
Abstract
A technology for electrical detection of protein biomarkers has been developed. It is based on developing high-density, low-volume multiwell plate devices. The scientific core of this technology lies in integrating nanoporous membranes with microfabricated chip platforms. This results in the conversion of individual pores into wells of picoliter volume. Specific antibodies are localized and isolated into individual wells. The formation of the antibody–antigen-binding complex occurs in individual wells. The membrane allows for robust separation among individual wells.
This technology has the capability to achieve near real-time detection with improved sensitivity and selectivity. This is due to the two factors associated with the technology: (1) event-based electrochemical detection process, where the individual step in the formation of the binding complex results in a specific change to the electrochemical conductance due to the pertubation of the electrical double layer at the base of the each well. (2) The nanoporous membrane is an electrical insulator and is structurally robust throughout hence there is improved signal-to-noise ratio and cross-contamination between is minimized.
Another advantage of this technique is the use of electrical signal in protein identification as compared to the use of optical methods; hence, it is a noninvasive and a label-free technique. The signal acquisition is simple and it uses the existing data acquisition and signal analysis methods.
We have demonstrated the use of this technology for addressing a specific clinical problem: identification of vulnerable coronary plaque in the perioperative state.
Every year about 10% of the population of United States undergoes cardiovascular surgery. This costs about $450 billion annually, averaging $13,000 per patient/treatment, which is 40% of the health care budget. One million of these patients have adverse effects after the surgery costing an additional $45 billion. It has been projected that within the next two decades surgical patients would increase by 25%, costs by 50%, and complications by 100% as the population ages.1–4 The current surgical burden is burgeoning as a surgical crisis. Our best allay is to improve the outcomes after surgery to reduce the after effects. Currently, this is being addressed by using medicines, which were developed to address the perioperative ischemia. Perioperative ischemia is the best know predictor for postoperative cardiovascular morbidity and mortality.5–8
At present, the best predictor of how a patient will do after surgery is perioperative ischemia, which is present in 70% of patients with any long-term adverse outcome after noncardiac surgery. 9 Patients sustaining a perioperative myocardial infarction have the worst outcomes. The mortality from perioperative infarction is 25–40%, and higher-risk surgery, such as vascular surgery, has an incidence of perioperative infarction as high as 34%.10–12 Those surviving perioperative infarction have a 28-fold increased risk of cardiac complications within 6 months after surgery. 9 Perioperative ischemia and infarction are thought to occur from plaque rupture of an unstable or vulnerable plaque in most cases.
Even the few patients who may not have had acute plaque rupture, but still had an isolated positive troponin, perhaps from supply: demand mismatch, are at increased risk of mortality after surgery. 13 It is not known what makes a coronary plaque unstable or rupture, but emerging evidence suggests systemic inflammation may contribute to local plaque instability. Inflammation can activate the endothelium, which then expresses multiple cellular adhesion molecules that recruit monocytes and low-density lipoproteins (LDLs) into the coronary artery, which become activated and release cytokines and proteolytic enzymes. These cytokines can induce apoptosis in smooth muscle cells, which make collagen, the structural support for the plaque. The overall effect of inflammation on this balance is to favor plaque degradation and rupture. 14 Furthermore, the unstable plaque temperature is 1 °C higher in myocardial infarction, and is directly related to macrophage density and correlates with systemic levels of cellular adhesion molecules, cytokines, and C-reactive protein (CRP).15–17 CRP has received much recent attention as a marker of inflammation. A meta-analysis of the inflammatory marker CRP demonstrated that the relative risk of coronary heart disease in persons with elevated CRP was 1.7. 18 CRP was also identified as having a strong linear relation to myocardial infarction, ischemic stroke, coronary revascularization, or death in a large retrospective cohort study. 19
Current Limitations+Gap in Technology
Due to the complex nature of the problem at hand, one single biomarker is not sufficient to predict the risk factor of a patient (Fig. 1). The heterogeneity of the condition stems from the fact that many markers have to be considered as potential factors for this condition. Monitoring multiple biomarkers at the same time would provide a holistic image of the patient's condition. To perform such a test there are currently no tests that could do these proteins at the same time, which would require a patient to make multiple visits and also trained technicians to run the tests. We wanted to address these problems by creating a multiplexed test that is easy to perform in a clinical environment (doctor's office), which would require very low quantities of patient's samples. The various proteins identified as potential markers are as follows:
CRP Myeloperoxidase (MPO) Ox-LDL Tissue factor CD40 ligand.
