
Abstract
Cytokines are soluble proteins produced by nucleated cells throughout the body. They have wide ranging effects on cell growth and differentiation, mediating immune responses, haemopoiesis and tissue repair. Advances in recombinant DNA technology have led to a vast increase in knowledge of their biological properties and subsequently their use in human clinical trials. The use of human cytokines in feline medicine has been of limited success as the action of cytokines is often species restricted or their activity may be neutralized due to antibody formation. Recently, however, many feline cytokines have been cloned which raises the possibility of their future use in the management and prevention of feline disease. Ultimately, they may find widespread clinical uses including the treatment of cancer, cytopenias and viral infections and as vaccine adjuvants.
The aim of this review is to present a summary of the potential clinical applications for cytokines and cytokine antagonists in feline medicine. A brief introduction to cytokines is followed by an overview of their biology in health and disease. A broad outline of their potential clinical applications is then considered. The limited clinical experiences with recombinant human cytokines in the treatment of feline diseases and future prospects for the use of feline specific cytokines are discussed. The scope of this article does not allow an exhaustive review of cytokines; the interested reader is therefore referred to other reviews and texts on the subject (Kruth 1995, Ogilvie 1995, Schijns & Horzinek 1997, Thomson 1994).
Cytokines are small proteins secreted by many cells, particularly those of the immune system, which enable intercellular communication. They are highly potent, acting via specific high affinity cell surface receptors to modify embryonic growth and differentiation, immune and inflammatory responses, and tissue repair and healing. The cloning of human cytokines using recombinant DNA technology has enabled their production in large quantities, allowing detailed study of their biological properties. An understanding of the biological effects of these cytokines has, in turn, led to their introduction as novel therapeutic agents with widespread potential uses, including the treatment of cancer, cytopenias and viral infections.
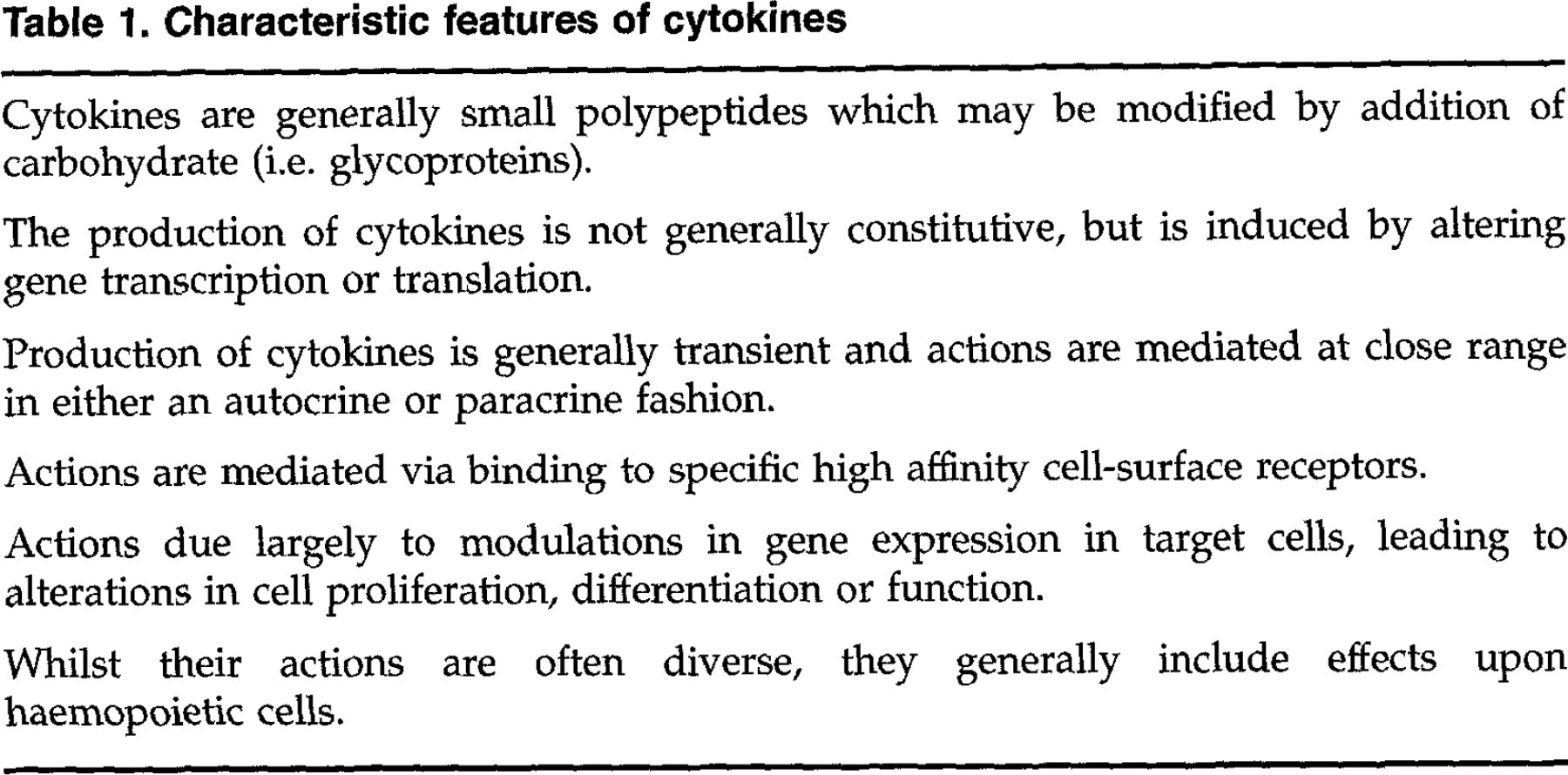
Due to the extremely diverse nature of cytokines and their effects, it is difficult to formulate a precise definition of what constitutes a cytokine. Vilcek & Le (1994) proposed a working definition of cytokines as ‘regulatory proteins secreted by white blood cells and a variety of other cells in the body; the pleiotropic actions of which include numerous effects on cells of the immune system and modulation of inflammatory responses’. This definition is necessarily vague, however, certain key features are common to many of the cytokines; these are outlined in Table 1. Major groups of cytokines include the interferons, haemopoietic growth factors, lymphokines (cytokines secreted by lymphocytes), monokines (cytokines secreted by monocytes) and classical growth factors.
Characteristic features of cytokines
