
Abstract
Abstract
Objectives
In the last 2 decades, BTX-A is increasingly being used in the management of spasticity in children with Cerebral Palsy (CP) and there is no doubt about its effect on range of motion, spasticity reduction and gait pattern in this patient population. However, in daily practice, there is still an ongoing search for the best way to apply BTX-A. Two studies were set up to evaluate how successful an integrated multilevel treatment approach is in children with CP. The first study identifies crucial factors within the treatment strategy which may predict the outcome. The second study evaluates the efficacy of repeated BTX-A injections.
Methods
Patient selection was based on following criteria: diagnosis of CP, lower limb BTX-A treatment, age at time of treatment <24 years, no combined surgery at the time of BTX-A injections, 3D gait analysis and clinical evaluation pre and 2 months post BTX-A injections. The first study included the last treatment of 577 patients. In the second study, the first and last BTX-A treatment of 222 children were included. The Goal Attainment Scale (GAS) was used to evaluate the functional outcome of each treatment session.
Results
In the first study, the mean GAS score of the total group was 51.7 (±7.5). Considering a converted total score of 50 as cut-off score for successful treatment, 67.1 % of the treatments were successful. Significantly higher GAS scores were found in mildly involved children compared to more involved children (p < 0.0001) and for multilevel injections or injections in the distal muscle groups only compared to injections in the proximal muscles of the lower limb only (p < 0.0001). Other crucial factors for a successful outcome were amount of physical therapy per week (p=0.0026), post injection casting (p=0.005) and frequency of using day and night orthoses after injection (p < 0.0001). In the second study, the mean GAS score of the total group decreased from 54.8 (±6.8) at the first treatment to 50.7 (±6.9) at the last treatment, indicating that on average, repeated BTX-A treatment is successful.
Conclusion
The integrated multilevel BTX-A approach is successful in children with CP. Several factors might help the clinician to select patients that are most likely to benefit from the treatment, to assure the most optimal treatment strategy and to predict the outcome. Each treatment should be carefully planned and goals should be well chosen, because the effectiveness of the BTX-A treatment may decrease with increasing number of treatments in the same patient.
Introduction
Botulinum toxin A (BTX-A) is a neurotoxin that, when injected into the muscle, affects the neuromuscular synapses by inhibiting the release of acetylcholine. This causes spasticity reduction in a safe and selective way. The effect is reversible and the period of clinically useful relaxation is usually 12–16 weeks [1, 2]. However, Schroeder et al. [3] found that structural alterations in the muscle are present up to 12 months after BTX-A injection into the lateral head of the gastrocnemius muscle. This should be taken into consideration when repeated BTX-A injections into the same muscle are planned. Furthermore, the effect of BTX-A is dose dependent, and the reduced muscle tone allows combined treatment with orthoses, casts, and intensive physiotherapy.
Cerebral palsy (CP) is characterized by tone problems, which affect activities of daily living. The Surveillance of Cerebral Palsy in Europe network divides CP into three subtypes: spasticity, dyskinesia, and ataxia [4]. With a prevalence of more than 80 %, spastic CP is the most common subtype [5]. Spasticity is the main cause of the development of bony deformities and muscle contractures [6]. Since spasticity is present at a young age, the treatment should be started early. In the last two decades, BTX-A has increasingly been used in the management of spasticity in children with CP, and there is no doubt about its efficacy in this patient population. Several studies have shown a positive effect on range of motion [7], spasticity reduction [8, 9], and an improved gait pattern [10, 11]. However, in daily practice, there is still an ongoing search for the best way to apply BTX-A.
Methods
Since 1996, at the University Hospital of Pellenberg, an integrated multilevel treatment approach has been applied. The fundamentals of this integrated approach are proper muscle selection, an appropriate dosage, and an accurate injection technique [6].
