
Abstract
Akita University Hospital was established in 1971. Since then, we have been introducing automated analysis systems to deal with rapidly increasing tasks and demand in the clinical laboratory. In 1988, in collaboration with Hitachi Ltd. (Tokyo, Japan), we developed an automated analysis system composed of an automatic serum separating-aliquoting system connected to analysis systems through an automatic transport system. In 1998, the systems were integrated, enabling 97.6% of samples to be analyzed automatically. With this integrated system, information including the name of the patient, code number, age, gender, department, test to be performed and so on are all encoded on the label of the sampling tubes which are automatically labeled and sorted at the sampling division. The laboratory automation system succeeded in saving labor and time, yet there are still some areas that need improving. Namely, 1) minimizing the quantity of the sample required for analysis, 2) speeding up of the transportation, and 3) down-sizing the system. The development of less invasive, more compact and speedier analysis systems will make the clinical laboratory mobile or portable in the near future and will expand the working field of the clinical laboratory to remote areas and home-nursing services in the community.
INTRODUCTION
Clinical laboratory medicine has progressed in the last several decades following the evolutionary change in medical science. It was only 40 years ago that clinicians made their diagnoses mainly with their eyes, ears, hands and some simple laboratory examinations, which were done almost totally manually. Today, we have many diagnostic tools to help us reach an accurate clinical diagnosis. Progress in clinical medicine brought with it a rapidly growing number and variety of clinical examinations, necessitating the introduction of automated analysis systems in clinical laboratories.
Since the establishment of Akita University Hospital in 1971, we have been introducing automated analysis systems to deal with the rapidly increasing tasks and demand in the clinical laboratory. In this paper, we describe the past and present automated clinical laboratory at Akita University Hospital and briefly discuss the future of laboratory automation.
THE BACKGROUND OF LABORATORY AUTOMATION IN JAPAN
The elderly population is rapidly increasing in Japan, resulting in a great increase in medical expenditures and a deficit for the balance of the national health insurance system (Figure 1). A policy to reduce medical expenditures is attracting special interest in Japan. The cost of laboratory examinations, which make up about 10% of total Japanese medical expenditures, is also affected by the policy. The annual number of samples handled by one laboratory technician showed a more than four-fold increase from 15,000 in 1975 to 70,000 in 1997. A shortage of manpower in our laboratories, together with the ever-growing national medical expenditures in Japan, forced us to develop a cost- and time-saving automatic analysis system for our clinical laboratories.
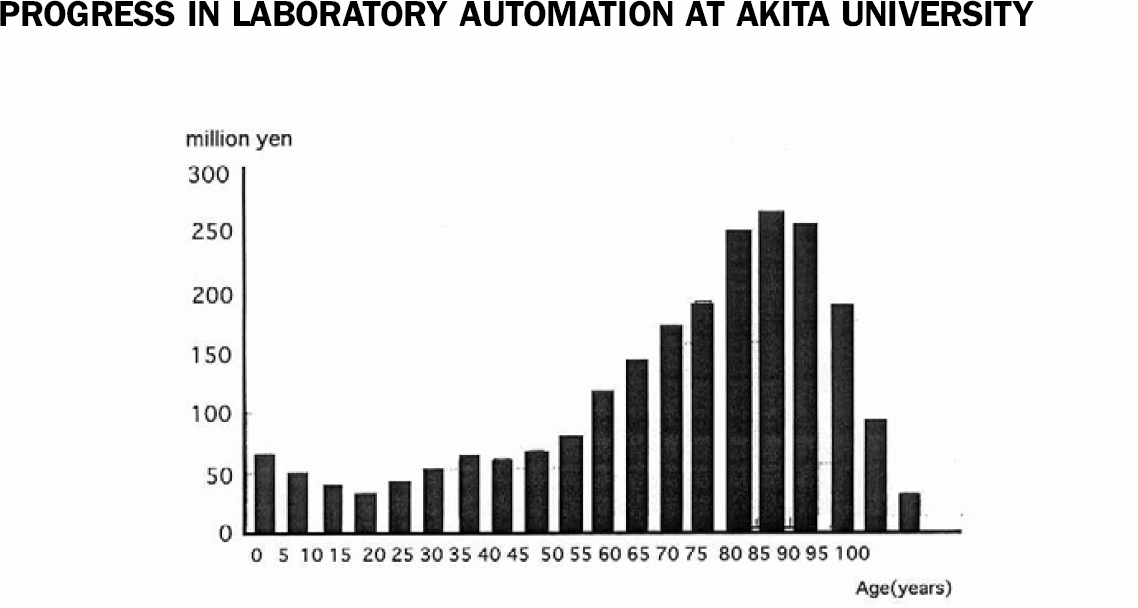
Age and medical expenditures in Japan. In Japan, the elderly population is rapidly increasing. The elderly tend to suffer from more chronic diseases. The increasing number of elderly people means an increase in the demand for medication.
