
Abstract
Abstract
Purpose
To prospectively evaluate long-term effects of repeated botulinum toxin A (BTX-A) injections in children with cerebral palsy (CP).
Methods
Repeated injections of BTX-A were offered to children with CP, according to clinical indications, for a maximum of four injections within a period of two years. Injections were administered into lower extremity muscles of 26 consecutive children (age 3.7 ± 1.2 years, 16 boys) with hemiplegic or diplegic CP. Clinical assessments before and one month following each injection included a gross motor function measure (GMFM), a modified Ashworth scale, and range-of-motion of knee extension and ankle dorsiflexion.
Results
Twelve children received two injections, six received three injections, five received one injection, and three received four injections. The most common reason for discontinuing treatment was the need for orthopedic surgery (n = 17). A long-term effect was demonstrated by a significant increase of the GMFM score before the first injection compared with the last injection for each patient (P < 0.0001). There was no comparable change in the muscle tone or range-of-motion. The mean rate of GMFM change during the study was significantly higher than literature norms for CP children (13.2 vs. 5.37 per year, respectively, P < 0.01). The increase of the GMFM score before and one-month after injection (short-term effect) was significantly higher after the first injection than after the last injection (P < 0.05). Similar results were found for the Ashworth scale and popliteal angle.
Conclusions
Botulinum toxin A injections have a long-term effect on gross motor function in children with CP even though the effect on muscle tone is short-term. The effect apparently declines with repeated injections, with most children benefitting from 2 to 3 injections.
Introduction
Botulinum toxin A (BTX-A) has proven to be effective in the treatment of childhood spasticity, particularly cerebral palsy (CP). Considerable data have now been gathered from many randomized and placebo-controlled studies to support the use of BTX-A for this condition [1–7]. Functional gains, however, have been more difficult to demonstrate [8]. Because the effect of BTX-A lasts for a few months only, several injections are necessary to achieve a longer-lasting effect.
The results of repeated injections in pediatric CP patients have been addressed in the literature in a few case series and clinical trials. Injections of BTX-A repeated every three months have proven to be safe and effective in chronic management of focal muscle spasticity in children with equinus gait [9]. A strong correlation was found between duration of response and the dynamic component in children undergoing repeated gastrocnemius muscle injections [10]. Another clinical trial [11] described significant improvements of the gait parameters after the first and second injections in children with spastic equinus foot. Those authors found a decrease in the duration of response after the third and fourth injections, which they suggested was probably caused by an increase of the dynamic equinus component with age [11]. In a prospective, randomized, placebo-controlled study, Sutherland et al. [12] injected botolinum toxin type A in a group of children with CP twice, with a four-week interval, and found significant improvement in ankle dorsiflexion. In a three-center retrospective chart review by Gormley et al. [13], the reason for the longest interval between injections at one site was because BTX-A was re-injected when the return of muscle tone began to interfere with function rather than when it returned to previous levels. In another site the mean interval between injections had been longer than the average of 3–6 months reported in the literature. The authors explained that this was related to the higher doses of BTX-A injected at this site.
Another long-term retrospective case study [14] reviewed 13 patients (5 children and 8 adults) with spasticity who had been treated with BTX-A for three years. Repeated injections, reaching a group total of 38, were administered to the same muscle sites each time. Treatment goals were achieved in 10 of 13 patients, with response rated as “good”, in 100% of the children [14]. In another study that compared BTX-A injection and selective posterior rhizotomy in children with CP [15], the BTX-A group demonstrated rapid improvement post-treatment but the improvement became insignificant 12 months later, even with repeated BTX-A injections at four-month intervals [15].
The objective of this study was to prospectively evaluate the long-term effect of repeated injections of BTX-A in children with cerebral palsy (CP).