The production of each cytokine is not generally limited to one specific cell type. The range of target cells and spectrum of actions of most cytokines is usually broad, leading to their description as pleiotropic. Additionally the spectra of actions of structurally dissimilar cytokines often overlap, leading to a large degree of redundancy. These features differentiate cytokines from the more classical endocrine hormones, which are produced by specialized cells, act at target cells at some distance and typically show distinct and specific effects.
There are a number of mechanisms that may increase the specificity of action of cytokines. Cells producing cytokines are generally located close to their target cells and act on neighbouring cells in a paracrine manner, or on the producing cell itself, in an autocrine manner (Metcalf 1991). A few cytokines, however, act in an endocrine manner, for example, erythropoietin. Cytokines are produced in small quantities, and production may be directed toward the responder cells (Poo et al 1988). Additionally, the effects of cytokines may be localized due to sequestering by extracellular matrix components or by their retention as cell membrane associated cytokines (Gordon 1991). Circulating, soluble cytokine receptors may further serve as a safety net to bind and therefore inhibit the action of cytokines that inadvertently reach the circulation (Heaney & Golde 1996). Furthermore, cytokine receptors may be expressed only transiently by target cells, providing a narrow window of opportunity for cytokine mediated responses.
On binding to its specific cell-surface receptor, a cytokine will initiate an intracellular signalling cascade that ultimately results in upregulation of gene transcription, protein expression and altered cellular function (Fig 1). The resultant cellular responses are numerous and depend upon a multitude of factors including the state of the target cell and interaction with other cytokines and mediators. It is important to note that due to the highly specific nature of cytokine-receptor interactions and the limited conservation of cytokines between species the activity of these agents is often species restricted.

Cytokine production may be induced by a number of stimuli, including antigen, toxins and other cytokines. The binding of cytokines to specific cell surface receptors generally leads to dimerization or oligomerization of receptor subunits. This initiates a cascade of intracellular signal transduction, involving multiple intracellular protein kinases, which culminates in changes in gene expression mediated by transcription factors. Altered gene expression leads to changes in protein synthesis, changes in cellular activity or cell proliferation.
The role of cytokines in health and disease
The physiological roles of cytokines are many, and it is only possible within this article to give an overview of those that may have most clinical relevance. On consideration of these, the potential for their clinical use in many different areas should become apparent.
Embryonic development and tissue differentiation
The importance of cytokines in embryonic development and organogenesis has been emphasized by studies using genetically modified mice deficient for a number of cytokine genes (‘knockout’ mice). Affected mice show various developmental abnormalities. For example, cytokines in the neuregulin gene family have been implicated in cardiac and neural development (Carraway 1996). Mice with mutations in the gene for stem cell factor or its receptor show abnormal embryonic migration and proliferation of primordial germ cells, melanoblasts and haemopoietic stem cells (Matsui et al 1990).
