was euthanased under general anaesthetic at the owner's request, due to severity of disease and suspicion of neoplasia, based on clinical and radiographic findings.
Follow up information was obtained for 24 of the 25 cats that were discharged. One cat with severe disease and weight loss was euthanased due to its nasal disease 8 days following discharge. Six cats died for reasons not relating to their nasal disease 240–1365 days following diagnosis (median 715 days) and one cat died of unknown causes after 1335 days. One of these had still been receiving intermittent courses of antibiotics. Information regarding response to treatment for nasal disease was not available for the others. Sixteen cats were still alive at the time of writing, with time since diagnosis ranging from over 270 to over 1550 days (median 728 days). Eleven cats were still symptomatic, some intermittently. Five of these cats received intermittent courses of antibiotics whilst the other 6 were not on any treatment. In 3 cats the condition appeared to have resolved. Two of these had received treatment with amoxycillin/clavulanic acid and the other had received cephalexin. Details regarding subsequent treatment were not available for 2 cats.
Foreign bodies
Foreign bodies (FB) were found in 8 cats, ranging in age from 7 months to 13 years (mean 5.8 years±4.5 years). Five of the cats were female and only 1 was a pedigree (Siamese). Duration of clinical signs ranged from 21–540 days (median 135 days). Clinical signs are summarised in Tables 1a and 1b. None of the 5 cats tested were positive for FIV antibody or FeLV antigen.
Presence of a foreign body was diagnosed by radiography in 3 cases (needle, stone, airgun pellet), endoscopy in 2 cases (grass blades), nasal flush in 1 case (grass blade) and blind exploration with forceps in one case (grass seed). In the other case diagnosis was confirmed several weeks following onset of nasal discharge when a grass seed emerged from an abscess overlying the cat's frontal sinus. The needle (Fig. 4) was removed by fluoroscopic guidance, and the airgun pellet by ventral rhinotomy. The two grass blades seen endoscopically were retrieved with forceps. It was not possible to remove the stone endoscopically; the cat suffered a hypoxic episode under general anaesthetic and was euthanased 3 days later. The remaining 7 cats are alive and well at the time of writing (365–2079 days later).

Radiograph of needle foreign body in the nasal cavity of a cat.
Nasopharyngeal stenosis
Five cats were diagnosed with NPS ranging in age from 1.5–9 years (mean 5.3 years±3.2 years). Three were female. Two were pedigree (1 Burmese and 1 Birman). Duration of clinical signs ranged from 180–1800 days (median 365). Increased upper respiratory tract (URT) noise was a feature in all 5 cats whilst nasal discharge was only reported in one cat. Three cats tested were negative for FIV/FeLV and 2 cats tested were negative for FCV and FHV-1. Radiographic findings are summarised in Tables 2a and 2b. Endoscopy was performed in all 5 cats—the procedure was diagnostic in 4 cats but in 1 cat the nasopharynx was obscured by mucus. Four weeks later, following antibiotic therapy, rhinoscopic examination was repeated and the diagnosis was confirmed. Nasal flushes were performed in 2 cats—cytology and culture (including fungal culture in 1 cat) were unremarkable. Nasal biopsies were obtained in 2 cases; 1 had a severe mixed rhinitis and 1 had evidence of granulation and chronic haemorrhage without significant inflammation.
Four cats had the stenosis dilated with forceps (Fig. 5). One cat initially improved but relapsed 4 weeks later. At this stage surgery was performed via the soft palate to resect the fibrosed tissue; the cat was reported to be very well at the time of writing (790 days). One cat was still showing intermittent clinical signs and receiving courses of antibiotics (940 days since diagnosis). One cat was killed in a road accident at 515 days. The fourth cat was reported to be doing very well (455 days). In the fifth cat the clinical signs were considered to be very mild and treatment was restricted to intermittent antibiotics; the cat still had increased URT noise 605 days later.