PROGRESS IN LABORATORY AUTOMATION AT AKITA UNIVERSITY
HOSPITAL
In Japan, the first automated sample transportation system was developed at Kochi Medical School in 1982. In the clinical laboratory of Akita University Hospital, an automated transportation-analysis system was developed in 1988 in collaboration with Hitachi Ltd., (Tokyo, Japan). The outstanding feature of the system developed in Akita was that the system was equipped with automatic serum separating and aliquoting apparatuses enabling fully automatic sample preparation. In 1992, by adding a re-entering transportation circuit and a self-assessment program, automatic re-analysis or additional examinations became possible for samples with abnormal or questionable results. This was called a Logic-Assisted Laboratory Practice (LALP) system. In the 1990s, these systems were added to the divisions of hematology, immunology, urinalysis and sampling, and connected to the fully computerized ordering system of the hospital, enabling 97.6% of samples to be analyzed automatically. Clinical information including the name of the patient, code number, age, gender, department, the name of the clinician who ordered the tests, tests to be performed, clinical diagnosis, pathogenicity of the material and so on are all encoded on the label of the sampling tubes which are automatically labeled and sorted at the sampling division. The samples are sent to the appropriate analyzers according to the information described on their bar-code label by the sample distributor located in the sampling division. Following the preparation, samples are sent to each analyzer in an appropriate amount by the aliquoting machines (Figure 2). The remaining sample is sent to the sample keeper for re-analysis or additional examinations. Clinicians can get the report through the computer network or can receive a conventional printed report. Moreover, they can assess the progress of their patients at their office.
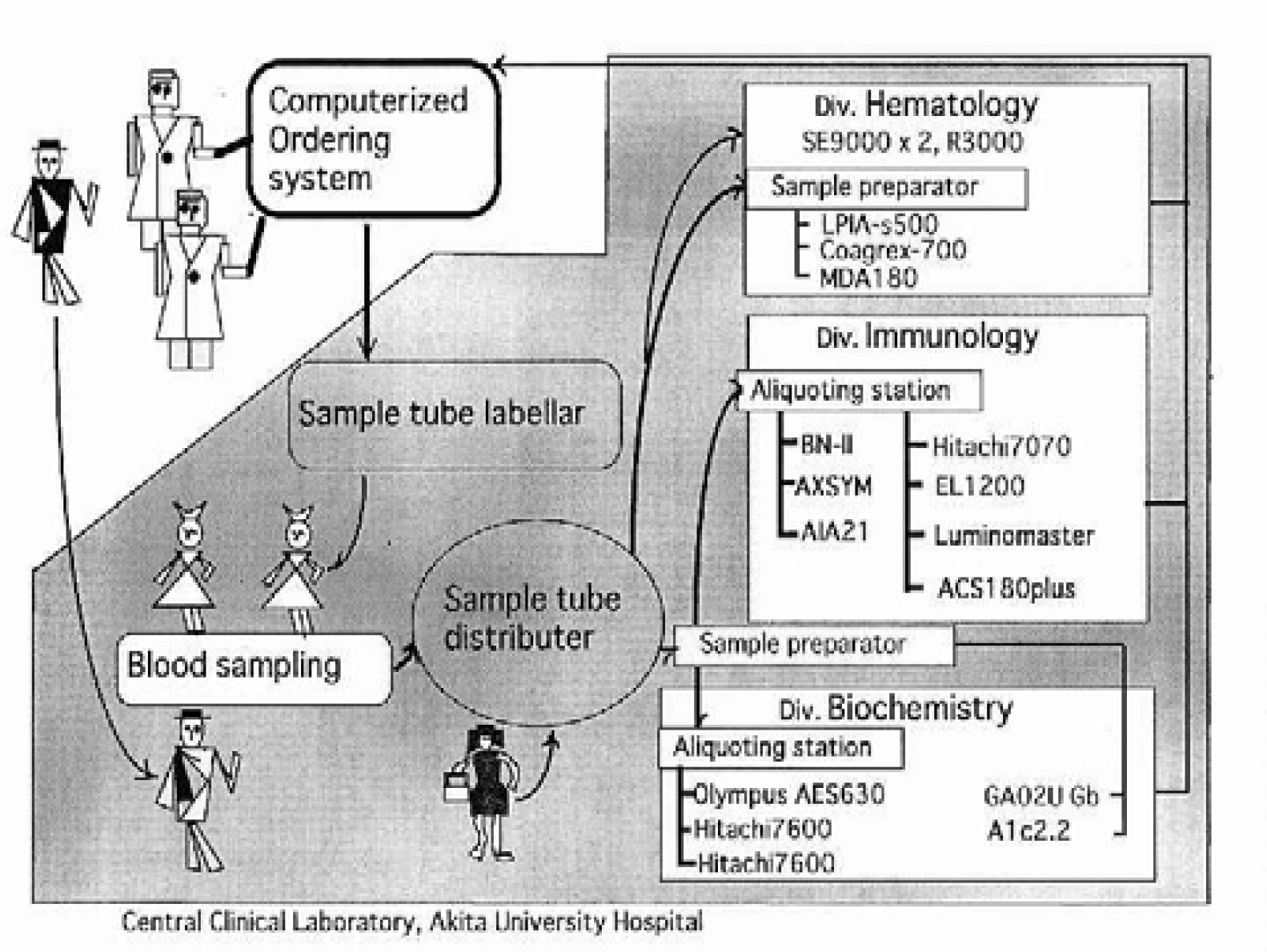
A schema of the automated clinical laboratory at Akita University Hospital. The reception office, the clinicians, the laboratory, and the accounting office are connected via computer network. The order of the clinicians and the clinical properties of the patients are sent to the division of sampling in the laboratory. The sample tubes are automatically labeled and sorted according to the order of the clinicians. After the sampling, the tubes are sent to the appropriate analyzers.
FUTURE PROBLEMS WITH LABORATORY AUTOMATION AT AKITA UNIVERSITY HOSPITAL