Materials and methods
This work is a prospective follow-up study designed to evaluate the long-term effect of repeated intramuscular injections of BTX-A for management of spasticity in pediatric CP patients. Consecutive patients of our CP clinic who met the inclusion criteria were enrolled into the study. Patients were offered repeated injection of BTX-A, according to clinical indications, for a maximum of four injections within a period of two years. The minimal interval between injections was six months. The parents were assured that they were not committed to complete the entire course of four injections and could always discontinue the treatment whenever there was a clinical indication for orthopedic surgery or if they felt that the response to treatment was not satisfactory. All the parents provided signed informed consent for their children's participation in the study. The study was approved by the ethics review committee of the Tel Aviv Sourasky Medical Center.
Participants
Children with hemiplegic or diplegic CP who presented with spasticity and dynamic muscle contracture were eligible to be enrolled into the study. The inclusion criteria were age 2–6 years, normal or mildly declined cognition (determined by developmental assessment either by a developmental psychologist or a pediatric-neurologist), and willingness of the family to cooperate in periodic follow-ups. A further requirement was that the patient had good forced passive range-of-motion and good muscle strength of the affected limb (4/5 or 5/5 according to manual muscle testing). Exclusion criteria were fixed joint contractures and/or previous surgery on the lower limbs. The functional level of all patients was assessed and classified according to the growth motor function classification scale (GMFCS) before each injection [16] (Table 1).
Clinical characteristics of the study population
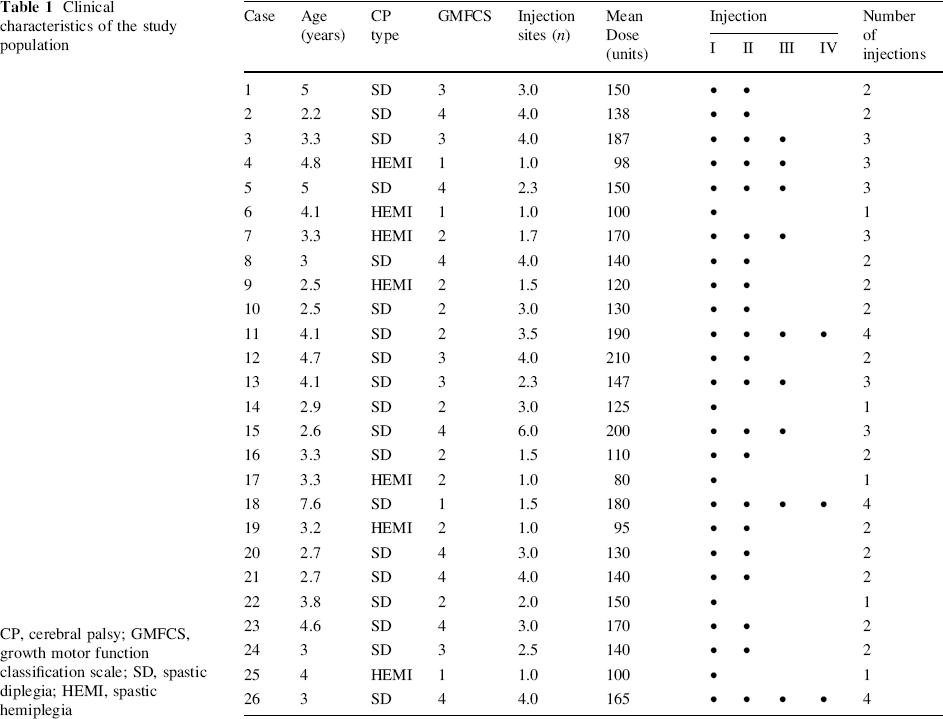
CP, cerebral palsy; GMFCS, growth motor function classification scale; SD, spastic diplegia; HEMI, spastic hemiplegia
Methods of assessment
The study was conducted as an open-label clinical trial. Patients were examined before and after injection by a pediatric neurologist and a pediatric orthopedic surgeon. A thorough medical history was obtained at the first visit. The clinical indications for injection were dynamic spastic equinus or dynamic knee flexion. The injected muscles were the gastrocnemius soleus, the hamstrings, or both. Muscle identification was based on neurological examination and anatomical landmarks. Local anesthesia was achieved by the application of EMLA 5% cream (lidocaine 25 mg and prilocaine 25 mg/g; Astra Pharmaceut Production, Sodertalje, Sweden) to the injection sites 1 h before injection. The injected preparation was BTX-A (BOTOX Allergan, USA) in a final concentration of 5 U/0.1 ml of saline (0.9% sodium chloride solution). Drug administration was carried out according to methodology described elsewhere [9]. The dose for injection was no more than 6 U/kg body weight per muscle of BTX-A and did not exceed a maximum total dose of 12 U/kg body weight. Following the injection, the patient remained in the investigator's office for 15–30 min for close monitoring.
