
Abstract
The first total clinical laboratory system (TCLA) in the Osaka City University Hospital was introduced in 1993. After six years of operation, it was recently replaced by a new system. The goals of this replacement were as follows: 1. Improve the analytical performance. 2. Make the system operate more efficiently. 3. Improve the quality of laboratory analyses. We successfully reduced the labor required to operate the laboratory; made the laboratory reports quicker; reduced the number of retraction and revalidation of the results; and minimized the system downtime.
INTRODUCTION
At the Osaka City University Hospital, the development of total clinical laboratory automation (TCLA) was originally started in 1967 when the first clinical chemical analyzer in Japan was developed in collaboration with Hitachi Company. In 1993, we developed and introduced a Laboratory Automation System (LAS) 1 . LAS is an assemblage of components of pre-analytical, analytical, and post-analytical functions assisted by a conveyer system that transfers specimens and a Laboratory Information System (LIS) 2 . It has operated successfully and has saved laboratory labor and improved various strategies for laboratory management 3 . After six years' operation, the system was aging. The number of samples received at the central laboratory has increased each year. Over 3,500 patients visit the hospital daily. The system was initially designed for 2,200 outpatients and 1,000 inpatients per day. We decided to replace the system in 1998. The project to design the new system started in February 1999 and installation was completed in March 2000. This article details the progress of replacement as well as our experiences during the first year of operation.
DESIGNING A NEW TCLA SYSTEM
The central clinical laboratory of the Osaka City University Hospital is a centralized facility that provides laboratory tests for all routine, special chemistry, hematology, immunology, urinalysis, microbiology, pathology and DNA/RNA testing. It also serves as a substitute to the STAT laboratory. Upon deciding to replace both the LAS and LIS in 1998, the following goals were discussed:
Efficient specimen transportation on the line. To streamline the transportation of specimens to the analyzer we adopted a “clockwise one way” direction for distribution.
Quicker sorting upon sample receipt. The previous sorter was limited in the capacity of processing specimens − 1,000 per hour at the maximum speed. Our goal was to raise this capacity by improving the specimen identification system that reads the bar code on a tube. Efficient bar coding and an updated reader helped reduce the waiting time while identifying the patient and confirming the requests. The sorter can then send the specimen instantly to one of the three major lines: hematology, coagulation, and chemistry. In addition, we simplified the movement of robotic arms that transfer specimen tubes to the standardized rack.
In the previous TCLA system, two automated centrifuges stood on the way to the chemistry and immunology line that had a maximum capacity of 250 specimens per hour. Insufficient capacity often delayed the process. We aimed to design a quicker robotic arm that picked a rack up, carried it, and placed it in and out of the centrifuge unit. We also planned additional centrifuges on the line.
We tried to improve the capacity of the decapper units (350 stoppers per hour), aliquoter units (300 specimens per hour), and recapper units (400 closures per hour).
Considering the “man-machine interface”, we tried to design a device smarter by ourselves.
To provide more free space in the laboratory, we designed a shorter conveyer line and a simple layout so that every technologist can work comfortably.
The high-grade quality control program was uploaded such that every technologist could plan for preventive maintenance of an analyzer or the conveyer mechanisms. This helped us anticipate the shorter downtime that might affect the smooth sample processing.
Consolidation of the test function among analyzers. Several tests were processed by two analyzers in duplicate for the purpose of quality assurance. We abandoned this duplication with the expectation that it would lead to cost and labor savings.
We constructed an updated client-server system in the HIS-LIS network to improve the entire information system.
We developed intelligent information software to provide useful laboratory announcements and a business memo to the medical staff.
We tried to give flexibility to TCLA for renovations in the future.
MATERIALS AND METHODS
Because of the difficulty of replacing the LIS concurrently with the replacement of the LAS, the computer and its software for LIS were replaced on March 1999, prior to the replacement of LAS and analyzers. This was previously reported 4 and is briefly described here. Two server computers (SUN 7/400: 1024MB memory with two 9.1GB hard disks and connected to five 9.1GB RAID memories) were linked with the HIS main computer (Fujitsu GS8600/300). Two SUN servers are working in tandem adopting the disk-array structure so that it can be accessible 24 hours a day with no downtime. LIS also has 50 client computers (Fujitsu FMV6350CL2), four automated bar code labelers, and ten bar code printers. All laboratory analyzers and data-input-terminals are on-line connected via a LAN network.