Gap in the current technology and positioning our technology.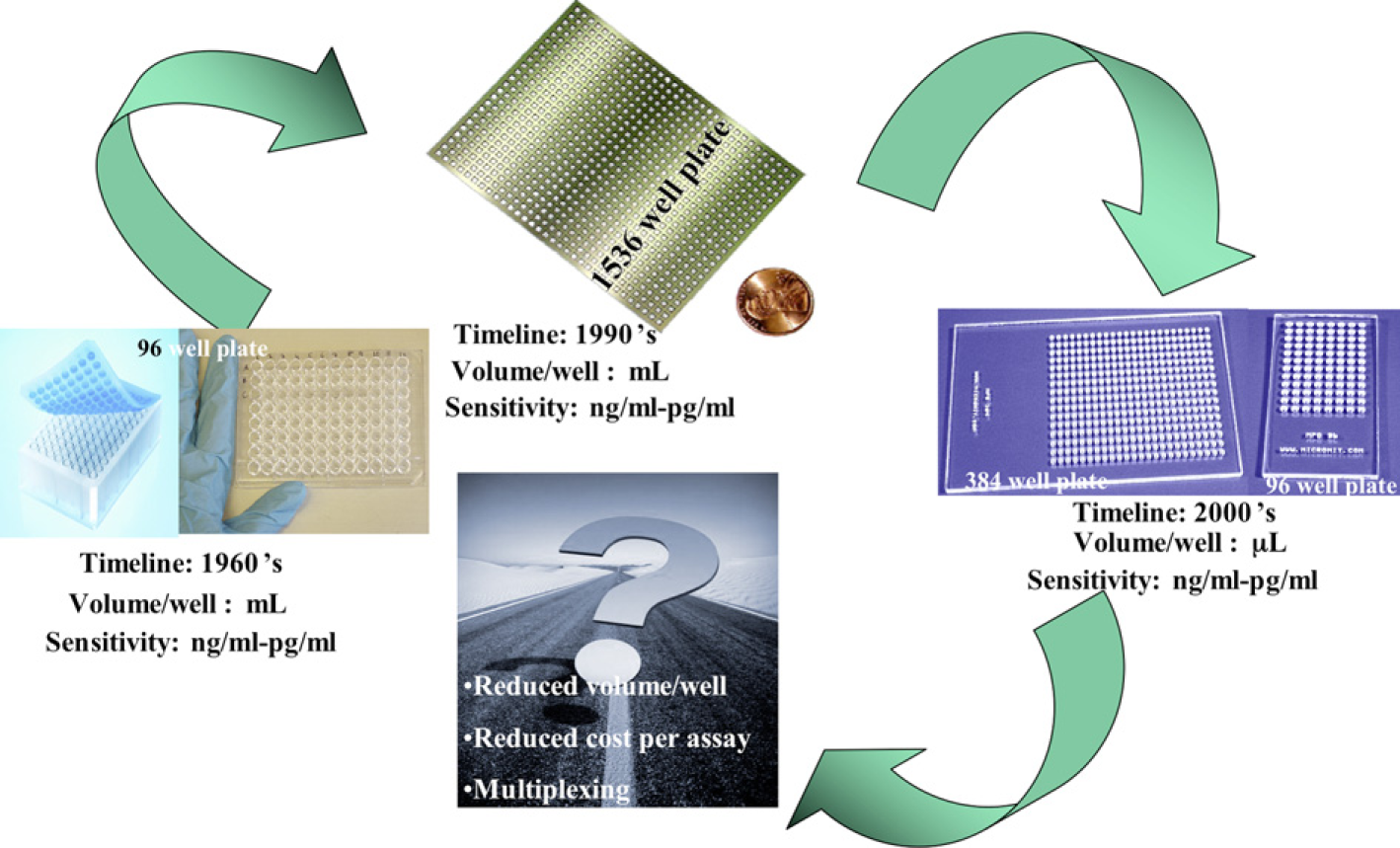
In this current work, we use the first two proteins CRP and MPO as a proof of concept demonstration of the technology.
The goal of this assay was to achieve label-free detection with same specificity and selectivity as the current enzyme linked immunosorbent assays (ELISA) techniques and achieve reduction in cost per assay/test, decrease the volume or sample, and achieve multiplexed detection of the biomarkers.
Technology
We have developed an electrical immunoassay technology that works on the principle of creation of the electrical double layer at the liquid/metal interface and modulation of the double layer due to the addition of charged species such as proteins. We decided to shrink from microtitter well-plate technology to a nanowell plate, which has picoliter volume, and integrate that with the detection and measurement system to improve sensitivity. Integration of both detection and the measurement makes the device label free and easier to use.
Selective capture of the biomarkers need collection and immobilization. To achieve this, we integrated a “nano” fabricated nanoporous alumina membrane onto a microfabricated electrical platform. The membranes of alumina were chosen because the chemistry to make them is well known and the pore diameter could be well controlled.
Alumina membranes are helpful:
Adsorption of protein onto their surfaces due to simple van der Waals bonds. When sample liquid flows on top of the membrane due to capillary effect the molecules in the solution flow to the transducer element (microfabricated platform) at the bottom of the well. Due to the flow of charge on the electrodes, which creates the accumulation of the ions in solution to adsorb on the surface creating the double layer. The electrical double layer consists of the array of charged species and/or oriented dipoles existing at the electrode interface (Fig. 3).