The laboratory automation at Akita University Hospital succeeded in saving manpower and time and improved the service for clinicians as well as patients; yet the following points are left as future problems.
Measurement of small samples
It is not possible to get a sample from neonates or small infants large enough for the automated analysis system. Even though small in amount, blood sampling itself can be invasive for neonates and small infants. Although almost all the usual laboratory examinations are accomplished with the automatic analysis system, concerning the difficulty in the sampling from neonates, it is desirable to minimize the amount of the sample required for the analysis. Samples from neonates or small infants require manual preparation before automatic analysis, and they require the use of sample tubes with a special design. Reduction of the quantity of samples and reagents reduces the cost of laboratory examinations.
Development of high-speed transportation and sample preparation systems
In the present system, the automatic analyzer Hitachi 7600 (Hitachi Ltd., Tokyo, Japan) requires no more than 10 minutes to get results. Yet, it requires more than 40 minutes for preparation and transportation before the samples reach the analyzers. The long transportation lines connecting the independently located analysis apparatuses are responsible for the loss of time before analysis. A compactly designed system with shorter transportation lines may shorten the waiting time.
Down-sizing of the system
The system in the division of chemistry takes up 200 m2 in the laboratory. The down-sizing of the system will make more room for specialized, off-line examinations.
OUTLOOK FOR THE CLINICAL LABORATORY
Further down-sizing of the system will make the clinical laboratory mobile or portable in the near future and will expand the working field of the clinical laboratory to remote areas and home-nursing services in the community (Figure 3). In Japan, simple tests such as blood pressure, blood glucose, urinary gonadotropins and peak flow have already come into wide use at home. With a simple and portable analyzer, it may be possible to know clinical markers for popular chronic diseases, such as liver functions, cholesterol and uric acid, at home. The rapid progress of the technology in clinical medicine is yielding highly specialized laboratory examinations. Together with computerized information networks, the progress in medical technologies will bring great changes to clinical laboratories.