LAS has an independent computer called the line controller (Hitachi HILAS), which controls sample transportation by conducting the conveyer lines and sends messages to each analyzer or aliquoter. The line controller works separately but cooperates with LIS. The configuration of the client-server system of LIS allows easy management of the laboratory database and allows for a multi-user environment by applying the in-house local area network via Ethernet.
The manufacture of LAS instruments began in February 1999. The installation and the evaluation of LAS were finished in April 2000. During the replacement period all routine jobs were processed in the same room, as before, while the new TCLA system was simultaneously constructed and installed. The hardest aspect of replacing the TCLA instruments was not being able to stop any routine laboratory work because the laboratory services were critical for the medical services in the hospital. The replacement was carried out mainly on weekends and holidays to minimize the effects on specimen processing. By this “scrap and build” operation, we carried the new devices in and carried old devices away. The replacement was successfully completed, and no routine jobs were interrupted. We introduced and evaluated a couple of analyzers at the same period. Once the results assayed by the newly introduced analyzer agreed with the results assayed by the old analyzer, we switched the analyzers for use in routine analyses.
Training on the new instruments and devices occurred outside of normal working hours. Regarding the clinical laboratory jobs, there were several “sections” with respect to the laboratory procedures that consisted of operators and analyzers related to the tests. For example, there was a chemistry section and a hematology section. During training we focused on making the TCLA operate smoothly; the conventional “sections” were then phased out. The new sections were temporarily constructed and operated transitionally during TCLA replacement. (“Section” was renamed “block” in TCLA, see figure 1.) Four months were spent for the complete replacement and the evaluation of TCLA.
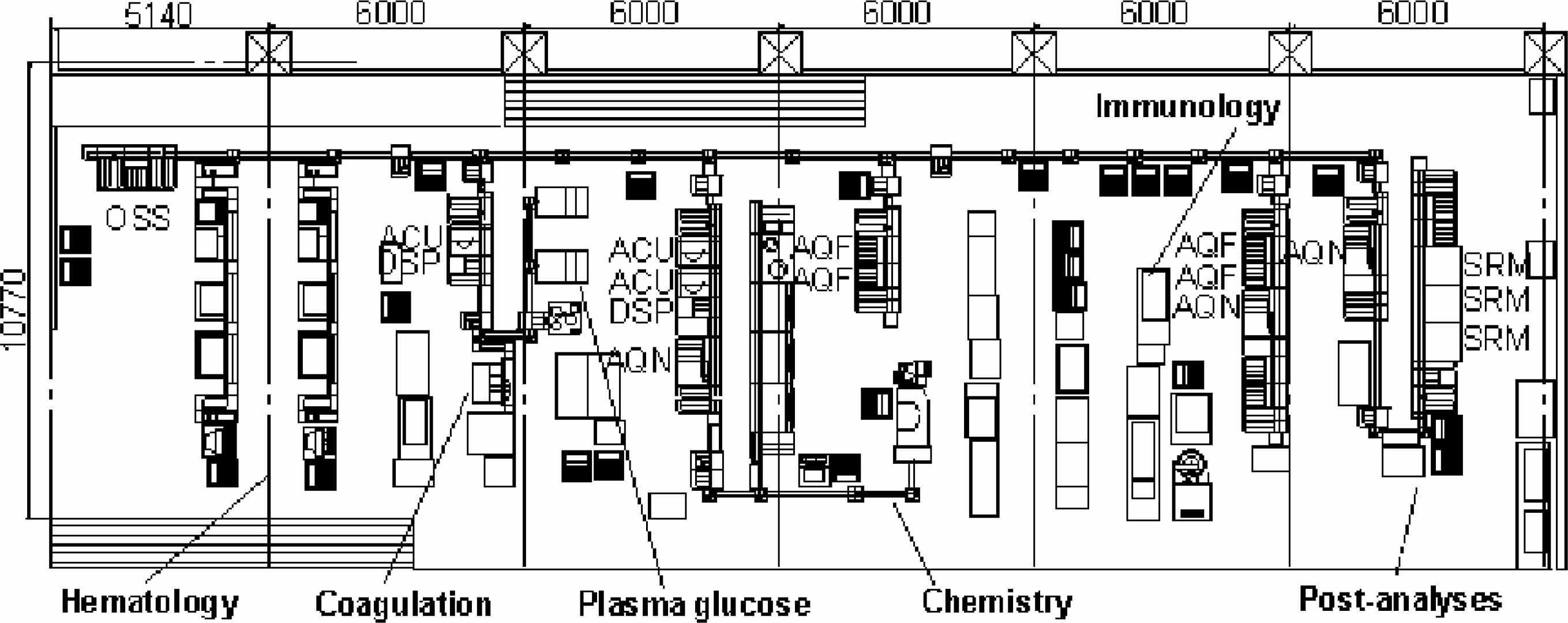
The layout.
