
Abstract
Abstract
Introduction/background
Russell–Silver syndrome (RSS) is the combination of intrauterine growth retardation, difficulty feeding, and postnatal growth retardation. Leg length discrepancy (LLD) is one of four major diagnostic criteria of RSS and is present in most cases. We aimed to ascertain whether pediatric RSS patients will adequately consolidate bony regenerate following leg lengthening.
Materials and methods
We retrospectively reviewed pediatric RSS patients who underwent limb lengthening and compared them to a similar group of patients with LLD resulting from tumor, trauma, or congenital etiology. The primary outcome measurement was the bone healing index (BHI).
Results
The RSS group included seven lengthened segments in five patients; the comparison group included 21 segments in 19 patients. The groups had similar lengthening amounts (3.3 vs. 3.9 cm, p = 0.507). The RSS group healed significantly faster (lower BHI) than the control group (BHI 29 vs. 43 days/cm, p = 0.028). Secondary analysis showed no difference between RSS and trauma patients in terms of the BHI (29 vs. 31); however, the BHI of the RSS group was significantly lower than both of the other congenital etiologies (29 vs. 41, p = 0.032) and tumor patients (29 vs. 66, p = 0.019). The RSS patients had fewer and less significant complications than the controls.
Discussion
The limb lengthening regenerate healing of RSS patients is faster than the healing of patients with other congenital etiologies and tumor patients, and is as fast as the regenerate healing of patients with posttraumatic LLD. Although all RSS patients were treated with human growth hormone (hGH), we are unable to isolate the hGH contribution to the regenerate bone healing. We conclude that RSS patients can have safe limb lengthening.
Introduction
Russell–Silver syndrome (RSS) is a genetically heterogeneous condition characterized by short stature, small size for gestational age, variations in sexual development, and asymmetry [1]. Patients typically present with intrauterine growth retardation, difficulty feeding, failure to thrive, or postnatal growth retardation [2]. Catch-up growth is often inadequate, resulting in abnormally short stature in adulthood (≤−3.6 standard deviations [SD]) [3, 4]. More than 400 cases have been reported and estimates of incidence range from 1 case in 3,000 to 1 case in 100,000 [5]. Leg length discrepancy (LLD) is one of the most common orthopedic presentations and is found in more than 90 % of patients with RSS [1]. The average LLD reported in RSS patients is 3.1 cm, with a persistent percentage of inhibition throughout growth, leading to larger absolute LLDs at maturity [1, 4].
Also, abnormalities of spontaneous growth hormone (GH) secretion and subnormal responses to GH stimulation testing have been reported in many children with RSS [6, 7]. Many RSS children are treated with human growth hormone (hGH) to treat abnormally short stature. Increased linear growth without concomitant increase in limb length discrepancy was reported in the setting of RSS patients [8–11]. Various conditions have been indicated for hGH treatment, including congenital short stature, Turner syndrome, Prader–Willi syndrome, Noonan syndrome, chronic renal failure, congenital adrenal hyperplasia, idiopathic small stature, and small for gestational age complex [12–19]. While hGH therapy increases the total limb length, it does not appear to induce limb-specific catch-up growth or reduce the discrepancy between limbs.
Given the frequency and severity of the LLD associated with RSS, many patients will present for limb equalization surgery; however, their condition limits the therapeutic options. Contralateral epiphysiodesis around the knee further reduces adult height and, as such, is a suboptimal surgical option for these patients. There are reports of limb lengthening of RSS children [1], but no specific data on regenerate consolidation are given. In principle, both the failure to thrive and dietary difficulties [2, 20] inherent in RSS raise concerns about these patients’ healing potential.
In order to clarify the potential for the safe limb lengthening in RSS patients, we conducted a retrospective case-matched comparison of RSS patients to a general pediatric lengthening control group.