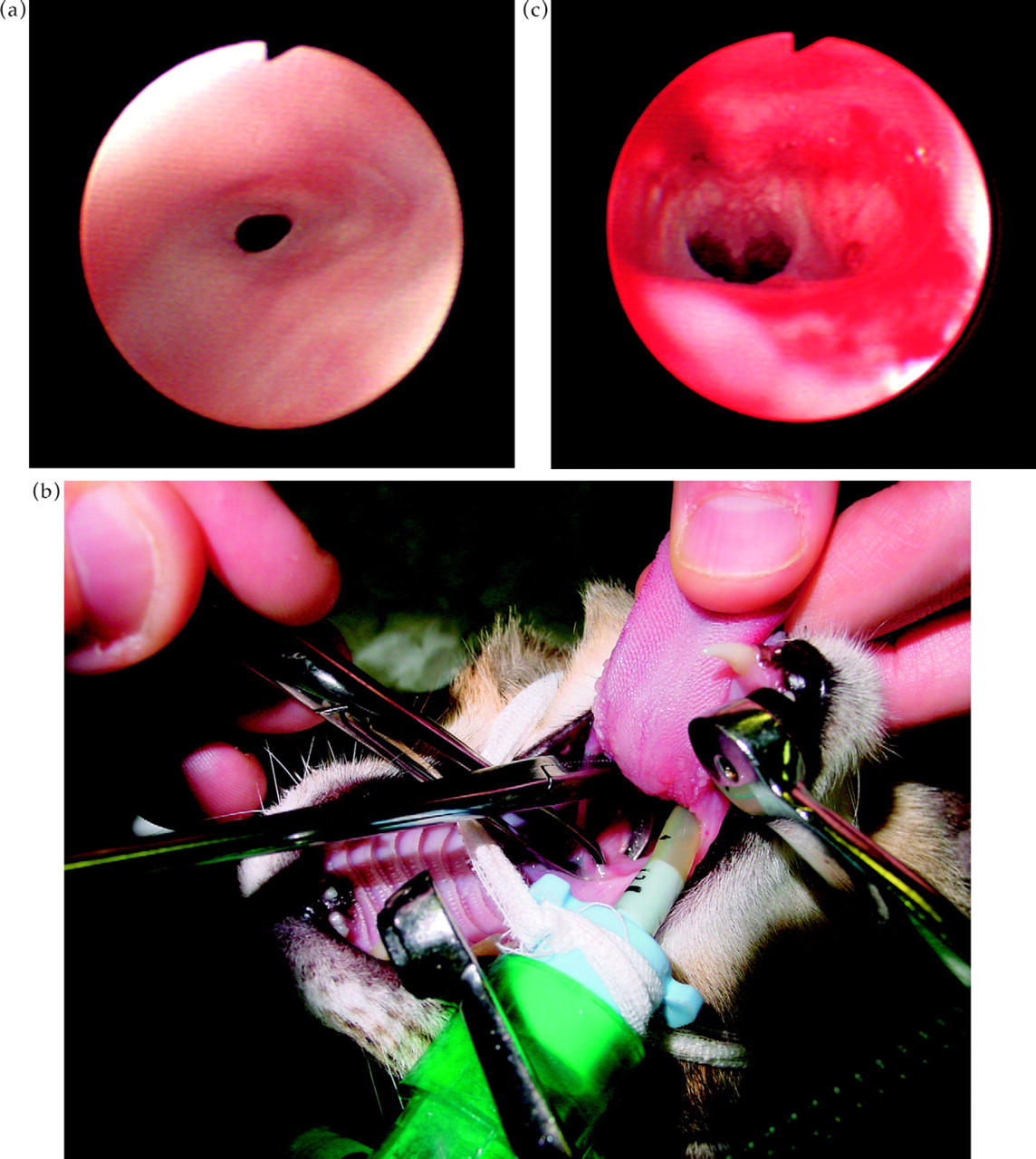
(a) Endoscopic view of nasopharyngeal stenosis in a cat, obtained by retroflexing the endoscope in the pharyngeal region. (b) Procedure used for dilation of nasopharyngeal stenosis with artery forceps. (c) Endoscopic view of nasopharynx post dilation of nasopharyngeal stenosis.