Motor functioning was assessed and scored according to the gross motor function measure-88 (GMFM) [17]. Muscle tone of the injected muscle was assessed by the modified Ashworth scale, and range-of-motion of knee extension (popliteal angle) and ankle dorsiflexion were measured by use of a goniometer. All assessments were carried out by a trained physical therapist prior to each injection and at one-month post-injection. The patients were re-examined four months after each injection to evaluate the need for a repeated injection. The decision on repeated injection, and the timing and site of injection, were based on clinical considerations. Parents were asked to complete a questionnaire and to report whether their child suffered any side-effects, such as systemic fever, local pain or tenderness, irritability, generalized weakness, localized weakness, or sphincter incontinence.
Statistical methods
The studied children were classified according to the number of injections they had received. The groups were compared for age, injected dose (units), and number of muscles injected by the non-parametric Kruskal–Wallis test. The male-to-female ratio, CP type, and GMFCS levels were compared by the Fisher's Exact test. Pearson correlation was used to correlate between the number of injections and the GMFCS levels. The independent t test was used to compare the number of injections of the diplegic and hemiplegic patients.
The pre-injection and post-injection GMFM score, Ashworth scale, popliteal angle, and ankle dorsiflexion were compared by the pairedt test for each injection. The same analysis was used to compare the delta (i.e., the change between pre-injections and post-injections) of the GMFM score, Ashworth scale, popliteal angle, and ankle dorsiflexion, between the first and last injection. This was carried out for each of the 21 children who received more than one injection, whether they had undergone 2–4 injections (“last observation carried forward”).
The paired t test was also used to evaluate the long-term effect by comparing the final (i.e., before the last injection) and baseline scores of the GMFM, Ashworth scale, popliteal angle, and ankle dorsiflexion. The mean rate of GMFM change during the study was calculated as the difference between the last pre-injection score and the baseline score divided by the time (in years) between the two measurements. The mean rate of GMFM change was compared with literature norms of children with CP, standardized for age and GMFCS severity level [18], using the one-sample t test.
The pre-injection scores of the nine patients that received three injections or more were analyzed by ANOVA with repeated measures.
Results
The clinical characteristics of the study population are presented in Table 1. The mean age of the initial group of 26 children was 3.7 ± 1.2 years and the male-to-female ratio was 16:10. Nineteen children had spastic diplegia and seven had spastic hemiplegia. According to the GMFCS, four children were level I, nine were level II, five were level III, and eight were level IV. The mean number of injection sites and the mean total dose injected for the individual patients are displayed in Table 1. The mean total dose of BTX-A was 143 ± 34 units and the mean dose per kg was 9.9 ± 2.5 U. The mean number of injection sites was 2.6 ± 1.2. Most patients (n = 17) were injected in both hamstrings and gastrocnemius soleus muscles, seven in the gastrocnemius soleus alone, and two in the hamstrings alone. The mean interval between injections was 7 ± 3.3 months.
Five children received one injection, twelve received two injections, six received three injections, and three received four injections (Table 1). Overall, 18 children (69%) completed 2–3 injections. The five children who stopped the treatment after the first injection reported having had an unsatisfactory response: two of them had severe calf tightness and underwent orthopedic surgery.
Of the twelve children who discontinued the treatment after two injections, ten underwent an orthopedic surgery within one year, one reported a disappointing response to the second injection and one failed to appear for follow-up (dropout). Six children discontinued the treatment after the third injection; five of them required surgery and one failed to appear for follow-up (dropout). Overall, 17 children underwent orthopedic surgery after at least one injection.