Methods
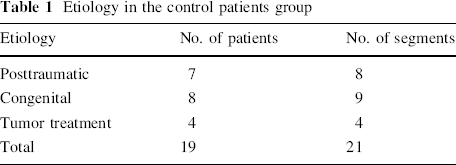
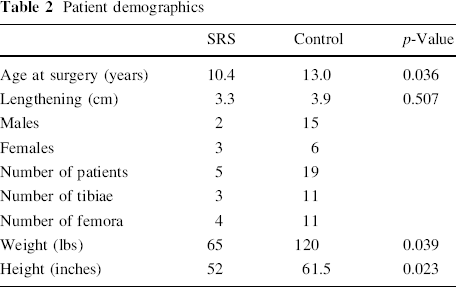
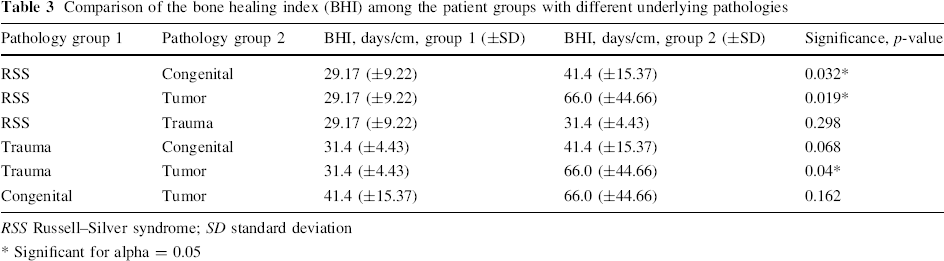
The current study was designed as an institutional review board (IRB)-approved retrospective comparison of pediatric patients with RSS who underwent limb lengthening for LLD equalization as compared to similar surgery for other indications in a general pediatric lengthening population. Seven limb segments (either the femur or the tibia) in five patients with RSS were treated between 2000 and 2010 (Fig. 1). All of these patients were being treated with hGH prior to and at the time of surgery and during the lengthening period under the supervision of the referring pediatric endocrinologist.
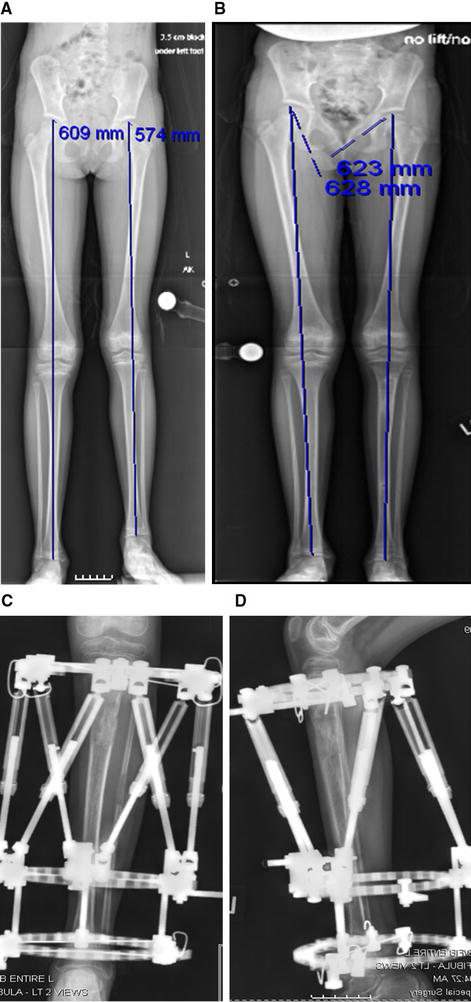
Illustrative case of an 8-year-old patient with Russell–Silver syndrome (RSS).
Control group patients were selected from the limb lengthening service IRB-approved database based on their age at surgery and the amount of lengthening, in an attempt to match the RSS patients. The control group etiologies were heterogeneous and included congenital shortening, posttraumatic growth arrest, and growth inhibition/arrest following tumor surgery (Table 1).
Etiology in the control patients group
Skeletal dysplasia patients and patients who underwent simultaneous bilateral lengthening or a combination of lengthening with nailing/plating were excluded from the control group. A total of 21 limb segments in 19 patients were identified for inclusion into the control group.
All patients in both groups underwent surgery by the senior author (S.R.R.). The Ilizarov–Taylor Spatial Frame (Smith & Nephew, Inc., Memphis, TN) or monolateral rail frames (EBI/Biomet, Parsippany, NJ) were used to stabilize and distract the bone following osteotomy in the tibia and femur, respectively [21, 22].
Although the RSS patients were 2.5 years younger than the average control patient (p = 0.027), the amount of lengthening per segment was equivalent (p = 0.507) (Table 2). We calculated the predicted LLD at maturity by using the multiplier method [23]. The treatment plan was either one or two lengthening treatments, depending on the LLD and age at presentation, and predicted LLD. We prefer to do lengthening of less than 20 % of the bone segment length.
Patient demographics
The bone healing index (BHI) was the primary outcome. The BHI was defined as the number of days between osteotomy and bony union, divided by the amount of lengthening in centimeters. The bone healing date was decided by a surgeon who was not involved in the patients’ treatment. Bones were considered to be healed once radiographic continuity of three of four cortices was demonstrated.