THE NEW AUTOMATION SYSTEM CONFIGURATION
The system consists of one sample sorter, three major lines and four units:
Sample sorter Hematology line Plasma glucose plus coagulation line Chemistry line Aliquoter for daughter tubes (for more complex tests) Aliquoter for sending samples to the reference laboratories Aliquoter for offline connected immunochemistry analyzers Sample retrieval line with automated insulated storage
(See figure 1 for the layout of the TCLA.) A sample tube, sent either from a ward or the blood collection center for outpatients, is received at the original sample sorter (OSS) of TCLA. Each sample tube is placed in the standardized rack that has five halls for tubes. OSS reads the rack bar code on an end wall of each rack (rack ID), and reads the sample bar code on each tube (sample ID) individually. Patient information is given to OSS via the LIS, and the OSS sorts samples according to the tests requested. Sorted tubes in a rack are sent to one of three major lines: hematology, plasma glucose plus coagulation, or chemistry. Samples on the hematology line are processed to the blood cell counter and analyzer (Sysmex XE-2000, Sysmex, Kobe, Japan), reticulocyte counter (Sysmex R-3000) and blood film preparation unit (Sysmex SP-100) 5 . LAS delivers the samples to the Sysmex conveyer line, which is connected to but is independent from the main conveyer line. The Sysmex line uses a unique rack that has ten positions each. OSS sets hematological samples from the standardized five-position rack to the ten-position rack before delivery. The hematology line branches into two parallel lines. Each line consists of three instruments in series and each instrument takes a sample at a designated point on the interconnected track. Each hematology instrument communicates directly with LIS for order queries and uploads the results.
The samples on the plasma glucose plus coagulation line are centrifuged on the automatic centrifuge unit (ACU). Subsequent to centrifugation, the destopper module (DSP) removes a tube closure automatically, then the line branches away into the next two lines. At the junction next to ACU, the conveyer approaches the coagulation analyzer (Sysmex CA-6000) and leaves the line to go towards the analyzers for plasma glucose (Hitachi 7020, Tokyo, Japan), hemoglobin A1c and glycosylated plasma protein (Arkrey HA-8150, Kyoto, Japan). Those instruments are connected on-line.
The samples on the chemistry line are also centrifuged by ACU and subsequently decapped. The sample check module (SCM) located just after ACU detects any possible interfering substances including clots, turbidity, icteroid, and hemolage, and ensures the necessary minimum volume is present. If SCM detects an inappropriate sample, the sample is kicked out from the line to the table of “defects” and the SCM gives an alarm sign. The defective specimen awaits the operator's prompt decision.
The chemistry line has a fundamental chemistry analyzer (Hitachi 7600-310) with two types of modules: D and P. 6 D-module is a multi channel parallel-automated analyzer and has a large capacity for processing tests. The P-module is a random access automated analyzer and processes specimens one by one. P-module is suitable for analysis when the number of requests is small. The analyzer in our laboratory has three D-modules and one P-module, and has the capacity to process eight thousand (8,000) samples per hour. Downstream of the chemistry line, several offline aliquoters (AQF) and online aliquoters (AQN) are connected. AQF and AQN provide a “daughter” tube that contains a portion of a specimen placed in a new tube with a new label for identification. The daughter tubes can be used by the offline analyzers, and/or for further special analysis at reference laboratories. The daughter tubes are also reserved for future research use.