No difference was found between the groups of children classified by number of injections for all measured variables (age, gender, CP type, GMFCS level, and BTX-A dosage). No correlation was found between the number of injections and the GMFCS levels, and no difference in the number of injections of the diplegic and hemiplegic patients.
Four children displayed improvement in their GMFCS level after the first injection: three went from level IV to III and one went from level III to II. Five children achieved a motor milestone during the study. Four of them progressed after the first injection: two from being non-walker to walking-with-aid and two from walking-with-aid to unassisted walking. One child progressed following the second injection from non-walker to walking-with-aid.
Comparison of the mean GMFM score prior to and one-month after each injection revealed a significant increase after the first (P < 0.001, n = 26) and second injections (P < 0.005, n = 21) but not following the third injection. Comparison of the pre-injection and post-injection Ashworth scale showed changes similar to those of the GMFM scores. There was a significant decrease in muscle tone after the first injection (1.7 ± 0.8 pre-injection vs. 1.0 ± 0.7 post-injection, P < 0.001, n = 26) and after the second injection (1.8 ± 0.8 pre-injection vs. 1.4 ± 0.7 post-injection, P < 0.05, n = 21) but not after the third injection. Similarly the extent of the pre-injection and post-injection popliteal angle and ankle dorsiflexion was compared. The decrease in popliteal angle was significant after the first injection (P = 0.001, n = 26) and after the second (P = 0.01, n = 21). The decrease in ankle dorsiflexion was significant only after the first injection (P = 0.005, n = 26).
We compared the effects of the first and last injections for each of the 21 children who received more than one injection. We analyzed the change (delta, Δ) in GMFM score, popliteal angle, ankle dorsiflexion, and Ashworth score (i.e., the differences between the post-injection and pre-injection scores) after the first injection and compared it to the final injection of each child (Table 2). Significant differences were found for the GMFM score, Ashworth score, and popliteal angle, but not for the ankle dorsiflexion (Table 2).
The delta change of clinical parameters for the first injection compared with the last injection (n = 21)
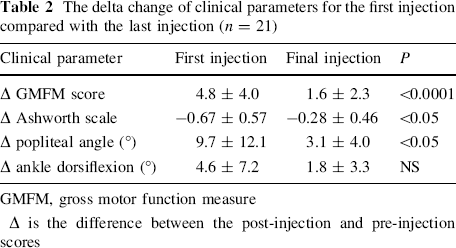
GMFM, gross motor function measure
Δ is the difference between the post-injection and pre-injection scores
The long-term effect of BTX-A injections was evaluated by comparing the baseline score before the first injection with the score before the last injection for each child. A significant difference was found for the GMFM score but not for the Ashworth scores, popliteal angle, or ankle dorsiflexion findings (Table 3). Figure 1 displays the improvement in pre-injection GMFM scores.
Comparison of pre-injection scores at the first and final injections (n = 21)
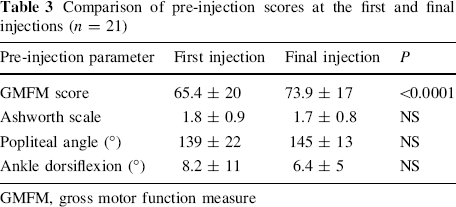
GMFM, gross motor function measure
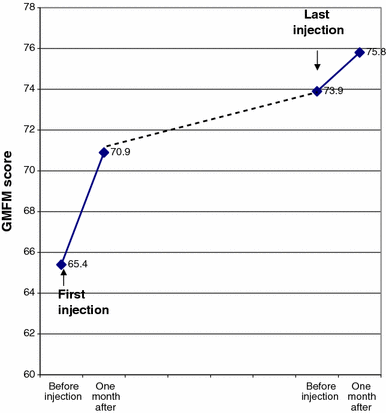
Comparison of mean growth motor function measure (GMFM) scores for the first injection compared with the final injection (n = 21). The mean delta (change between the post-injection and pre-injection score) was significantly greater for the first injection compared with the last (P < 0.001). The mean pre-injection score for the final injection was significantly higher than the pre-injection score for the first injection (P < 0.0001), because of the long-term effect
The mean rate of GMFM change in the 21 children who received more than one injection during the study was 13.2 ± 11.6 per year. We compared the rate of change with literature norms of children with CP according to age and GMFCS severity level (5.37 per year) [18]. The rate of change of our BTX-A treated patients was significantly higher (t = 2.99, df = 20, P < 0.01).