Adverse events were recorded and analyzed. Finally, the use of ultrasound or electrical bone stimulators was collected for each subject. The length of follow up for the RSS group was 32 ± 8.2 months (range: 16–38) and for the control group, it was 58 ± 35.8 months (range: 12–130).
All statistical analysis was performed using PASW 18.0 (SPSS, Inc., Chicago, IL). An alpha level of 0.05 was set. Nonparametric tests were selected because the sample size was too small to reliability assume normalcy. Independent samples Mann–Whitney U-tests were used to compare all continuous variables between the RSS group and the whole control group. When the control group was split into etiological subgroups (trauma, tumor, congenital), the initial analysis was done using Kruskal–Wallis tests. Significant models were followed up with Mann–Whitney U-tests to determine which subgroups differed.
Results
RSS patients had a mean BHI of 29 days/cm, and the control group had a significantly longer BHI of 43 days/cm (p = 0.028). Kruskal–Wallis analysis of the BHI by etiological subgroups within the control group revealed significant differences in the BHI (p = 0.014): congenital 41.4 days/cm, trauma 31 days/cm, tumor 66 days/cm. Post-hoc analysis demonstrated equivalency of the RSS group and trauma control subgroup BHIs (p = 0.298). However, there was a significantly lower BHI in the RSS as compared to both the tumor (p = 0.019) and congenital (p = 0.032) control subgroups. Within the control group, the trauma subgroup had significantly shorter BHI than the tumor subgroup (p = 0.04) (Table 3).
Comparison of the bone healing index (BHI) among the patient groups with different underlying pathologies
RSS Russell–Silver syndrome; SD standard deviation
Significant for alpha = 0.05
The amount of lengthening was not homogeneously distributed across the control subgroups (p = 0.011) (Table 4): trauma patients (5.06 cm) had significantly larger lengthening than patients with congenital etiologies (2.98 cm, p = 0.02).
Comparison of the amount of lengthening among the patient groups with different underlying pathologies within the control group
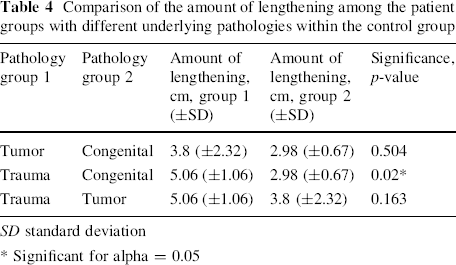
SD standard deviation
Significant for alpha = 0.05
All RSS patients used an electrical bone stimulator (Biomet, Parsippany, NJ) during lengthening and consolidation. Seven of the 19 control group patients used electrical (Biomet, Parsippany, NJ) bone stimulators and three used ultrasonic bone stimulators (Exogen, Smith & Nephew, Inc., Memphis, TN). One control patient had bone marrow aspirate concentrate injected into the regenerate bone to stimulate healing. The analysis within the control group demonstrated no difference between those treated with bone stimulator and those who were not (43 vs. 44 days/cm).
Five RSS patents had temporary ankle or knee stiffness, which resolved with Dynasplint (Dynasplint Systems, Severna Park, MD) and physical therapy; one patient had superficial pin site infection, which resolved with 10 days of oral antibiotics.
Eleven control patients had problems with temporary stiffness that resolved with dynamic splinting and physical therapy or pin site infection that resolved with oral antibiotics. Six patients had knee or ankle joint stiffness that was treated with the surgical release of quadriceps, iliotibial band, hamstrings, or gastrocnemius. One control patient had osteomyelitis treated with incision and drainage in the operating room and intravenous antibiotics. Residual deformities were accepted in two patients (one had mechanical axis deviation 39 mm laterally and the second had 17 mm medially).
Discussion
Russell–Silver syndrome is a rare condition with multiple comorbid orthopedic problems, notably including function-limiting LLDs. As a result, many RSS patients seek limb length equalization procedures; however, the nature of their underlying condition presents a therapeutic dilemma. RSS patients typically have difficulty feeding and, thus, poor nutritional status, to the point of requiring nasogastric or percutaneous enteral feeding [2, 12]. These issues raise concerns about the timeliness and adequacy of regenerate formation and consolidation following distraction osteogenesis in RSS patients. This dilemma is compounded by the extreme paucity of RSS lengthening reported in the literature [1].
In this series, all five RSS patients had good outcomes, with minimal incidence of adverse events. Each of the patients achieved the preoperative limb lengthening goal; neither persistent deformities nor permanent joint stiffness occurred. None of the patients treated with hGH experienced premature consolidation. The only problems observed were temporary knee or ankle stiffness and pin tract infection, which resolved with physical therapy and dynamic splinting or oral antibiotics. Importantly, although hGH treatment has known potential complications such as carpal tunnel syndrome, Legg–Calvé–Perthes disease, slipped capital femoral epiphysis, and scoliosis [24–30], none of these complications were seen in this series.