Proper muscle selection
An extended clinical evaluation with validated tools can be used to measure range of motion, spasticity, muscle strength, and selectivity. However, Desloovere et al. [12] found a low correlation between this extended clinical evaluation and three-dimensional gait analysis. Even a combination of several clinical measures was not able to accurately predict gait parameters. This problem can be partly explained by the role of biarticular muscles during walking and by the fact that spasticity is velocity dependent. Most of these clinical problems, however, are well documented by (integrated three-dimensional) gait analysis, which describes the segmental movements in all anatomical planes. This allows the pathological gait pattern of an individual patient to be compared with that of typical developing peers. It is also important to gain insights into the main power sources that cause movement. These insights can be obtained from kinetics and integrated electromyography, identifying the responsible muscles. A combination of an extended clinical exam and a gait analysis or video evaluation is therefore essential to select the right muscles.
An appropriate dosage
The first studies on BTX-A treatment of spasticity associated with CP were originally restricted to the treatment of equinus. However, a child with CP rarely presents with an isolated problem of spastic equinus; there are usually has problems on multiple levels (pelvis, hip, knee, and ankle). Many of the common gait patterns in CP can only be adequately treated if several muscles are addressed simultaneously in one treatment session. Therefore, multilevel treatments are more appropriate. As several muscles are injected simultaneously within one treatment session, multilevel treatments may require a higher total dosage when compared to single-level treatments to gain optimal treatment outcomes. The treatment approach does not include standardized total dosages. Instead, the total dosage is defined by the standardized dosages per muscle group. The dose injected in one muscle is dependent on the muscle volume, the amount of spasticity, and the degree of involvement of the muscle in the pathological gait pattern.
Accurate injection technique
Ultrasonography with or without EMG guidance or electrical stimulation is the most appropriate technique for localizing and identifying the muscles to be injected, especially for the smaller muscle groups [13]. Since the effect of the toxin relies on uptake by the presynaptic membrane of the motor endplate (MEP) at the neuromuscular junction, injections should be given into the MEP area [14, 15]. The review of Van Campenhout et al. [16] summarizes all of the available knowledge on the localization of the MEP zones from frequently injected muscles of the lower limb.
Once these fundamentals have been established, it is clear that other factors are crucial in achieving successful outcomes [6]. The duration of the effect of a BTX-A treatment is mainly determined by the pre- and post-injection care, which consists of intensive physical therapy, orthotic management, and casting. To set up a long-term treatment plan, appropriate patient selection with ideal timing and individually defined goal settings is crucial to obtaining successful results from BTX-A treatment. Finally, once the treatment is completed, the outcome should be critically evaluated to improve the outcome and plan for future treatment.
Results and Discussion
Two studies were set up to verify if this integrated treatment approach is the right way to use BTX-A in children with CP.
The aim of the first study was to evaluate the clinical responsiveness of lower-limb BTX-A treatment in children with CP and to delineate crucial factors within the treatment strategy which may predict the outcome. From a database of all BTX-A treatments (N = 2276) at the University Hospital of Pellenberg between January 1996 and December 2006, 1,090 treatments were selected based on the following criteria: diagnosis of CP, age at time of treatment <24 years, lower limb treatment, no surgery at time of BTX-A injections, standardized three-dimensional gait analysis, and clinical evaluation before and 2 months after the BTX-A injections. Only the last treatment for each patient was included for further analysis, resulting in a final set of 577 treatments. Because of the variety of treatment goals for BTX-A treatment, the Goal Attainment Scale (GAS) was used to evaluate the efficacy [17]. Analysis of variance (ANOVA; post hoc Tukey) and the Kruskal–Wallis test were used to evaluate differences in group characteristics for continuous and categorical data.
The mean GAS score of the total group was 51.7 ± 7.5 (Table 1). Considering a converted total score of 50 as the cut-off score for successful treatment, 387 of the 577 children (67.1 %) reached the expected GAS score of 50 or more, whereas 190 children (32.9 %) did not meet this cut-off score. The frequency distribution of GAS scores for the total group is presented in Fig. 1.