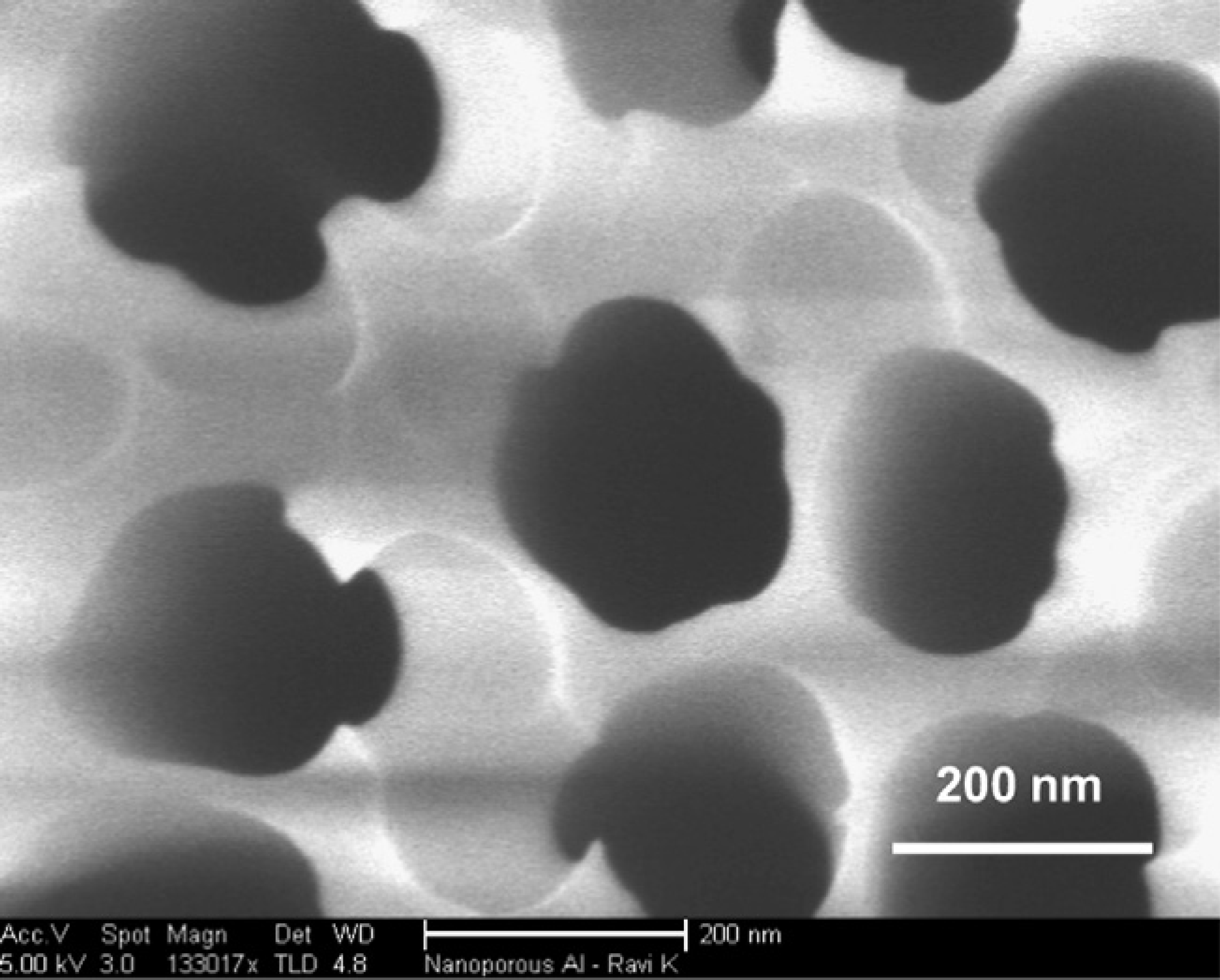
Electric double-layer electrode on which the nanoporous structure exists, the electrons in the electrode cause the free ions in solution to adsorb at the metal-liquid interface creating the double layer, some of the solvated ions also occupy these spaces, the proteins which are charged also reach close to these surfaces which modifies the double layer causing changes to the frequency at which the peaks in energy occur. Scanning electron micrograph showing the nanoporous structure. The structure is very periodic in nature. This improves the accumulation of the proteins on the surface of the electrodes.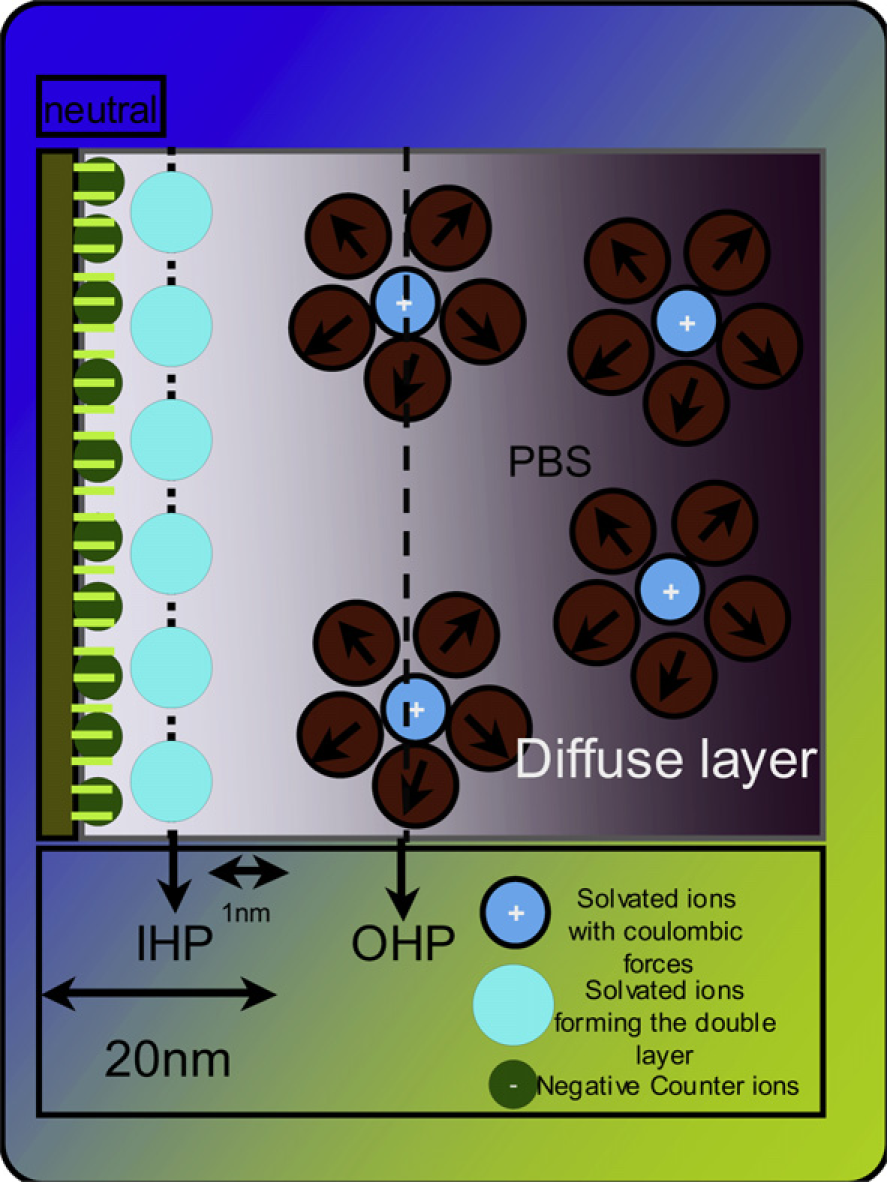
Micro encapsulation of the biomarkers in each well facilitates ease of the transfer of electrons and ions exclusive to that well, providing very little cross talk electrically across wells.