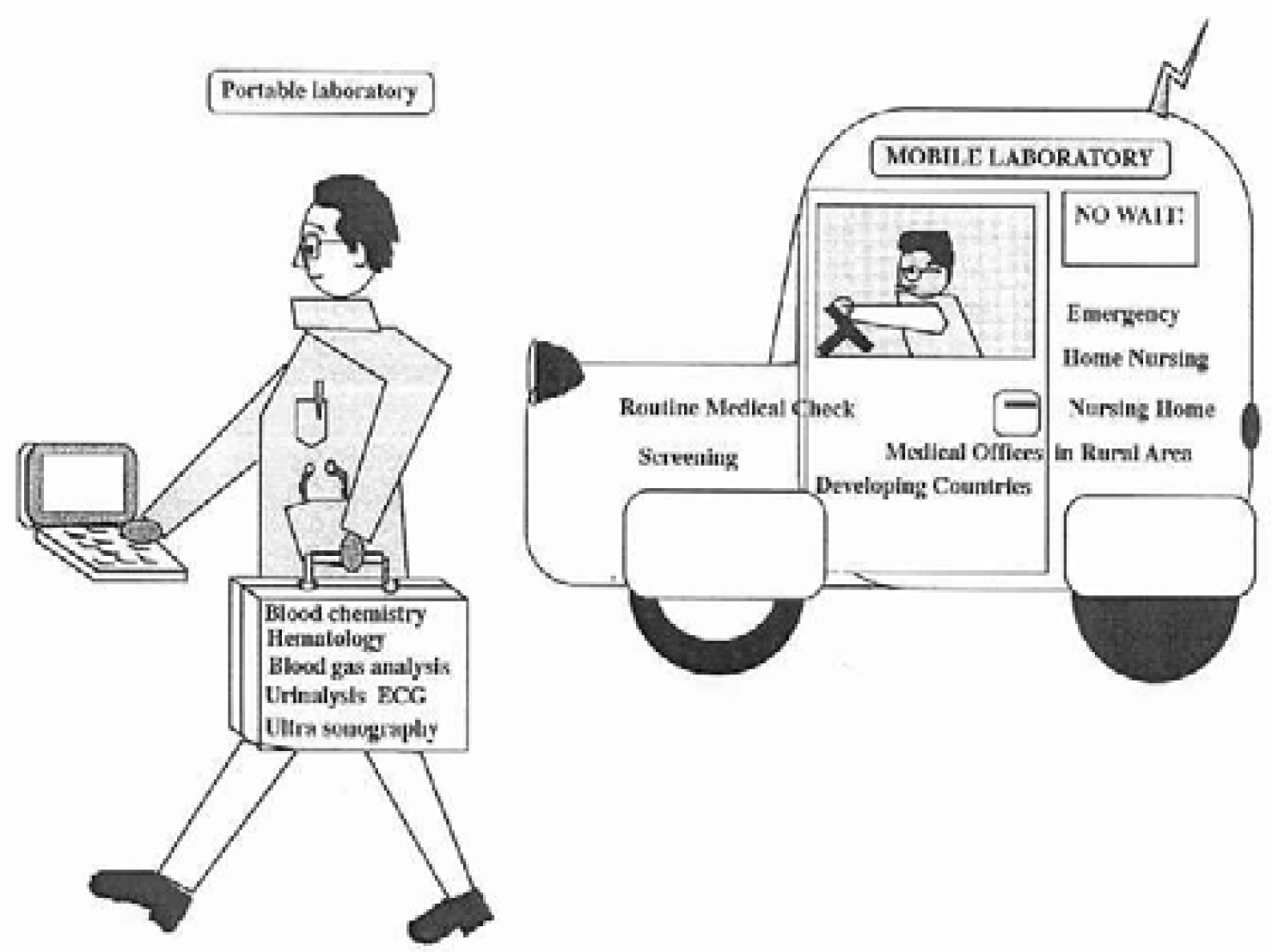
An example of the outcome of laboratory automation. The progress of laboratory automation and down sizing of the clinical laboratory results in a portable or personal laboratory. In some categories of laboratory examination, portable instruments for real-time analysis are already in use at clinics.
ACKNOWLEDGMENT
We dedicate this paper to the late Professor Shiro Uesugi, who was the head of the central clinical laboratory at Akita University Hospital, and one of the pioneers of laboratory automation in Japan.