Miscellaneous
Seven cats were diagnosed with disease that did not fit into the other categories. In two cases (aged 5 and 12 years) club-colony-forming organisms were seen on histopathological examination, suggestive of infection with Nocardia or Actinomyces spp. In both cases a severe rhinitis was noted histologically. Radiographic changes were moderate-severe. In one case an Actinomyces (sp.) was cultured—this cat responded well to treatment with surgical curettage of the frontal sinus and penicillin V with no recurrence 1730 days later. The other cat was FIV antibody positive; culture did not yield any organisms. Treatment with amoxycillin/clavulanic acid was instituted and repeat biopsies 4 weeks later did not show any organisms. The cat was euthanased due to progression of clinical signs (anorexia and nasal swelling) 3 months later.
The two cats with nasal polyps were 7 and 10 years old. Both polyps originated in the nasal cavity. One of these extended into the nasopharynx but could not be removed by traction per os. The cat was taken to surgery and the polyp was confirmed to be nasal in origin. Diagnosis was confirmed on histopathological examination. This cat also had otitis media/interna that failed to improve. The cat was euthanased due to renal failure 2 months later. In the other case inflammation but no mass was seen with anterograde rhinoscopy. This cat's clinical signs were a consequence of trauma. Flushing the nasal cavity demonstrated a connecting sinus between the nasal cavity and frontal sinus. The cat was taken to surgery and polypoid material removed via rhinotomy. At the time of writing the cat was reported to be well (395 days later).
Two young Persians (9 and 12 month old) were both diagnosed with stenotic nares. Nasal biopsies were obtained in one of these cats and demonstrated mild acute rhinitis. One was FCV positive. No treatment was given to either of these cats and there had been no progression of the disease 760 and 1335 days later.
One five year old cat had a history of nasal disease since being involved in a road accident 3 months previously. Nasal biopsies demonstrated severe mixed rhinitis. Antibiotic treatment did not provide a significant improvement and the cat was euthanased 790 days later due to progressive disease.
Statistical analysis
The cats with neoplasia were significantly older than the other cats with a mean age of 10.3 years (Fig. 2) compared to 5.6 years (miscellaneous, P = 0.002), 5.8 years (FB, P = 0.014), and 6.4 years (chronic rhinitis, P = 0.001). There were no significant differences in sex or breed between groups, although there was a trend for more non-pedigree than pedigree cats to have chronic rhinitis compared to neoplasia (P = 0.063). The duration of clinical signs prior to referral was shorter in the cats with neoplasia compared to those with chronic rhinitis (P = 0.007). There were no significant differences in vaccination status or access to outdoors (data not shown).

Box-and-whisker plot showing ages of cats with different diagnoses.
The only significant differences in clinical signs between groups were increased frequency of dyspnoea in the cats with neoplasia compared to the cats with chronic rhinitis (P = 0.013) and a greater frequency of increased URT noise in the cats with neoplasia compared to the cats with foreign body (P = 0.016). Cats with dyspnoea were 9 times more likely to have neoplasia than chronic rhinitis, and cats with increased URT noise were 23 times more likely to have neoplasia than a FB. There was a trend for increased URT noise in the cats with neoplasia compared to those with chronic rhinitis (P = 0.19). Nasal discharge was more likely to be unilateral in cats with neoplasia compared to cats with chronic rhinitis (P = 0.006); cats with unilateral discharge were 2.7 times more likely to have neoplasia than chronic rhinitis. The type of discharge was significantly different between cats with neoplasia or chronic rhinitis; it was more likely to contain blood in the cats with neoplasia (P = 0.046) and to be mucopurulent in the cats with chronic rhinitis (P = 0.045). Cats with haemorrhagic discharge were 2.2 times more likely to have neoplasia than chronic rhinitis, and cats with mucopurulent discharge were 1.7 times more likely to have chronic rhinitis than neoplasia.
