Abstract
Abstract
Introduction
Patients with neuromuscular disorders are not able to adapt their sitting posture continuously. Seating devices, like seating orthoses, braces, seating shells, and custom-made cushions for wheelchairs, however may improve their quality of life by stabilizing their pelvis and trunk. Sitting should be regarded as a dynamic process regulated by motor reactions of trunk and pelvic muscles due to endogenic and exogenic influences.
Methods
Prerequisites for the indication of high-quality and cost effective seating devices are guidelines for planning and fitting which consider both pathomorphologic mechanisms and the patient's personality. In order to avoid functional problems and pain caused by an insufficient seating device it is necessary to pay attention to the exact indication, time, and combination of technical options. Planning within a seating clinic needs teamwork. Primarily the goal of treatment is defined; it depends on the functional deficit, on the daily living activities of the patient, and on the social environmental factors. Secondly, fitting of the devices follows defined treatment guidelines.
Conclusion
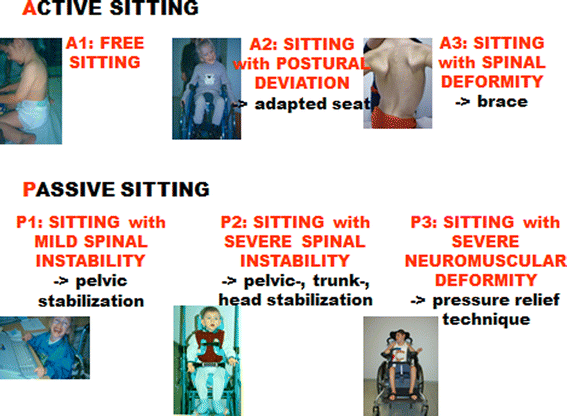
By examination of the sensor and musculoskeletal system, it is possible to classify the patient's sitting or seating ability for simplifying indication: three groups of ACTIVE sitters who are able to change position of trunk and pelvis actively are differentiated from three groups of PASSIVE sitters who have to be seated.
Keywords
Normal sitting
Sitting is a typical posture of the resting human body which allows an individual to reduce energy consumption while being involved in communication, eating or working by using his hands. Sitting allows us to use our upper extremities in an intensive and concentrated way [1]. Sitting postures may be differentiated according to cultures, geographic regions, religious or traditional activities. Accordingly, devices built for the support of sitting postures differ in the same ways [2].
Biologically, sitting is defined as a dynamic process regulated by motor reactions due to endogenic and exogenic influences.
Like standing upright and walking, the ability to actively sit results from the refined performance of the human neuromusculoskeletal system, which has been developed by an evolutionary process.
Prerequisites of this development are the special shape and function of the human pyramidal system and human brain. The considerable increase of hip extensor power and corresponding muscle growth due to the body's upright position are also important factors in the possibility of long sitting periods in daily life [3].
Physiologically, the neuromusculoskeletal system allows for continuous adaptation of sitting posture to exogenous and endogenous influences. Thus, active sitting occurs unconsciously.
Permanently trunk and pelvic positions actively change between a front, straight seat position stabilised by power of the spine extensors (“readiness position”), a middle, relaxed position, stabilised by the ligament apparatus of the spine (“resting position”), and a rear position, stabilised by a weight shift to the sacral bone of the spine (“weight-shift position”). See Fig. 1.
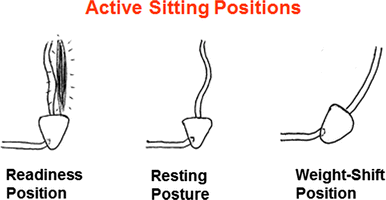
Sitting positions that can only be controlled by ACTIVE sitters and should be simulated by swivelling frames for seating shells
Sitting posture in cerebral palsy
In patients with cerebral palsy sitting may be compromised by lack of motor control and weakness of those muscles which should stabilise the trunk and pelvis. Severity of sitting disorders depends on the course of the disease.
Commonly these patients are handicapped by severe sitting disabilities due to spasticity, hypotonia, dystonia, ataxia, and over time, by developing secondary musculoskeletal deformities [4].