Regulation of haemopoiesis
Mature, circulating blood cells are all derived from a limited number of undifferentiated, pluripotent stem cells within the bone marrow. The survival and subsequent differentiation of these stem cells is dependent on cytokines [eg stem cell factor, interleukin-3, colony-stimulating factors (CSF)], produced by bone marrow stromal cells and haemopoietic cells themselves. In response to certain physiological stimuli, cytokines may mediate an increase in haemopoiesis over basal levels. Endotoxaemia, for example, associated with Gram-negative bacterial infection causes increased levels of a number of cytokines including interleukin-1β, interleukin-6 (IL-6) and granulocyte-CSF, the latter of which is a potent inducer of neutrophil production and release from the bone marrow.
Regulation of immune responses
Cytokines are critical to the development of an effective immune response against invading organisms and other immunogens. The coordination of both acquired and innate immunity requires the complex interaction of many different cytokines. For example, the development of either a T-lymphocyte (cell mediated) or B-lymphocyte (humoral) immune response depends largely on the interaction of immature B and T lymphocytes with T-helper lymphocytes. The T-helper (Th) lymphocytes produce a number of cytokines which lead to the differentiation of immature lymphocytes. Studies in mice have revealed two major functional subpopulations of lymphocytes: the Th1 subpopulation produces a number of cytokines including interferon-gamma (IFN-γ) and IL-2 and tends to promote a cell mediated immune response, whereas the Th2 subpopulation produces IL-4, IL-5 and IL-10 which affect B lymphocyte development and augment humoral immune responses [reviewed by Romagnani (1997)].
Regulation of acute and chronic inflammatory responses
Acute inflammation is characterized by both local (e.g. clotting and fibrinolysis) and systemic responses (e.g. pyrexia, leukocytosis, induction of acute phase proteins). Cytokines produced at the site of inflammation, predominantly by tissue macrophages, include IL-1, tumour necrosis factor alpha (TNF-α), IL-6 and IL-8. These and other cytokines mediate increased vascular permeability, upregulation of vascular endothelial adhesion molecules and are chemotactic for various leukocyte populations. This results in a marked ingress of leukocytes to the site of inflammation. The systemic acute phase response is also mediated in part by cytokines including IL-6, TNF-α and IL-1.
Chronic inflammation may occur in the presence of persistent antigen, with autoimmune or neoplastic disease. Undoubtedly, upregulation of cytokine expression, particularly IFN-γ, TNF-α and IL-1, is central to the catabolic events such as cachexia and tissue destruction that are associated with chronic inflammation. TNF- α and IL-1 have been implicated in mediating the excessive damage to articular cartilage that occurs with chronic osteoarthritis or rheumatoid arthritis [reviewed by Arend & Dayer (1995)].
Wound healing
Wound healing requires the co-ordination of a series of events involving cell division, migration and differentiation. A group of cytokines, collectively known as growth factors, including transforming growth factor beta (TGF-β), platelet derived growth factor (PDGF), basic fibroblast growth factor (bFGF), vascular endothelial growth factor (VEGF) and keratinocyte growth factor (KGF) play an integral part in this process. Collectively, they mediate migration of inflammatory cells and fibroblasts into the wound, stimulate cell proliferation, stimulate angiogenesis and vascularization and affect extracellular matrix production and degradation [reviewed by Greenhalgh (1996) and Slavin (1996)].
Clinical potential for manipulation of cytokine responses
Many cytokines interact in the body to maintain equilibrium of the immune status, with immunostimulatory cytokines being counteracted by inhibitory cytokines. During disease this balance is often lost with increased or decreased cytokine levels contributing to the pathogenesis of a number of disease states. Recombinant cytokines and their antagonists provide a novel means for manipulation of the immune system to either increase or decrease immune responses, tissue repair or inflammation, as appropriate.
The modulation of cytokine responses in disease is not a revolutionary idea. A number of conventional drugs mediate their actions via cytokine modulation. Glucocorticoids, for example, exert their immunosuppressive actions, at least in part, by suppressing the production of cytokines central to T-lymphocyte activation e.g. IL-1, IL-2, IL-6 and IFN-γ. Cyclosporin A has similar but more specific actions. Recombinant cytokines, however, can be produced in large quantities in cell culture and provide a more powerful means of manipulating immune and inflammatory responses. A vast number of potential clinical applications are becoming apparent as more of these cytokines are discovered and there is probably no area of medicine to which cytokine therapy cannot be applied. An overview of their potential clinical applications is shown in Table 2.