Patient and treatment characteristics
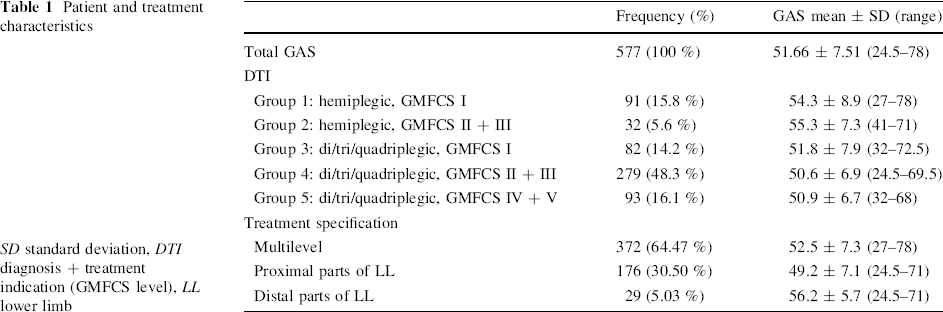
SD standard deviation, DTI diagnosis + treatment indication (GMFCS level), LL lower limb
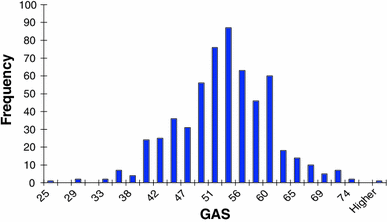
Histogram of GAS scores for the total group (N = 577)
Information about the GAS scores in relation to patient and treatment characteristics is provided in Table 1.
Patient characteristics (diagnosis and GMFCS level) seem to affect the outcome. Significantly higher GAS scores were found in mildly involved children (group 1 and 2) compared to more involved children (group 4 and 5; p < 0.0001).
The GAS was significantly lower in the group that was treated proximally compared to the multilevel-treated group and the group who were only injected in the distal muscles of the lower limb (p < 0.0001).
A significant, but low, negative correlation was found between GAS and age at time of treatment, which means that younger children had higher GAS scores (r s = −0.21, p < 0.001).
The mean total dosage per treatment session was 18.6 ± 6.5 U/kg body weight. No significant correlation between total dosage and GAS score was found (r s = 0.0144, p = 0.7319). This may be explained by the general strategy for dosage per muscle, where the dosage per muscle depends on the muscle involvement, the muscle volume, and the amount of spasticity.
Aftercare also influenced the outcome (Table 2).
Aftercare characteristics
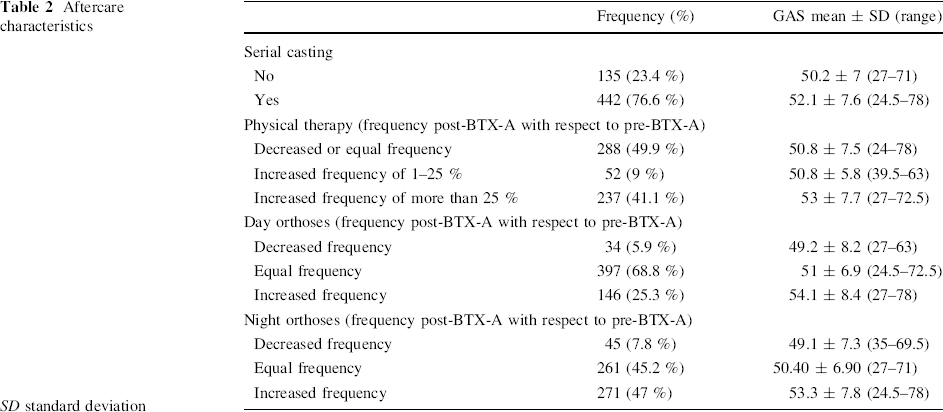
SD standard deviation
Children who received casts after BTX-A injection had a significantly higher mean GAS score than children who did not receive a combined treatment of BTX-A with casts (p = 0.0057).
The group of children with an increased frequency of >25 % of physical therapy after BTX-A treatment had a significantly higher GAS score than those with an equal or decreased frequency of physical therapy (p = 0.0026).
A significantly higher GAS score was found for children with an increased use of day orthoses after BTX-A treatment in comparison with children who wore their orthoses with an equal or decreased frequency (p < 0.0001).