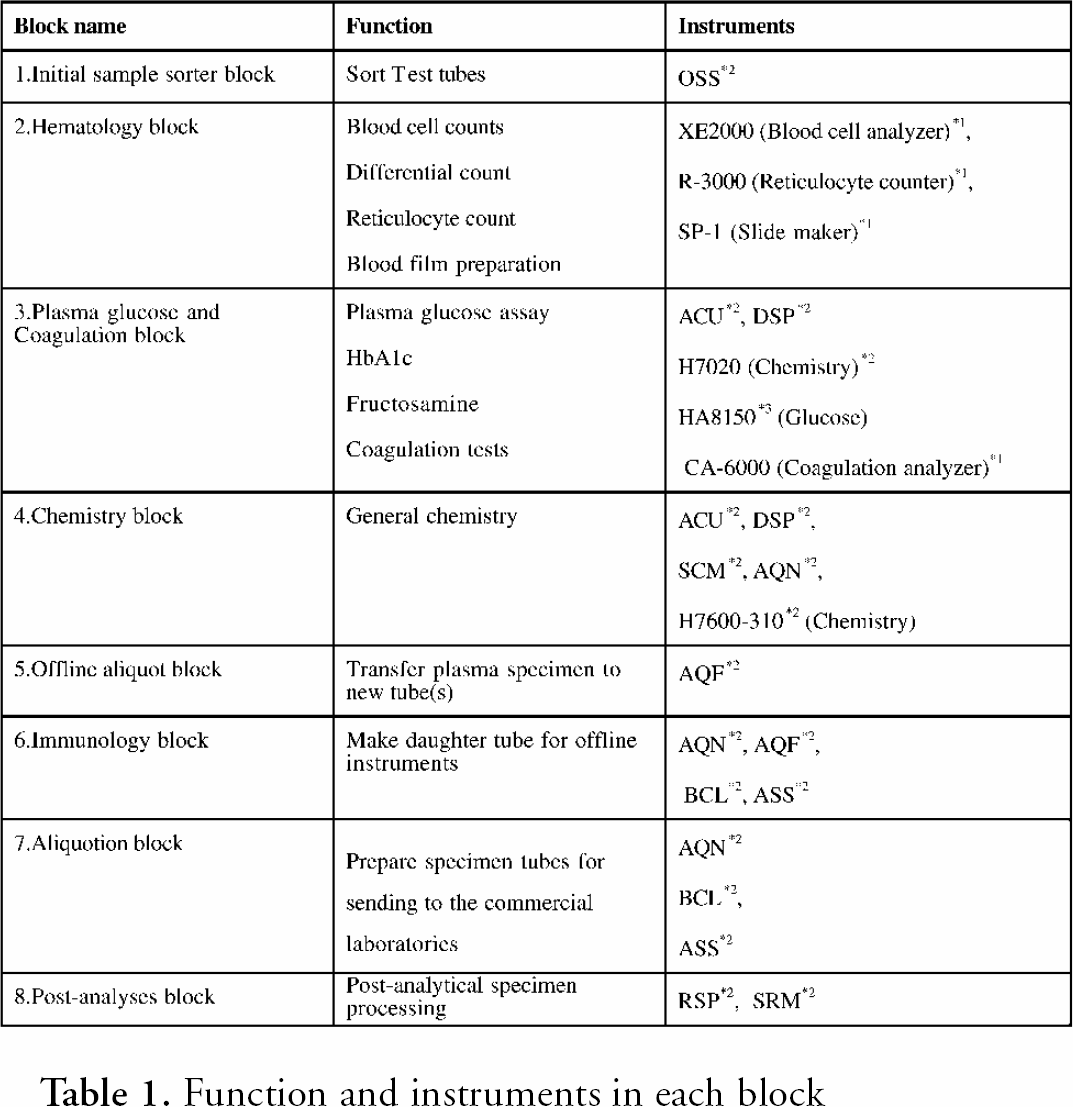
Three sample retrieval modules (SRM) are on the end of the conveyer line. SRM processes the parent tubes that contain the surplus specimen after analysis, puts a stopper on the tube and places it into a refrigerated stockyard for sample storage. If a test must be resumed for quality assurance, or if an additional test is requested, the requested tube is picked up from the refrigerator of SRM by using the sample ID. Autonomous Decentralized System (ADS) is installed on TCLA system software so TCLA can keep working if a module malfunctions or runs on an alternate state. As each module controller runs independently, each one is free from the other. If one ACU is down in the chemistry line, the second ACU works instead so that TCLA does not delay the process. More details about each block and unit of TCLA devices and instruments are given in table 1 and table 2.