Entrapment of the biomarker very close to the transducer element (microfabricated platform of gold) improves the signal transduction and improves sensitivity of the device (Fig. 4).
(A) Schematic representation of the microelectrode. The pattern is an interdigitated pattern with spacing of 10 μm, with each arm of the electrode being 10 mm. (B) Schematic representation with the nanoporous membrane, showing the creation of wells, which are 200 nm in diameter and 250 nm in height, this would give a volume of about 3 – 10–20 L, which with the massive parallelism on the surface would give rise to a million wells on each electrode, whose entire volume is still less than 1 pL. (C) Optical image of the interdigitated electrodes.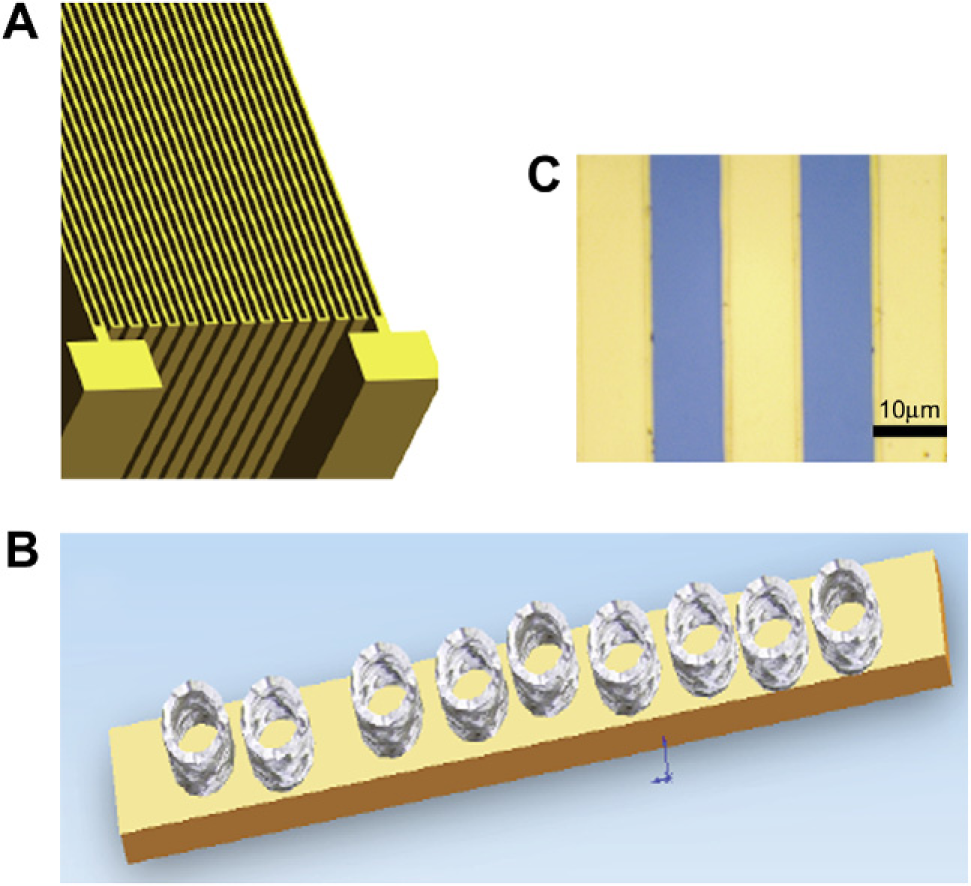
Principle of Operation
The device works on the principle of electrical double-layer formation. Electrical double layer is made of an array of charged particles and oriented dipoles, at the liquid/metal interface (Fig. 2). When an electrode is charged, it attracts oppositely charged species and forms a neutral region around the electrode. This neutral layer creates, other solvent ions in solution. The inner layer, which is closest to the electrode is called inner Helmholtz plane, contains solvent molecules and specifically adsorbed ions. The next layer is called outer Helmholtz plane, the layer after this is called the diffuse layer. We use a basic ionic solution that is 140 mM, pH 7.2e7.4 phosphate buffered saline (PBS) (Sigma Aldrich, MO), to demonstrate the working of the device. The ions in the solution are created at the interface by applying an interfacial voltage. After the initial baseline values are measured, the biomarkers are introduced into the solution, as the biomarkers (antibodies) move to the bottom of the well, there is a perturbation to this double layer, which modifies the charge balance at the interface and this is monitored, to identify the biomarker, which is the sample. This charge imbalance was measured as a current, variation given by the equation:
The frequency of such a signal would give the specificity of the measured biomarker. Voltage variations are also observed to correlate with the exact biomarker.