Children with an increased use of night orthoses also scored significantly higher on GAS compared to children who wore their orthoses with an equal or decreased frequency (p < 0.0001).
The results of this study confirm the effectiveness of BTX-A treatments of lower limb spasticity in children with CP. This study highlighted several factors that might help the clinician to select patients who are most likely to benefit from the treatment, to assure the most optimal treatment strategy, and to prognose the outcome. BTX-A injections should not be considered as an isolated treatment. The results indicated that, apart from treatment specifications, aftercare issues such as casting, physical therapy, and orthotic management also significantly influence the outcome.
In a subsequent study, the aim was to evaluate the efficacy of repeated BTX-A injections in children with CP who were administered according to the integrated high-dosage treatment strategy. From a database of all children who received at least two BTX-A treatments at the University Hospital of Pellenberg between January 1996 and December 2006, 222 children (444 treatments) were selected based on the following criteria: diagnosis of CP, age at time of treatment <24 years, lower limb treatment, no surgery at time of BTX-A injections, standardized three-dimensional gait analysis, and clinical evaluation before and 2 months after each BTX-A injection. The GAS score was used to evaluate the functional outcome of each treatment session. Differences between the GAS scores of the subgroups were analyzed using the unpaired t test.
The mean GAS score of the total group decreased from 54.8 (±6.8) at the first treatment to 50.7 (±6.9) at the last treatment, indicating that, on average, repeated BTX-A treatment remained successful. The total group was divided into three subgroups. For the subgroup of children who received two sessions of treatment (N = 95), the mean GAS score decreased from 52.7 (±6.1) at the first session to 50.9 (±6.6) at the second session (p < 0.05). For a second subgroup of 51 children with a history of three treatment sessions, the average GAS decreased from 54.5 (±5.4) at the first session to 51.3 (±7.9) at the third session (p < 0.05). The final subgroup of 76 children who received at least four treatment sessions had an averaged GAS of 57.7 (±7.4) at the first treatment, which significantly decreased to 49.9 (±6.7) at the last treatment session (p < 0.0001).
There was a similar distribution of diagnosis (hemiplegia, diplegia, quadriplegia) in the three subgroups. However, group differences were seen for functional level (GMFCS): 57.9 % of the children who received at least four treatment sessions were classified as GMFCS III, IV or V, as compared to 42.1 % of the children who received two BTX-A treatments.
At the first treatment, the majority of the children (>70 %) received a multilevel treatment in all subgroups (Fig. 2). For the last treatment session of the group who received at least four treatments, the treatment was more frequently (40.7 %) focused on the proximal muscles of the lower limb (targeted treatment).
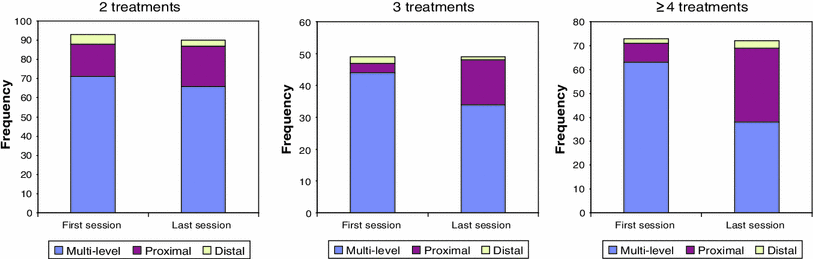
Treatment characteristics per subgroup
This study indicated that repeated BTX-A can be considered successful when treatment goals remain carefully chosen. The largest functional improvement can be achieved at the first treatment session. After multiple treatment sessions, a change in strategy may influence the outcome. Moreover, children who receive multiple injection sessions are more involved (have higher GMFCS levels).
Conclusion
In conclusion, we can say that the multilevel BTX-A treatment approach is successful in children with CP. Nevertheless, each treatment should be carefully planned and goals should be well chosen because the effectiveness of the BTX-A treatment may decrease as the number of treatments increases in the same patient. This decrease may be attributed to the severity of the pathology and the development of secondary problems caused by spasticity or weakness. Therefore, “reflection is more important than injection” remains a useful statement.