Function and instruments in each block
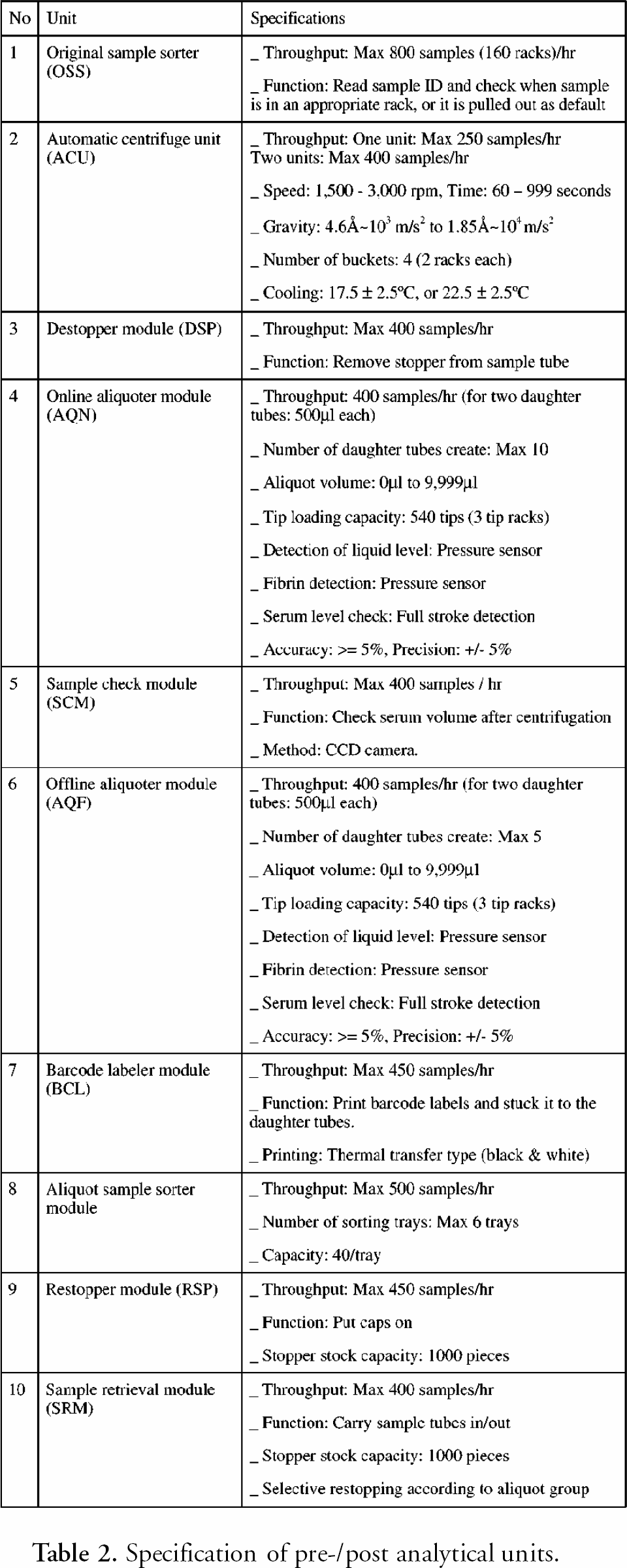
Specification of pre-/post analytical units.
LIS AND SOFTWARE CONFIGURATION
The new LIS that cooperates with LAS was selected from a multitask client-server computer architecture, and Multi-Terminal Server (MTS) of LIS was developed from our need to reduce system down-time. MTS was connected with an analyzer by RS-232C. The communication could be established without rewiring unless the IP address was changed. Redundant Arrays of Inexpensive Disks (RAID) 7 8 was also expected to help reduce the risks of the server being down. We developed the system of RAID five level. A double cooling fan for the computer hardware was installed. If one fan malfunctions, the other will run automatically to avoid the heat excursion of the system. To make LIS operation more user-friendly, we adopted the Comma Separated Value (CSV) files (*.csv) for writing a patient file. Personnel can easily apply the CSV file onto the commercially available software.