There were no significant differences in results of virological, haematological or biochemical analysis.
When compared to cats with chronic rhinitis, cats with neoplasia were more likely to have evidence of turbinate destruction on radiographs (P = 0.009) (Fig. 6). Cats with turbinate destruction were 1.5 times more likely to have neoplasia than chronic rhinitis. Septal changes were more common in cats with neoplasia than cats with chronic rhinitis (P = 0.004). Cats with septal changes were five times more likely to have neoplasia than chronic rhinitis. Although there was no significant difference in the number of cats with soft tissue changes between groups, cats with neoplasia had more severe soft tissue changes than cats with chronic rhinitis (P = 0.001). Of 13 cats with severe soft tissue changes, 85% were diagnosed with neoplasia and none with chronic rhinitis. There were no significant differences in unilateral/bilateral or focal/diffuse changes, or severity of turbinate destruction. A mass lesion was more likely to be seen during endoscopy in cats with neoplasia compared to the other groups (P<0.001). Of 18 cats in which masses were seen, 89% were diagnosed with neoplasia.

Radiographic changes in cats with nasal disease.
Cats with neoplasia were more likely to be euthanased as a result of their nasal disease than cats with chronic rhinitis (P<0.001) or foreign bodies (P = 0.001).
Discussion
To the authors' knowledge, there are no previous reports of the relative frequency of different aetiologies of nasal disease in cats. Neoplasia and rhinitis have previously been reported as the commonest causes of chronic nasal disease in the dog (Tasker et al., 1999). A retrospective study of nasopharyngeal disease in 53 cats found that 49% had lymphoma and 28% had polyps (Allen et al., 1999); however this study was restricted specifically to nasopharyngeal lesions.
The referral nature of the population of cats in this study probably influenced the frequency of diagnosis of different diseases, excluding some such as dental disease and oronasal fistulae which may be readily diagnosed in first opinion practice. Nasopharyngeal polyps are also considered a significant cause of chronic signs of upper respiratory tract disease in cats but were lacking in this study. It is probable that these would be more common in cats in first opinion practice, and their absence in this study reflects that they are more readily diagnosed in general practice. Whilst this population bias may be viewed as a limitation, the advantage of studying a referral population is that the more extensive investigations undertaken allow stringent diagnostic criteria to be applied.
Of the 30 cats diagnosed with neoplasia, the commonest tumours in this study were lymphoma (70%) and adenocarcinoma (13%), which is in agreement with a previous retrospective study of 123 cats with nasal neoplasia (Mukaratirwa et al., 2001). Adenocarcinoma and carcinoma were the most common nasal tumours in another study of 16 cases, in which only one cat was diagnosed with lymphoma (Cox et al., 1991). The reason for the disparity between these results is not clear but the relatively small sample size in the latter study may be a factor.
Chronic rhinitis is generally considered a consequence of prior infection with either FHV-1 or FCV (Van Pelt and Lappin, 1994). Up to 80% of cats that recover from acute viral upper respiratory tract infections are likely to become chronic carriers which can lead to persistent clinical signs (Gaskell and Wardley, 1977). In addition, viral infection causes bony and severe mucosal injury to the turbinates, which can predispose to secondary bacterial infection. Although previous viral infection may be the underlying cause in most cases, isolation at the time that cats are referred with chronic signs gives inconsistent results. Isolation of URT viruses does not prove their involvement in the current disease process (Hawkins, 1998). Bordetella bronchiseptica was isolated from one case and has been reported as a primary and secondary pathogen in cats with URT disease (Speakman et al., 1999). However the significance of infection in the case reported here is unclear and the cat was not excluded from the rhinitis group.