Materials and Methods
The two-step anodization process was used to fabricate the ordered alumina nanoporous membranes. Purified aluminum is used as the positive electrode or anode in an acid electrolytic bath comprising of 0.1 M Oxalic acid. 20 Varying the temperature of the bath, applied DC voltage and the time of anodization could control the dimensions of the nanopores. The pores we fabricated are of 200 nm in diameter; the thickness of the membrane is 250 nm.
The microfabricated platform made using standard photolithographic process consists of interdigitated electrodes. The size of each of the fingers in the design is 10 μm in width and 100 μm in length.
Experiment Setup and Results
The first step in detection of the proteins was to saturate the nanoporous membrane with the antibody and then inoculate the region with sample for detection. The purified samples were obtained from EMD Biosciences, San Diego, CA. The baseline measurements were recorded with 0.1X PBS because the dilutions for both antibody and the samples were made in 0.1X PBS. The interfacial voltage and the frequency of the voltage signals are recorded. Experimental protocol included the cleaning of the chip before the experiment and then embedding the nanoporous membrane on the chip. Baseline measurements with 0.1X PBS were done, and then the antibodies were inoculated on the surface and the chip was incubated for a period of 15 min at room temperature, the measurements were made after the incubation period. After the measurements are done the proteins were inoculated and the chip was incubated for a period of 15 min at room temperature. The voltages were measured with the oscilloscope (Tek TDS3034). The results for both CRP and MPO are presented here (Fig. 5). After the data are collected, it was further analyzed using MATLAB (Mathworks, MA), a fast Fourier transform was carried out on the obtained data to understand where the maximum amplitudes in the frequency existed. The multiplexed data with both the antibodies of CRP and MPO immobilized on the surface are tested with a solution of both the proteins (Fig. 6).
