
Abstract
Abstract
Purpose
To bring to the attention of the orthopaedic fraternity that adolescent children smoke and this has an adverse effect on the bone regenerate during limb deformity corrective surgery.
Methods
Retrospective review of patients undergoing limb deformity corrective surgery with a prolonged frame time and bone-healing index. Patients operated on between 1993 and 2005 in a single regional specialist paediatric orthopaedic hospital.
Results
Seventeen smoking patients (16 adolescent, one aged 9 years), with prolonged bone regenerate consolidation time of more than double the standard time. Bone-healing index (BHI) was increased in both active smokers and passive smokers.
Conclusions
In the older child/adolescent we should consider smoking (active or passive) as a detrimental factor in prolonging their frame times. We should council these patients and their carers to stop smoking at least during the period of their treatment.
Introduction
A recent Department of Health white paper revealed there are currently 13 million smokers in the UK [1]. This despite the campaigns to reduce and stop smoking. A report on teenage smoking attitudes found that most smokers in England start smoking soon after secondary school education [2]. A recent survey in Nottinghamshire found that 17% of pupils in school years 7–11 (age 11–16) were current smokers [3].
During routine follow up of adolescent patients (11–19 years), undergoing limb reconstructive surgery, it was noted that the time taken for the formation of regenerate was prolonged in a subgroup of patients who were found to be smokers. Closer examination of all patients undergoing limb deformity corrective surgery was then performed, looking in particular at the smokers for the quality of the bone regenerate and the time to consolidation.
Materials and methods
A retrospective review was carried out to identify patients who were found to have a prolonged time to consolidation following limb reconstructive surgery during their post-operative assessment. These patients had their reconstructive procedures performed between 1993 and 2005.
Each of these patients was interviewed about their smoking habits and their carers’ smoking habits. Their notes were reviewed to calculate the time taken for the removal of the external fixator frames in days and the total length of regenerate gained in centimetres. Serial check radiographs were examined and measured for length gained and consolidation by a single observer (RR). Bone-healing index was calculated using the number of days from the time of application of the fixator to its removal divided by the total number of centimetres gained.
Results
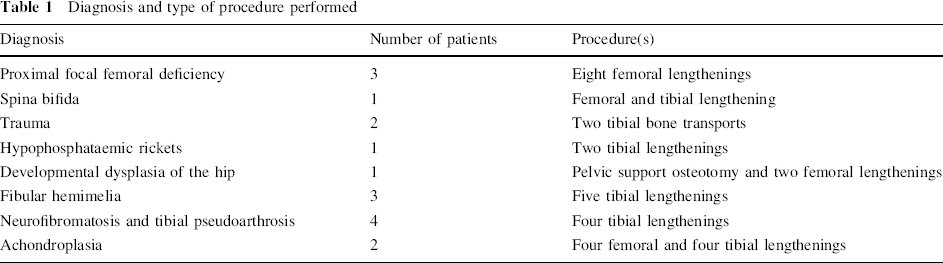
Seventeen patients, 16 adolescents, one aged 9, were identified as having much longer than expected frame times with prolonged BHI. The objective criterion used for a prolonged BHI was in excess of 60 days cm−1. These 17 patients (7 female, 10 male) underwent a total of 33 operations. Their average age was 14.5 years (9–18). The diagnosis and type of procedure performed was documented (Table 1).
Diagnosis and type of procedure performed
Twelve of the 17 patients identified to have increased BHI admitted to being active smokers. In addition, two of this group of active smokers had parents who were also active smokers. The remaining five patients denied smoking but had carers who were active smokers.
In the active smokers group (12 patients), 16 operations were performed and the average BHI was 77.5 days cm−1. In the non smokers group (five patients), a total of 17 operations were performed with an average BHI of 68.5 days cm−1. Although there is a marked difference in the BHI between these two groups, the difference is not statistically significant since both groups of patients were pre-selected because they were found to have a much prolonged BHI in the first place.
Discussion
The BHI for limb-lengthening procedures in lower limbs for children with osteogenesis imperfecta has been found to be 33.25 days cm−1 [4], in tibial pseudoarthrosis 37 days cm−1 [5], in achondroplasia 33.6 days cm−1 [6], and in fibular hemimelia 54.3 days cm−1 [7]. Both our groups of 17 patients demonstrated a much higher BHI than these averages.
We were perplexed to find that the second group (non-smokers with carers who were active smokers) still demonstrated this doubling of BHI. However, on closer investigation, we found that their carers smoked in the presence of these children both at home and within the confined space of the car. All these five children lived a considerable distance from Sheffield and were driven to Sheffield for their follow ups in a smoke-filled car as their carers smoked both on the way to and from regular follow ups. Clearly their increased BHI demonstrated the effects of passive smoking.
Various animal-model studies [8, 9] have demonstrated adverse effects of nicotine on cytokines associated with neovascularisation and osteoblast differentiation, and nicotine also delays bone mineralization. Authors of in-vitro culture studies of osteoblast-like cells exposed to cigarette smoke speculated that nicotine had a stimulating effect on bone cell metabolic activity, but the delay in healing was attributed to the absorption of other components of cigarette smoke other than nicotine [10].
In trauma with open tibial fractures, an increased time to union and complications in smokers was demonstrated [11]. Closed tibial fractures of smokers when compared to non smokers took 62% longer to heal [12].
As far as we are aware there are no studies which demonstrate how long a time period is required for full reversal of the detrimental effects of smoking on the skeletal system. Also, to the best of our knowledge, there are no studies looking at the reversal effects of cessation of smoking in children. We do not know whether, following the cessation of smoking, the reversal of its detrimental effects could possibly be age related.
Our group of patients were pre-selected due to their prolonged BHI. We cannot possibly make any comment about the possibility that some children might have had a normal BHI despite being either active or passive smokers.
Although this is a retrospective review study, we feel that the message from this study is worth stressing. The orthopaedic fraternity needs to be aware that smoking does occur in the adolescent group. We also need to be aware that the effects of both active and passive smoking are detrimental to the adolescent group undergoing limb reconstructive surgery, prolonging the frame time. This in turn increases the chances of pin site infection, frame failure, and has psychosocial effects too.
We have designed a pamphlet in The Sheffield Childrens’ Hospital to make both the patient and their carers aware of the effects of active and passive smoking. We feel that it would not be possible to conduct a prospective randomised controlled trial in this case to demonstrate the detrimental effects of smoking but that the results of this retrospective review speak volumes.