Rhinitis in association with Actinomyces/Nocardia infection has been reported previously in two cats (O'Brien et al., 1996). In our study these cats were excluded from the chronic rhinitis group as the presence of these organisms was considered a significant factor in the progression of the disease.
There were no cats in our study diagnosed with fungal infections such as cryptococcosis or aspergillosis. Although culture was not routinely performed, lesions with a histopathological appearance of granulomatous inflammation were routinely investigated further with a panel of special stains including periodic acid schiff (PAS). Therefore it seems unlikely that fungal diseases were overlooked, particularly since these infections are usually progressive. In countries such as Australia where fungal infection is more common, further diagnostics such as latex cryptococcal antigen test should be considered (Hunt et al., 2002).
Nasopharyngeal stenosis has been described in cats usually following an inflammatory condition of the URT (Glaus et al., 2002; Griffon and Tasker, 2000; Mitten, 1988; Novo and Kramek, 1999) and is an important differential in cats with progressive upper airway disease, especially when nasal discharge is minimal and increased URT noise is present.
Small sample sizes in the groups other than neoplasia and chronic rhinitis limited statistical analysis, and it is possible that other significant findings would have been apparent with more cases.
Older cats were rarely presented with diseases other than neoplasia which, although not an unexpected finding, does not appear to have been previously reported. The shorter duration of clinical signs prior to referral in cats with neoplasia compared to cats with rhinitis may suggest a more rapidly progressive disease pattern.
A male predominance has previously been reported in cats with neoplasia (Mukaratirwa et al., 2001) but was not apparent in this study. In a previous study Siamese cats were found to have an increased frequency of rhinitis compared to the overall hospital population (Cape, 1992). Although not compared with overall hospital data, there were no significant differences in sex or breed between the groups in the present study.
Clinical signs were not pathognomonic for any disease but certain features can be useful to increase the index of suspicion for a particular condition. Unilateral nasal discharge and evidence of haemorrhage were both more than twice as common in cats with neoplasia than cats with rhinitis, an observation that is in agreement with other authors (Hawkins, 1998). However, 8/27 (30%) of the cats with rhinitis and 5/8 (63%) of the cats with foreign bodies also had unilateral discharge. Previous reviews of chronic rhinitis have also indicated that a proportion of cats with chronic rhinitis have unilateral discharge (Cape, 1992; Michiels et al., 2003). Increased URT noise was much more common in cats with neoplasia than foreign bodies, and tended to be more common in cats with neoplasia than those with rhinitis although this did not reach significance. Changes in facial shape have previously been reported to be more common in neoplastic or fungal disease (Hawkins, 1998). Facial changes were seen in small numbers of cats in the present study, most commonly with neoplasia but also with rhinitis, foreign bodies, polyp and suspected Actinomyces infection.
Abnormalities detected on routine haematology/biochemical testing were non-specific and were not useful in identifying the cause of the nasal disease.
Radiographic evidence of turbinate destruction and septal changes were more common in cats with neoplasia than rhinitis, in agreement with previous findings (O'Brien et al., 1996). Although there was no difference in frequency of increased soft tissue density in the nasal chambers between groups, cats with neoplastic disease had more severe changes than those with rhinitis. In this study one cat was euthanased based on radiographic and clinical suspicion of neoplasia but diagnosed with rhinitis at post-mortem. O'Brien et al. (1996) noted that 2 cats in their study with evidence of Actinomyces/Nocardia infections showed signs of severe disease radiographically; this was also apparent in the two cats in our study. In many of the cases in the present study in which the discharge was unilateral, the radiographic findings suggested bilateral involvement. Although radiography can provide clues as to underlying disease, it does not provide a specific diagnosis and further investigations including biopsies are required to make a definitive diagnosis. Computed tomography (CT) has been evaluated for the investigation of nasal disease in cats, and is considered more sensitive than radiography for determining locality and extent of lesions (Schoenborn et al., 2003).