For quality assurance purposes, we added several programs including the Levey-Jennings control chart and the delta check method. The delta check method finds sudden changes (shifts) in successive data from a patient, which can be physiologically exceptional. Upon receiving the test results, LIS drops each result in one of three criteria (see below) and sends a command for the necessary action to both the LAS and the analyzer by the automatic data validation process.
Rank 1. Within a normal range. No command
Rank 2. Beyond the technical error. Show a flag on the monitor and send a command to the responsible analyzer to retrieve and retest the specimen without any manual operation.
Rank 3. Beyond the panic range (pathological). Send a conditional command depending on the method to the responsible analyzer and give a notice to the operator.
RESULTS
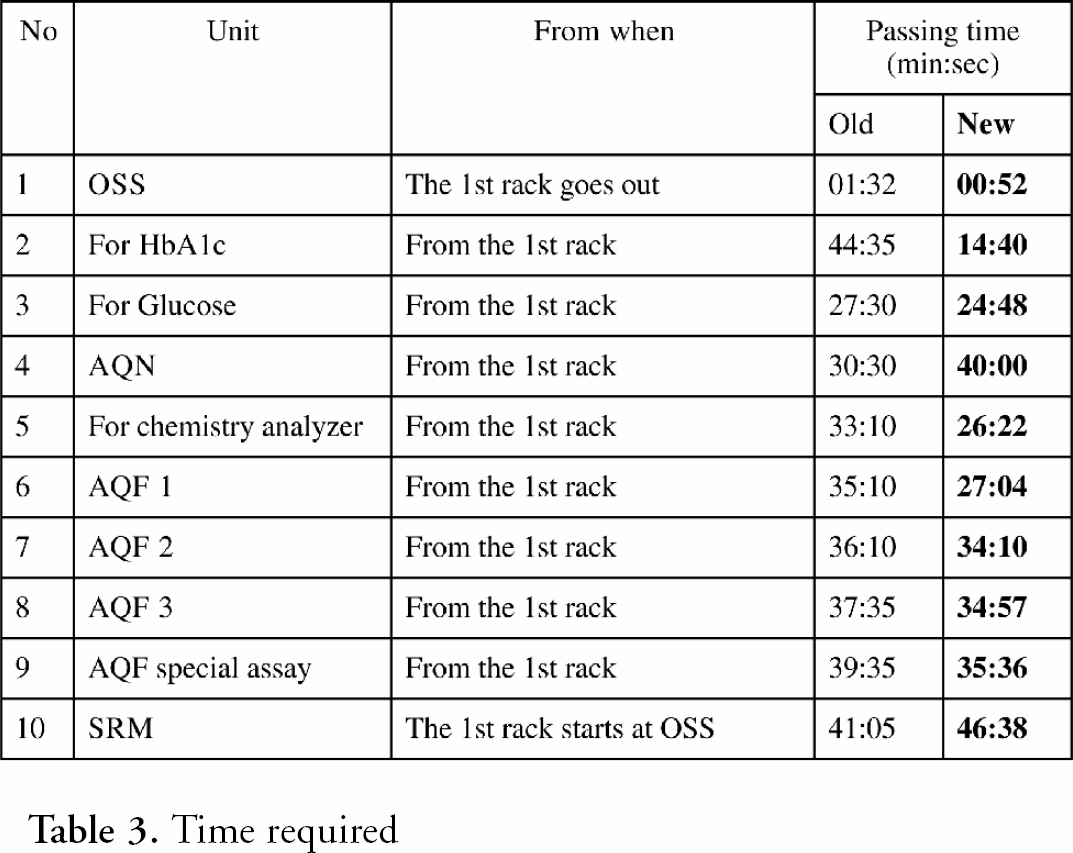
After completing installation and validation of the new TCLA, we started routine laboratory services in April 2000, and saw the following improvements. (See table 3 for a comparison of instrument performances.)