The prediction of final LLD using conventional methods may be challenging, since all the patients in our series were treated with medication to delay puberty. We think that the predicted LLD at maturity will ultimately be greater than the calculation of the multiplier method [23], since growth will continue beyond the usual endpoints related to drug-induced delay of puberty.
Although the RSS group had no complications, the sample size and design of the study are not adequate to say that the RSS and control groups actually have different rates of adverse events; however, the rate of adverse events across groups was comparable to those previously published. Eidelman et al. reported a 45 % rate of superficial tract infections in 31 children and adolescents, and one residual deformity following correction. Obstacles in that study included three regenerate fractures, transient peroneal palsy, and injury to the genicular artery [31]. Marangoz et al. [32] reported 20 patients; problems they encountered included six pin tract infections four stiff knees, and one new subluxation treated nonoperatively; obstacles included two delayed unions requiring grafting and one knee subluxation requiring release and frame extension.
While the RSS and control group patients had equivalent lengthening (3.3 [2.5–4.2] cm vs. 3.9 [2.5–7.5] cm, p = 0.507), the RSS group's BHI was significantly lower than the control group's BHI (29 vs. 43 days/cm, p = 0.028), suggesting faster healing. The trauma subgroup had a larger amount of lengthening as compared to the RSS group, which may also account for the lower BHI. Limb lengthening in RSS patients with hGH treatment shows lower BHI than in patients with congenital or tumor-associated LLD, but the same BHI as in normal bone (posttraumatic patients) and there were no adverse events.
The variable use of bone stimulators is a potentially confounding variable. However, all patients did use adjuvant bone stimulation. The inconsistent use of the type of bone stimulators reflects the evolving standard of care on our service and is a function of when patients were treated, rather than a feature of the particular cases. No BHI difference was seen within the control group with regard to bone stimulators use.
Other limitations of this study include the younger age of RSS patients (10.4 vs. 13.0 years p = 0.036) and retrospective design without etiologically matched controls. With respect to age, both ages fall within the same distraction–consolidation group as described by Fischgrund [33]. Although prospective randomization would clearly be preferable, the scarcity of patients and the widely accepted benefits of hGH treatment in RSS children for congenital short stature patients makes such a study practically challenging and difficult from an ethical perspective.
Although it would be ideal to compare limb lengthening in RSS patients with and without hGH treatment, this was not possible. The referring pediatric endocrinologist had an established treatment protocol with hGH. The literature search did not reveal any reports regarding the BHI of RSS patients treated with or without hGH.
Etiological subgroup analysis within the control group demonstrated that patients who had lengthening following tumor resection had the longest BHI (66 days/cm). This was significantly longer than the BHI of RSS (66 vs. 29 days/cm, p = 0.019) and posttraumatic (66 vs. 31 days/cm, p = 0.04) patients. Tumor and congenital reconstruction BHIs were equivalent (66 vs. 41 days/cm, p = 0.162). Finally, the posttraumatic subgroup required larger lengthening than the congenital etiologic subgroup (5.06 vs. 2.98 cm, p = 0.02), and they trended toward shorter BHIs than the congenital patients (31.4 vs. 41.4 days/cm p = 0.068). This may reflect the longer absolute lengthenings in the trauma group. However, our findings also mirror Catagni et al.'s previously published congenital lengthening BHI (44.9 days/cm) [34] and Maffulli et al.'s finding that lengthening for congenital etiology healing is slower than that for posttraumatic etiology [35]. The similarity of these previously published results to our control population lends added interest to the apparently faster healing in RSS patients (29 vs. 43 days/cm, p = 0.028). The lack of data reporting on RSS patients not treated with hGH does not allow us to conclude about the influence of hGH on bone healing in that group of patients.
In conclusion, despite the small number of patients, retrospective design, and confounders inherent therein, we believe that RSS patients demonstrated uniformly good healing of bone regenerate following Ilizarov lengthening by distraction osteogenesis. Additionally, it is noted that their bone healing may even be faster than other congenital and tumor pediatric lengthening patients. The role of hGH in regenerate bone healing remains unclear and a randomized control trial would potentially clarify this issue.
Footnotes
None.
Acknowledgments
We would like to thank Dr. Stephen Lyman for his assistance with the statistical issues in this study. This study was not financially supported by any source.