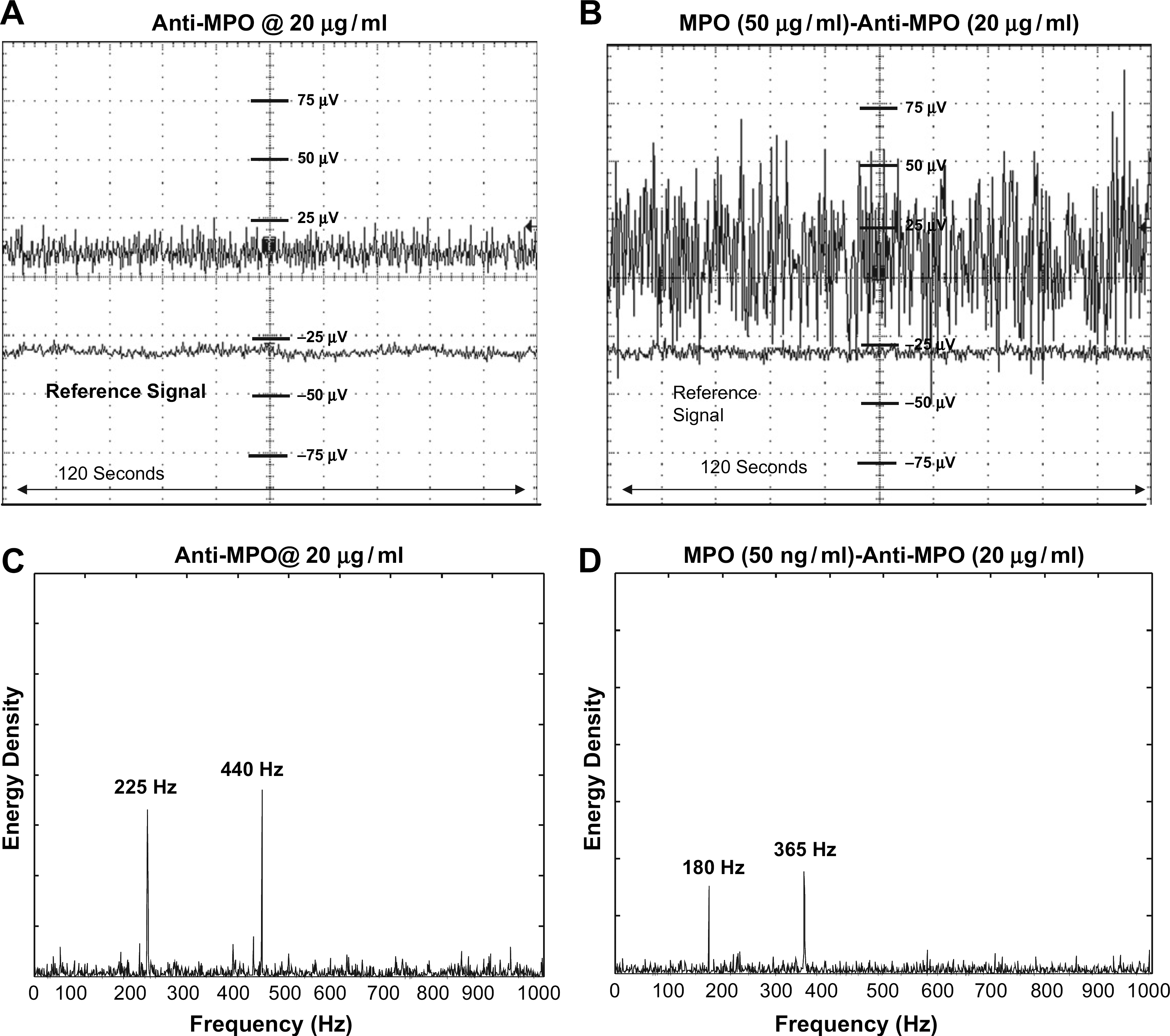
C-reactive protein (CRP) response: (A) Timescale analysis of the voltage measured with immobilization of the CRP antibody on the electrode surface. (B) Timescale analysis of the voltage measured after the formation of the immuno-complex (antibody + antigen). (C) The frequency spectrum analysis showing the frequency peaks generated by the associated mass charge of the antibody, which modulated the double layer which in turn changes the charge cloud at the interface resulting in the observed frequency peaks. (D) Shows the shift in the frequency after the formation of the immuno-complex suggest the change in the structure and therefore shifting of the charges that are at different locations, changing the peaks of the frequency at which they occur. Myeloperoxidase (MPO) response: (A) Timescale analysis of the voltage measured with immobilization of the MPO antibody on the electrode surface. (B) Timescale analysis of the voltage measured after the formation of the immuno-complex (antibody + antigen). (C) The frequency spectrum analysis showing the frequency peaks generated by the associated mass charge of the antibody, which modulated the double layer which in turn changes the charge cloud at the interface resulting in the observed frequency peaks. (D) Shows the shift in the frequency after the formation of the immuno-complex suggest the change in the structure and therefore shifting of the charges that are at different locations, changing the peaks of the frequency at which they occur.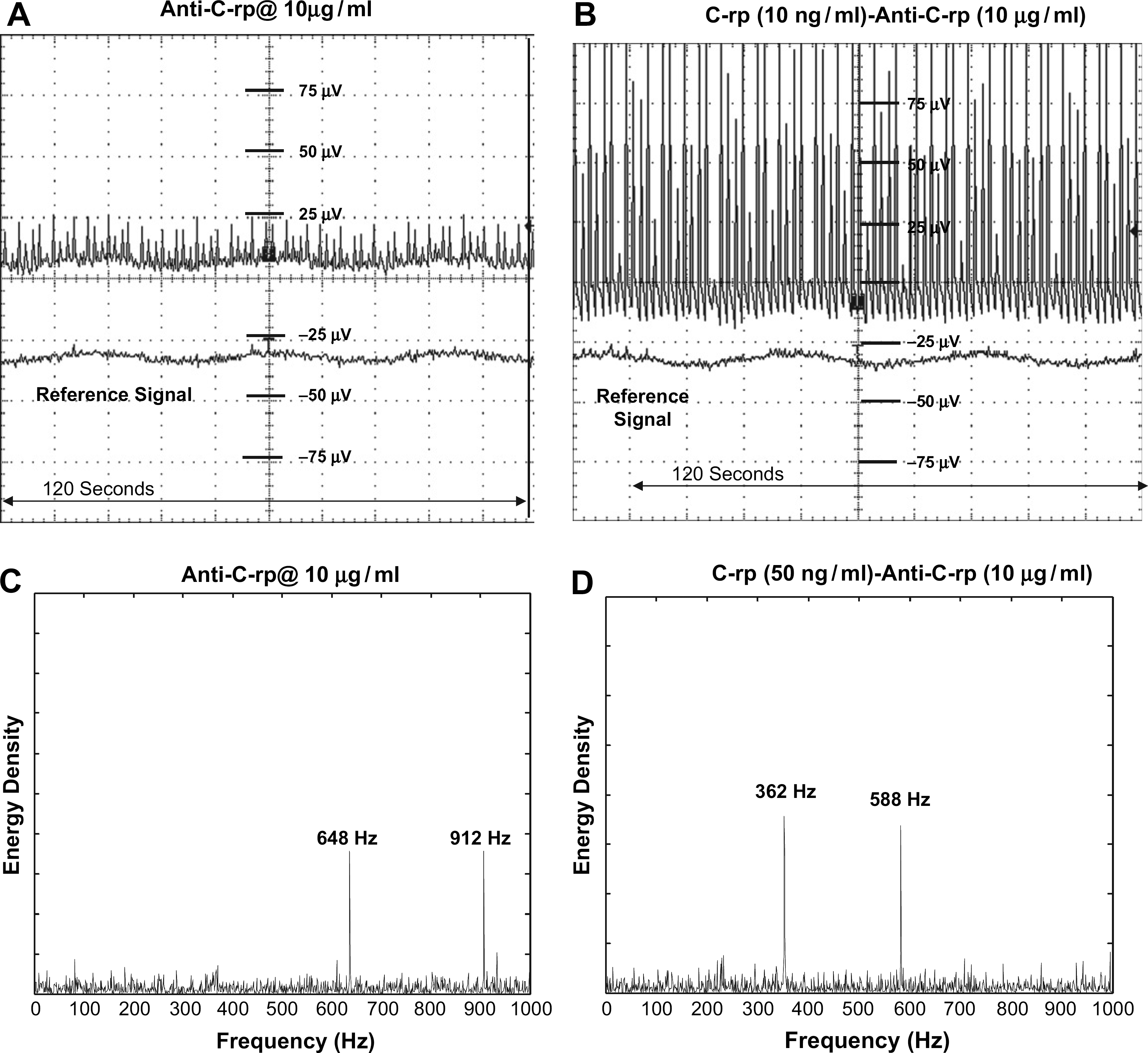
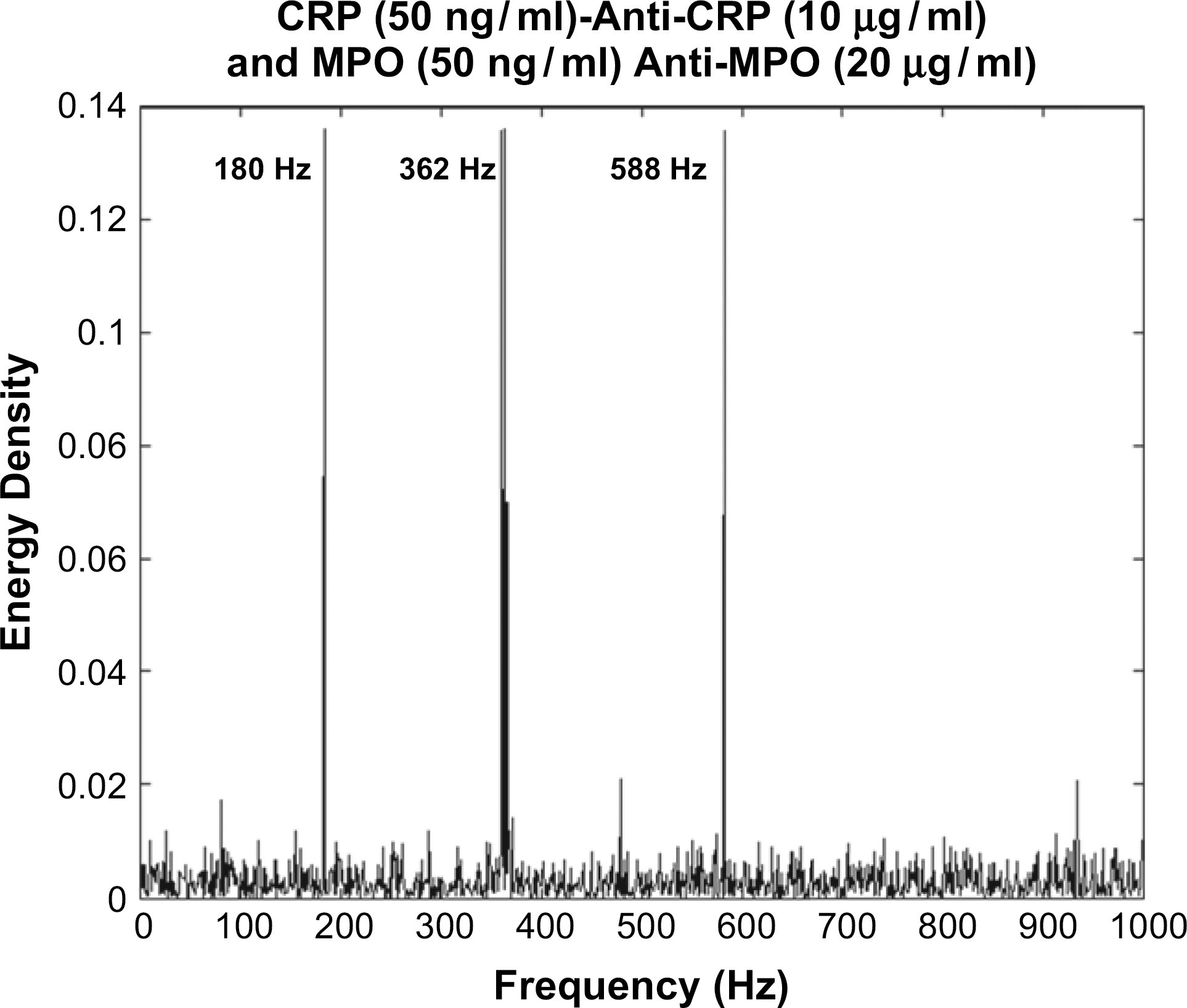
Further experiments conducted with the serum (Fischer Scientific) to check for the nonspecific binding issues associated with most immunoassay setups. The results from these experiments are presented here (Figs. 7 and 8).