Strategies for manipulation of host cytokine responses and their potential clinical applications

The upper half of the table shows possible strategies for reducing or augmenting cytokine mediated actions. The lower half of the table outlines potential clinical situations where this may prove useful.
Haemopoietic growth factors may be used to treat anaemias or other cytopenias associated with chemotherapy, viral infections (eg feline immunodeficiency virus, feline leukaemia virus and feline infectious enteritis) or myelodysplasias. Immunomodulatory cytokines (eg IL-2, IL-12) may be used to augment the immune response to neoplasia or infectious diseases. Growth factors associated with wound healing may be used to accelerate healing or reduce scarring. Cytokines may also be used instead of conventional adjuvants in the development of vaccines.
Cytokines may be administered systemically or locally. Local administration generally more closely approximates the physiological situation and avoids potential adverse effects of systemic administration. In addition to therapy with recombinant proteins, alternative methods of delivery are under development and include administration of the DNA encoding the cytokine either in a bacterial plasmid (as ‘naked’ DNA) or viral vector (commonly used vectors include retroviruses, adenoviruses and poxviruses). The protein of interest is then produced by the body's own cells. This has been used in the development of vaccines against viral, bacterial and parasitic diseases, where the cytokine serves as an adjuvant, and in cancer immunotherapy [reviewed by Pasquini et al (1997)].
Other clinical situations exist where it may be desirable to inhibit cytokine mediated responses (Table 2). The activity of endogenous cytokines may be blocked by the use of anti-cytokine antibodies, soluble receptors, specific antagonists or ‘mutant’ proteins. Soluble receptors comprise the extracellular domains of their cell membrane associated counterparts which may bind and inhibit the activity of cytokines. The blockade of TNF-α using soluble receptors decreases morbidity and mortality in animal models of septic shock [reviewed by Dinarello et al (1993)]. An example of a natural antagonist of a cytokine is the IL-1 receptor antagonist protein (IRAP). Treatment with IRAP can prevent death due to septic shock and reduce the severity of inflammatory bowel disease and arthritis under experimental conditions; IRAP is currently undergoing clinical trials in humans [reviewed by Dinarello (1991)]. Mutant proteins may be engineered to bind to cytokine receptors without receptor activation, therefore acting as specific cytokine antagonists. Another method of specifically blocking cytokine production is to inhibit the translation of the cytokine gene by introducing a complementary nucleic acid sequence into the cell (antisense therapy). The complementary nucleic acid binds to cytokine messenger RNA in the cell, preventing its ribosomal translation and consequent protein expression.
Whilst many of these approaches are, at present, largely experimental, limited experience has already been gained with the use of several cytokines in the treatment of feline disease.
Use of cytokines in feline medicine
Erythropoietin
Recombinant human erythropoietin (r-huEPO) has been used in cats to treat the non-regenerative anaemia that accompanies moderate to severe chronic renal failure. Administration of r-huEPO increases RBC and reticulocyte counts leading to clinical improvements in treated animals. This is manifested by improvements in appetite, weight gain and decreased morbidity (Cowgill et al 1998). Adverse effects are seen inconsistently. These include hypertension and iron deficiency which are attributed to increased erythropoiesis, and seizures, thought to be secondary to adaptive mechanisms to increased red blood cell (RBC) mass. In a significant number of patients, a non-regenerative anaemia is seen, which may be more severe than the pre-treatment anaemia, but resolves following cessation of r-huEPO therapy. This is attributed to development of antibodies to the heterologous recombinant cytokine, which block its bioactivity. The antibodies also cross-react with endogenous feline erythropoietin, hence the tendency for anaemia to fall below pre-treatment values. Upon cessation of treatment, RBC counts rise to pre-treatment values, presumably associated with a waning of anti-r-huEPO antibody levels.
Granulocyte colony-stimulating factor
Granulocyte colony-stimulating factor (G-CSF) is a lineage specific haemopoietic growth factor acting principally upon granulocyte progenitor cells and mature neutrophils to increase circulating neutrophil counts and upregulate effector functions such as chemotaxis and phagocytosis. Administration of recombinant human G-CSF to normal cats has been shown to produce a rapid increase in peripheral blood neutrophil counts (Fulton et al 1991). Peripheral blood neutrophil counts peaked at approximately four-fold pre-treatment levels after 10–14 days treatment (3–10 μg/kg subcutaneously twice daily). Prolonged use, however, led to a decrease in neutrophil counts to the normal range, seen after 19–21 days. This, again, is probably due to antibody formation to the heterologous cytokine. Administration of recombinant canine G-CSF produced similar elevations in neutrophil counts of normal cats (Obradovich et al 1993). However, neutrophil counts remained elevated until treatment was stopped at 42 days, suggesting that production of neutralizing antibody to the recombinant cytokine did not occur. Unfortunately, the recombinant canine cytokine is not commercially available at present.