Problems usually are described as decreased upper extremity function, lack of head control, increased deficit of sensory functions, reduced time of sitting posture, back pain, and pressure sores [5].
Progressive fixed musculoskeletal deformities like scoliosis, kyphosis, hip dislocation, pelvic obliquity, severe muscle shortening, hip extension contracture, etc. considerably aggravate the patient's seating and positioning problems [6].
Diagnostic tools of the seating clinic
Screening programs should be provided for all patients with neuromuscular disorders. Consultations should include a check-up of daily living activities, gross motor function, sitting posture, sensory and communication possibilities, hand function, head control, muscle length and strength, spasticity, pressure sores, pain, and function and shape of spine, hip and feet [7].
Documentation is recommended by using GMFCS scale, Goal Attainment Scale, Tardieu or Ashworth scale, Oxford scale for muscle power of upper extremities, clinic muscle tests additional to ROM for lower extremities, X-rays of spine and hips, photographs of seating posture, and video analysis of upper extremity function.
Problems and new chances concerning sitting and positioning should be discussed. Treatment goals have to be defined by the team. Most important goals are improved trunk stability in weak patients and increased range of movement as well as reduced muscle tone for hyperactive, spastic, or dyskinetic kinds of diseases [8].
Establishing a seating clinic has become a main task for neuroorthopaedic treatment centres [9]. Members of the seating clinic's team are patients, parents or caregivers like nurses, physical therapists, occupational therapists, orthopaedic technicians, neuroorthopaedists, and neuropaediatricians or neurologists.
Professionals should be trained to work together regularly, using the same language, and translating it to the patients. Their task is to analyse problems, define the goal of treatment and create a rehabilitation plan for how to get there. Seating is an important part of that plan. This plan is composed of interventions immediately improving daily living activities whereas others may require more time or even associated therapy [10].
The team should always agree on the best possible individual seating concept. They need to conclude and document their recommendations using any kind of standardised form, such as the Goal Attainment Scale, for follow-up and evaluation.
Re-evaluation, adaption of seating units and prescriptions for new devices should be considered once a year and every 6 months for the growing child.
Principles of seating
Indication for the best individual seating system belongs to the most challenging tasks of specialists in neuroorthopaedics.
Biomechanical and technical orthopaedic fundamentals, medical essentials and the requirements according to occupational and physical therapists have to be considered as well as the needs and desires of the patient and the parents [11].
The optimum outcome is a comfortable seating device improving function that helps the patient to increase his participation in social life. It should include an upright position of the trunk with a balanced head position [12]. The pelvis should be positioned in three dimensions, physiologically with bilaterally flexed and slightly abducted hips. A fixed windswept deformity requires an asymmetric seating position. A flexible windswept deformity has to be corrected by sufficient pelvic fixation [13].
Optimal pressure distribution by a surface as large as possible reduces the risk of pressure sores.
One of the main goals of seating is to achieve free function of upper extremities and reduced spasticity of trunk and extremities. Sitting should be comfortable for several hours.
Care and transfers should be eased so that they can be performed by a single person only. The devices should provide enough flexibility and stability for daily life functions, and they should comply with hygienic and aesthetic standards [14].