Frequency response analysis with the protein in serum. Human serum was spiked with 10% C-reactive protein and tested with the immobilized antibody. The specificity associated with the frequency is still present indicating the detection mechanism is consistent even with nonspecific interactions. The noise floor is higher than with just pure samples, indicating the presence of nonspecific binding interactions. Multiplexed response: Response of both the antibodies and the proteins analyzed. The frequency response with the immobilized antibodies and the formation of the immuno-complex indicates the specificity of the response even in the presence of other competing proteins. The measurement technique is specific to the charge variations at the double layer in each nanowell, the miniature effects combined with the parallel measurement across million such wells give the exclusivity and specificity of the technique.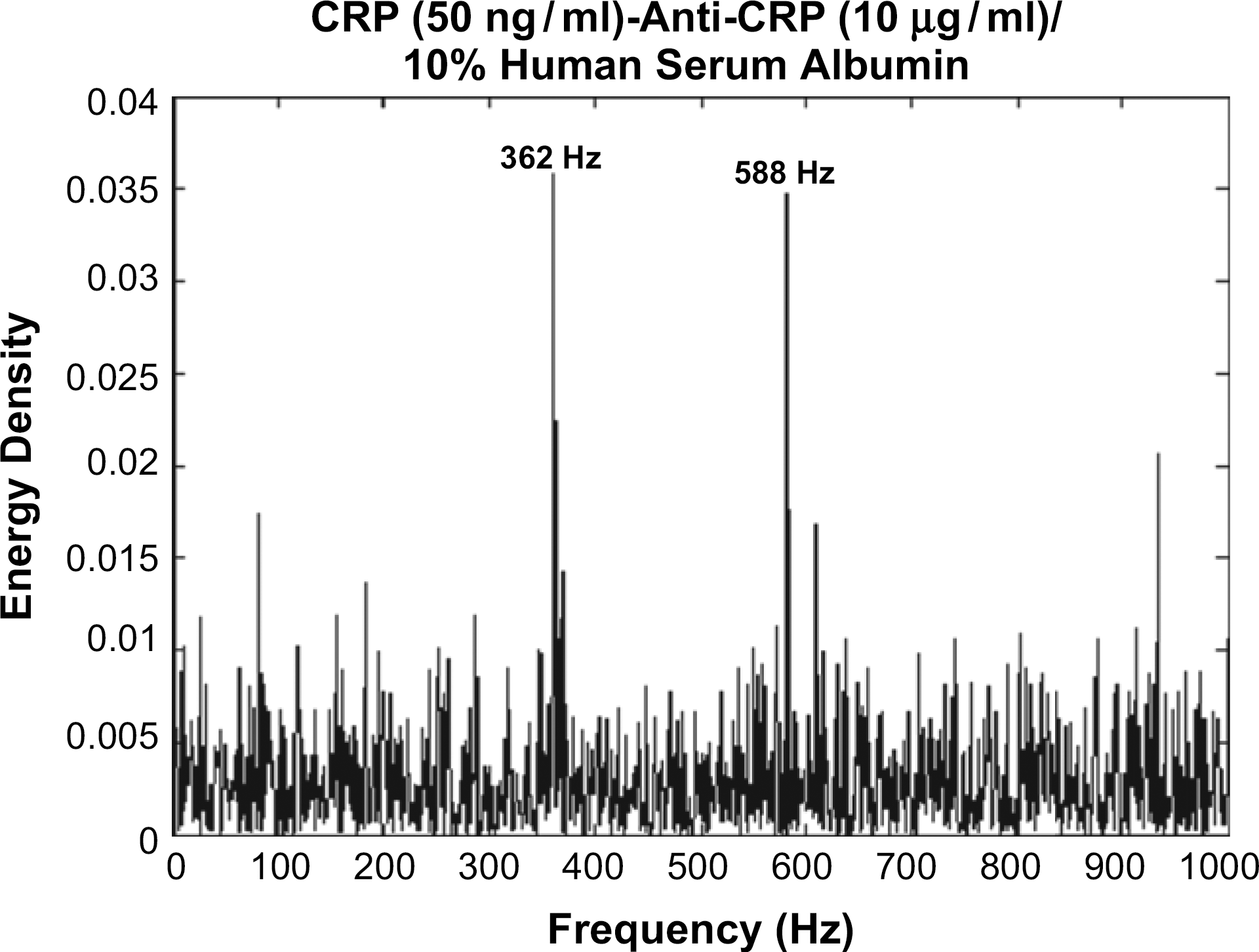
There were eight data points in the dose–response curve from 1 to 500 μg/mL. Each data point was evaluated in triplicate. The same peaks were observed in the frequency domain for the specific protein biomarkers. There was linear correlation between the amplitude of the frequency peaks and the concentration with the amplitude decreasing with decreasing concentration.
The change in the frequency peaks in pure and serum-spiked samples was less than 5 Hz, this was considered negligible and hence the technique is considered to be relatively robust to the frequency shifts on addition of complexity to the test samples.
Discussion
In this article, we have demonstrated the design, fabrication, and operation of electrical biosensor for protein biomarker detection. We have selected two inflammatory proteins, CRP and MPO, as the study proteins to demonstrate the operation of the device prototype. These protein biomarkers were chosen as they are thought to be biomarkers of the vulnerable coronary plaque rupture state.
The basis of the electrical biosensor functioning is the perturbation to the Helmholtz layer due to the binding of the relevant proteins from a test sample. This perturbation results in a modulation to the electro-ionic distribution of the interfacial electrical double layer formed in each of the nanowells/pores).