Focal masses seen on endoscopy proved to be either neoplasia or polyps. Given that polyps may be more common in first opinion practice, the importance of obtaining biopsies is again emphasised. Mass lesions were not identified in any of the cases diagnosed with rhinitis, which differs from another study in which 2/12 cats with masses found on endoscopy were diagnosed with chronic rhinitis (Willard and Radlinsky, 1999). Endoscopy was also important in identifying nasopharyngeal stenosis. In 11 of the 63 cases where endoscopy was performed, examination was limited by excessive discharge. Vigorous flushing with saline may help overcome this problem (Hunt et al., 2002).
Nasal flushing was performed in a limited number of cases and thus it is difficult to assess its usefulness as a diagnostic test. Vigorous nasal flushing can be useful to dislodge mass lesions or foreign bodies (Hunt et al., 2002). Cytology of nasal flushes is likely to be very superficial and of limited value. In particular neoplastic conditions may be misdiagnosed as rhinitis following the finding of inflammatory cells only on cytology (Caniatti et al., 1998), and chronic inflammation may be diagnosed as acute based on cytology (Michiels et al., 2003). Culture was performed on relatively few of our samples and this procedure is considered of limited value by some (Hawkins, 1998). However, others suggest that results of culture and sensitivity testing may be useful in guiding antibacterial therapy (Cape, 1992; Michiels et al., 2003).
Histopathology was considered to be the key test for a diagnosis of neoplasia and to rule out other potential causes of disease in cats with chronic rhinitis. Radiographic and endoscopic findings were rarely specific apart from in cats with NPS or foreign bodies.
Cats with neoplasia were significantly more likely to be euthanased as a result of their nasal disease than cats with other forms of nasal disease. Lymphoma was the most common nasal tumour, and was amenable to therapy in several cases, with survival of over 4 years in one cat. Since follow-up examinations were generally performed by the referring veterinary surgeons, and ongoing treatment protocols varied it was not feasible to assess remission times or response rates. Consequently the only outcome measurement recorded was survival time.
Median survival of cats with nasal lymphoma which received multiagent chemotherapy were shorter than reported in another recent study (Teske et al., 2002), but both studies were based on a small number of cats. Survival times of 8 months to more than 4 years in four of the treated cats was encouraging, and further investigation of responses to different chemotherapy protocols and radiation therapy is warranted. Radiation therapy has been recommended in cats with lymphoma (Elmslie et al., 1991; Straw et al., 1986) but was not readily available at the referral centre where the current study was based.
There were too few cats with non-lymphoid tumours to draw any meaningful conclusions regarding survival. Median survivals in cats with non-lymphoid tumours which have received radiotherapy have been reported as 382 days (Mellanby et al., 2002) and 330 days (Theon et al., 1994).
In the only two cats with chronic rhinitis which were euthanased as a result of their nasal disease this was done within 8 days of referral. Clinical signs persisted in the majority of cases with only three owners reporting resolution of clinical signs. However the disease did not appear to be progressive and owners seemed to accept that their cats would have ongoing problems.
A variety of techniques have been described to treat nasopharyngeal stenosis including bougienage, surgery via the soft palate (Mitten, 1988), use of a mucosal advancement flap (Griffon and Tasker, 2000), balloon dilation (Boswood et al., 2003; Glaus et al., 2002) and use of a stent (Novo and Kramek, 1999). In our study three of four cats clinical signs resolved following dilation of the stenosis with forceps. One cat showed recurrence of clinical signs severe enough to warrant a surgical approach.
Footnotes
Acknowledgement
The authors would like to thanks their colleagues who were involved in the investigation of some of the cases included in this study, Emma Opperman for her help with obtaining follow-up information, and Dr Andy Sparkes for his helpful comments on the manuscript. SMAC is supported by the Feline Advisory Bureau. ST holds a position funded by Royal Canin/Waltham.