Time required
Reduce the labor requirement for TCLA. Three technologists from the conventional staffs could move to echography, pulmonary function, and STAT service sections. Six technologists are currently allocated to operate TCLA. Manage the effectual free space in the work area. The new LAS occupies 140 square meters; 80% of the area of the previous one (174 square meters). It conveniently shortened the operator's walking path Quicker process and quicker report. TCLA processes about 80% of the samples received at the laboratory. OSS accepts those samples and sends them to the line more efficiently than in the former system. Two faster ACU have been consolidated and another one is supplemented to the coagulation line. The “core” analyzers for chemistry and hematology have bigger sample processing capacities. The LIS system uses 100Mbps Ethernet for data transfer and allows communication by 10Mbps. The automated analyzer for hematology is able to process one “blood cell counts” every 40 seconds. Additionally, processing “reticulocyte count plus white cell differential count” takes another 20 seconds (60 seconds total) by the analyzer. These processes took 45 seconds and 85 seconds by the predecessor, respectively. The average turn-around-time for the general panel is approximately 24 to 37min (38 to 55min in the past). The effect on the total clinical services shortened the patient's stay at the outpatient clinics more than half an hour (from two hours and 45min to two hours and 10min in average). Reduce system down time. ADS installed on TCLA system reduced the delay of the automation process. MTS and RAID for the client-server systems also helped to minimized down time. As a result of our efforts, the occurrence rate of the total system down time during our evaluation period is 26/1000/unit/month compared to 64/1000/unit/month in the past. Quality assurance software Due to the automatic data validation process by LIS, the new system reduces the labor requirement for quality assurance. Only 7% of the total tests need to be reexamined compared to 10% in the past. Laboratory Information service. Medical staff can change the data style for a patient by using a data terminal attached to HIS with a file written by the CSV files originally from LIS. This could reduce phone calls to make special inquiries about test results. Information about the general laboratory can now be disseminated to the medical staff via an HIS data terminal.
DISCUSSION
Not only in Japan but also in many countries, more efficient management is required for health care services under the current economic environment. Operating the laboratory system in a hospital has been strongly suppressed during the past two decades. Today, evidence-based clinical medicine is more important and thus a smart diagnosis is required now more than ever. Practicing tactical laboratory examinations in an intelligent way can also decrease total costs. When considering cost management of a clinical laboratory, labor costs should be considered as a major factor among the total costs per test. The standardized simple jobs including sample transfer and setting from the reception table to the automated analyzer are easily replaceable by using robotic arms and conveyers.
In the central clinical laboratory of the Osaka City University Hospital, TCLA system started to run in 1993. In 1998, a project for the system replacement both for TCLA and LIS was started. In March 2000, the system had been completely replaced and from April 2000 routine operation started.
The most difficult question during the system replacement was how to operate a nonstop laboratory service. We could not stop any analyzers from Monday to Friday or allow any interruption in the distribution of results. We could not use any replaced instruments before complete validation. We had to compare the results from the same samples assayed by both old and new instruments at a validation step. An eight-week period was needed for us to evaluate the core chemistry analyzer, Hitachi 7600-310. Both the old and new systems were operated in parallel during the period. Stand-alone units of the automation system were settled and then replaced gradually. A glucose analyzer, a hematology analyzer, and a coagulation analyzer were replaced one by one so that every laboratory technologist used them after training.
Prior to this replacement, LIS was completely upgraded. We selected a client-server system because of its dependability on secured information services. All information is kept in the server. If one client goes down, the task assigned to the client can be switched to another only by the parameter change. A physical wiring for the communication between LIS and an analyzer is normally connected by RS-232C. MTS solves the problem of rewiring of these connections, by converting between one Ethernet port and up to eight RS-232C ports. Ethernet connects the client and MTS, and the MTS and the analyzer are connected by RS-232C. The IP address is the key to establishing communication between them. RAID level five was developed to reduce the risk of the server being down. The duplicated server also resumes the system within fifteen minutes even if the server fails. When recording data from an analyzer, it is divided and stored in several hard disks. If a hard disk fails, lost data can be recovered from the remaining hard disks. These features guarantee minimal failure of the system.
The new TCLA system had a tremendous impact on cost savings for laboratory management, and has shortened the time for the qualified report. Three labor requirements allocated to operate the former system have been reduced, and this savings allowed us to expand the laboratory service. The development and the adoption of the flexible autonomous technology, the upgraded quality assurance software, and the advanced disk array technology with the client-server computer architecture made this possible. Current network technology also allows quick access by Ethernet. This technology also makes it possible to monitor and control the system any time from anywhere on the network. To meet our final goal, the system was designed so that all of the instruments and systems are changeable if we encounter any difficulties. A twenty percent downsizing of the system (174 to 140 square meters) should make future renovations more convenient.