We analyzed the three pre-injection scores of the nine children who received three injections or more and found that there was a time-effect on the pre-injection GMFM scores (F(2,12) = 12.078, P = 0.01), while the changes in their pre-injection Ashworth score, popliteal angle, and ankle dorsiflexion did not reach a level of significance.
Reported side-effects included local pain (n = 2), generalized weakness (n = 2), irritability (n = 1), and transient incontinence that lasted 2 days (n = 1). All side-effects were after the first injection. No child had fever or seizure associated with BTX-A treatment.
Discussion
Injection of botulinum toxin A into the lower limbs of children with CP has been shown to have clinical benefit but there are not enough studies to establish a long-term effect of repeated injections. This prospective study endeavored to investigate this issue by offering repeated injections of BTX-A to a group of ambulatory children with CP. Injections were recommended according to clinical indications for individual children, and not by a rigid injection schedule as reported in other studies [9, 12]. Our results showed that most patients (69%) chose to receive two to three injections. The main reason for withdrawal from the study was secondary unresponsiveness, which could be attributed to late implementation of treatment in relatively older children [19]. This speculation was supported by the fact that most of our patients (17/26, 65%) underwent orthopedic surgery after discontinuing the treatment. As such, the current recommendations are for earlier implementation of treatment with BTX-A [20]. The rate of primary non-response in the present study was 19% (5/26), a figure that is in accordance with the reported rate of 10–40% [12, 21–24]. We attempted to characterize the children who would be most likely to comply with prolonged treatment but did not find any specific predictors for identifying them.
Different methods have been used to evaluate response to intervention. We chose the GMFM score, the Ashworth scale and the range-of-motion as measured by popliteal angle, and ankle dorsiflexion. It emerged that the first injection resulted in the most effective response to treatment and that the effect gradually decreased with each ensuing injection. This could be explained by antibody formation that was demonstrated in a recent study: high antibody titers were found in 35 of 110 (31.8%) patients with >2 BTX-A injections and they correlated with secondary nonresponse [25].
The main finding of our study was the long-term effect of BTX-A. We demonstrated that children had a higher GMFM score before the final injection compared with the score before receiving the first injection although their muscle tone, as measured by the Ashworth scale, was the same. It is well known that the effect of BTX-A is temporary and that the muscle tone resumes its previous level after a few months. The results of our study, however, show that motor function, as measured by GMFM scores, does not returns to its original level but that some improvement persists for at least 19 months. Furthermore, the rate of GMFM change was significantly higher than expected from figures published in the literature [18] and thus cannot be attributed to “normal” motor development. This finding suggests that BTX-A treatment has a long-term effect on motor function even though the effect on muscle tone had disappeared. Similar evidence of improved motor function over time emerged when we compared the pre-injection GMFM scores of the first three injections (n = 9).
The limitations of the study are the diverse number of injections in the study group due to individualized clinical considerations. As a result we used the method of comparing the last observation carried forward. Consequently, the studied group was small (n = 21) and the follow-up period was not equal for all children. Nevertheless, our results demonstrated significant improvement in motor function, regardless of the number of injections, in CP children treated by BTX-A injections compared with the untreated ones.
In conclusion, the results of this study indicate that BTX-A has a long-term effect on gross motor function in children with CP, even though the effect on muscle tone is short-term. The short-term effect seems to decline with repeated injections, with most children benefitting from two or three injections.
Footnotes
Acknowledgments
We thank Esther Eshkol for her editorial assistance, and the children and their parents for their time and goodwill. This study was supported by an educational grant from Allergan Inc. UK.