The time domain variations to these perturbations when translated into the frequency domain result in resonant frequency peaks. We can correlate the frequency peaks to occur due to the protein-binding event as the same peaks were observed both from pure samples and serum-spiked protein samples. The signal-to-noise ratio of the peaks were at least three times larger than the back ground noise in both the types of test samples, indicating that the signal was not an electrical artifact but occurred due to the protein-binding event.
Two peaks were observed in each case and it is hypothesized that there may be two resonant states associated with the docking and binding of the CRP and MPO molecules, further work is underway based on molecular dynamics simulations to investigate the binding mechanism. But it is clear from the current work that it is possible to selectively identify surface-charged proteins by measuring the variations to the Helmholtz layer in nanoscale confined spaces.
PBS was used as the baseline solution based on the protocol obtained from EMD Biosciences that synthesized the antibodies and antigens. The isotonicity and the pH were appropriate for running the test experiments. 1X stands for stock solution, whereas 0.1X indicated a one-tenth dilution of stock PBS solution.
The current work is a feasibility study indicating that changes at the nanoscale can be captured and correlate to protein-binding events thus indicting a promise in the development of a technique that is rapid and label free for the detection of protein molecules (Figs. 5–8).
Conclusion
In the studies conducted, the device has been tested with standard synthesized samples obtained from the vendor. The samples have been validated with ELISA Vendor validation datasheets. We observe peaks in the measured signals, which seem to indicate the presence of the antibodies and the immuno-complex formation when it occurs.
Future work
In this work, we were trying to prove the principle of operation of the device based on our initial assumptions. In the future work, we plan to improve on the limit of detection and analyze more proteins to test the multiplexed detection capability of the device.