Potential clinical applications for G-CSF include the treatment of animals with neutropenia associated with retroviral infections, viral infections of the respiratory tract and severe myelosuppression due to chemotherapy or radiotherapy. In the immunosuppressed patient the potential for antibody formation to a recombinant cytokine is likely reduced. This has been shown in dogs receiving mitoxantrone and cyclophosphamide chemotherapy (Goodman et al 1990). Thus r-huGCSF may have greater clinical potential in immunosuppressed cats, with less side effects than suggested by preclinical studies. In one study, the use of r-huG-CSF in neutropenic cats with viral panleucopenia, cat flu or severe bacterial infections resulted in increased peripheral neutrophil counts although no effect was seen in cats with neutropenia secondary to retrovirus (FeLV or FIV) infections (Kuffer-Frank & Kraft 1998). Further work is required to assess the effect on survival and morbidity in treated cats.
Interferon alpha
Interferons have, by definition, well recognized inhibitory effects on viral replication. They also have potent immunomodulatory actions, including enhancement of macrophage and natural killer cell activity. However, the dose and route of administration may alter specific actions, for example, low doses of interferon alpha (IFN-α) enhance lymphocyte proliferation and antibody formation whilst high doses are inhibitory. Small scale trials have shown the ability of combination treatment of FeLV infected cats with human IFN-α, infusion of activated lymphocytes and the antiretroviral drug zidovudine to reverse viraemia (Zeidner et al 1995).
Interleukin 2
Interleukin-2 (IL-2) is a key cytokine in the regulation of T-lymphocyte immune responses. Following antigen stimulation, antigen presenting cells (e.g. macrophages, dendritic cells) produce IL-1 and other co-stimulatory molecules which induce the production of IL-2 and the IL-2 receptor by T lymphocytes. IL-2 receptor activation thereafter induces proliferation of specific T-lymphocyte clones. IL-2 also stimulates natural killer cell production and B lymphocyte immunity. There has been much interest in the potential for recombinant IL-2 to invoke anti-tumour immunity, leading to tumour regression. Recombinant human IL-2 has been used with some success in the treatment of human patients with renal cell carcinoma and malignant melanoma (Bukowski et al 1993, Foa et al 1992). However, the problems of using cytokines systemically are well illustrated with reference to experiences with IL-2. Side effects are common and include pyrexia, anaemia, shock, respiratory distress due to pulmonary oedema, coma and death. These problems may largely be avoided by the administration of the cytokine locally. For example, cats with fibrosarcoma have shown less frequent relapses and longer survival times when treated with surgery, radiotherapy and the local injection of a human cell line expressing human IL-2, in comparison to animals receiving surgery and radiotherapy alone (Quintin-Colonna et al 1996).
Future prospects
The use of recombinant human cytokines in cats has been of only limited success, as suggested above, in part due to limited conservation of these proteins between species and their consequent poor efficacy or tendency for the development of neutralizing antibodies. In order to fully realise the potential of cytokines as therapeutic agents and to facilitate further studies into the role of cytokines in feline disease, the isolation of cytokines specific to this species is desirable. At the time of writing the study of feline cytokines is in its infancy. Isolation of feline cytokine genes enables determination of their nucleotide sequence which permits techniques such as quantitative analysis of messenger RNA levels to be used to study the role of cytokines in feline disease. Once cloned the cytokine protein can be expressed in vitro and antibodies to the cytokines may be produced; both the in vitro and in vivo effects of the cytokine may then be investigated. Ultimately a number of cytokines are likely to form a new array of therapeutic agents to treat feline disease. Table 3 shows those feline cytokines which have been cloned and appear in the European Molecular Biology Laboratory (EMBL) DNA database. This work lays the foundations for many future projects and it is likely that a wealth of new information will appear over the forthcoming years in both basic and applied feline medicine.
List of feline cytokine DNA sequences which appear on the European Molecular Biology Laboratory's sequence database

This may be accessed via the Internet at the URL http://www.ebi.ac.uk.
Unfortunately the production of recombinant cytokines in large quantities is extremely expensive and it is likely that these agents will remain available for research purpose only for the foreseeable future. With advancements in technology, however, and the utilization of alternative methods of delivery such as naked DNA injection, costs may decrease and a number of cytokines may become available for clinical use.