Classification of sitting ability and recommendations for special devices
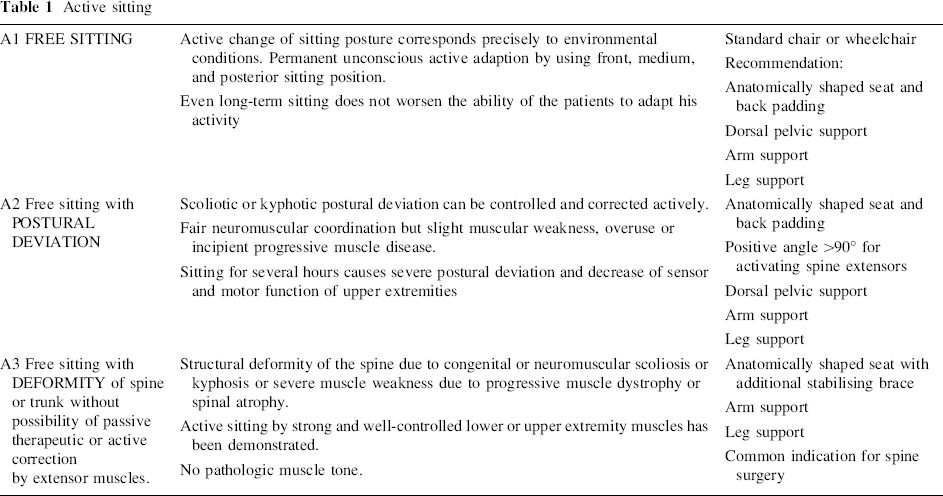
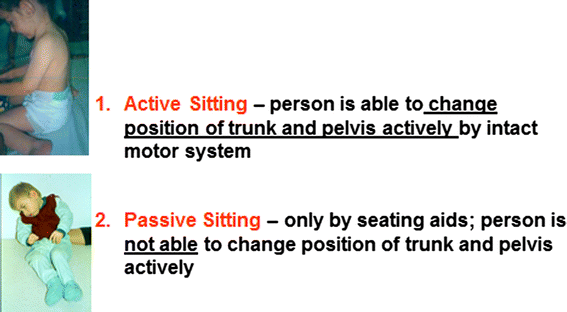
ACTIVE SITTING is defined by the ability of the patient to control his trunk and pelvic muscles actively by an intact motor system. This allows for continuously adapting the sitting posture to the environmental conditions. Patients are able to sit ACTIVELY [15]. See Figs. 2 and 3.
Active sitting
Definitions and examples for ACTIVE sitting–PASSIVE seating
Overview: classification of sitting ability and recommendations for special devices
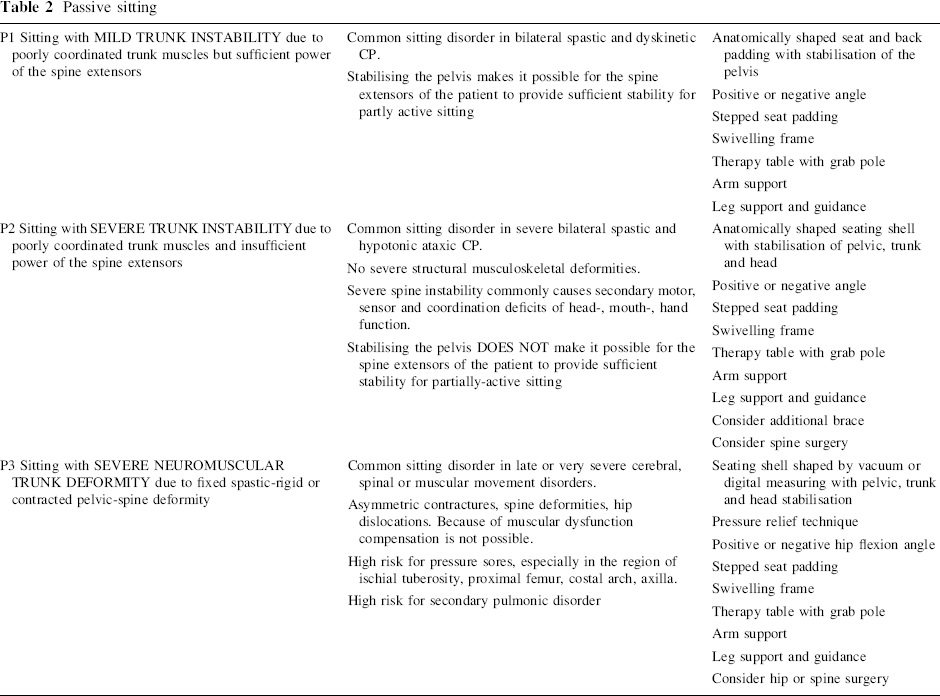
PASSIVE SITTING is defined by the patient's inability only to be SEATED by supporting seating aids. He is not able to change the position of trunk and pelvis actively due to a disorder of the motor system. Trunk, pelvic and lower extremity muscles cannot be moved voluntarily or are done so inadequately. Without seating aids the patient would slide to a severe asymmetric posture or would drop out of the chair. Such patients have to be seated PASSIVELY (Tables 1 and 2).
Passive sitting