
Abstract
Abstract
Purpose
Waterproof casts have been shown to provide adequate support and immobilization in fractures. This study evaluated two waterproof cast liners, namely, Wet or Dry® and Delta Dry®, in terms of ease of application/removal, durability, longevity, and patient satisfaction using patient- and technician-reported outcome measures.
Methods
A total of 105 children were enrolled in a randomized trial and received a below-elbow synthetic cast with either of the two cast liners.
Results
The two groups were comparable with regards to age, gender, side of cast, and hand dominance. Assessment was carried out at application and removal. In the patient-reported outcomes, the Wet or Dry® group was rated significantly better in the odor and water resistance categories. In the technician-reported application and removal outcome measures, the Delta Dry® group was rated significantly higher.
Conclusions
The use of waterproof cast liners appears to be safe in children with forearm fractures, with some differences in outcome between the two products trialed.
Introduction
Forearm fractures commonly occur amongst the paediatric population, with cast immobilization being the mainstay of management. In a Swedish urban population, the accumulated risk of a fracture during childhood was 27 % in girls and 42 % in boys [1]. Approximately 2,800 casts are applied annually in the outpatient department at our hospital, and ways to improve the service in terms of material cost, staff time, and user-friendliness are important. Traditional casting techniques employ plaster of Paris with cotton undercast padding; however, they impose significant limitations by demanding no water exposure. This is particularly relevant in the warm Australian climate.
The advent of modern water-resistant casting materials has revolutionized the management and behavior of paediatric patients. Synthetic casts in combination with water-resistant undercast padding allows unrestricted water exposure without compromise of integument or fracture healing [2–5]. Numerous water-resistant undercast padding products are currently available (Delta Dry®, Wet or Dry®, Gore®, Procel®, Water Pruf®, Infina Under-Cast®, and Nemoa® Cast); however, no comparison of qualitative or quantitative performance has been evaluated.
The aim of this study was to compare the technical, clinical, and functional outcomes between two water=resistant undercast padding materials, Wet or Dry® and Delta Dry®, in the treatment of paediatric forearm fractures. Clinical assessment and both patient- and technician-reported outcome measures were utilized.
Patients and methods
Trial design
A randomized trial comparing two water-resistant undercast padding materials, Wet or Dry® and Delta Dry®, was conducted between May 2010 and June 2011. The study was approved by the Institutional Review Board of our hospital.
Participants
Children under the age of 18 years with newly diagnosed, minimally displaced traumatic distal radius fractures requiring below-elbow cast immobilization were enrolled in the study. The study was undertaken in the Fracture Clinic of an urban tertiary referral center in Australia, where an average of 2,800 casts are applied annually. Children with open injuries were excluded.
Recruitment
Patients were recruited between May 2010 and June 2011, and ceased once the stipulated sample size was achieved.
Sample size
A sample size of convenience was taken, with a total of 105 patients.
Randomization
Sequence generation
Two hundred allotments with equal numbers of both interventions were made and placed in unmarked envelopes in a cardboard box in a random sequence.
Allocation concealment mechanism
Opaque envelopes were used, each containing a form indicating either Wet or Dry® or Delta Dry®.
Implementation
After consent and recruitment, the plaster technician randomly picked an envelope from the box and the listed intervention was assigned. During the course of the study, an interim analysis after 100 allotments was planned, but was carried out when 105 patients were recruited. The numbers at that point were found to be adequate to show a difference between the interventions and, thus, the trial was stopped.
Interventions
The interventions were the use of either Wet or Dry® or Delta Dry®) (Fig. 1) as the water-resistant undercast padding of a synthetic below-elbow cast (3M Scotchcast™ Plus, St. Paul, MN, USA). Children with forearm fractures were referred to the fracture clinic after the application of an initial above-elbow slab in the Emergency Department. Those requiring below-elbow casts who were included in the trial were then randomly allotted to either of the two liner groups. A single senior cast technician applied all casts. Patients and their parents were provided with written instructions advising and encouraging water exposure.
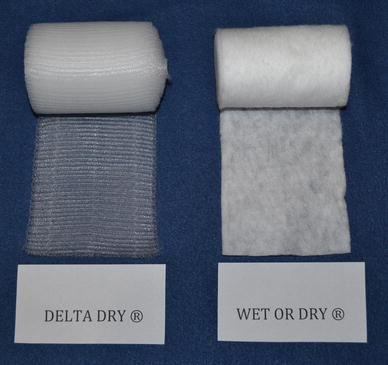
Photograph of Wet or Dry® (polypropylene/polyethylene knit and non-woven fiber) and Delta Dry® (polypropylene, polyamide, polyester, and acrylic adhesive) undercast padding
Outcomes
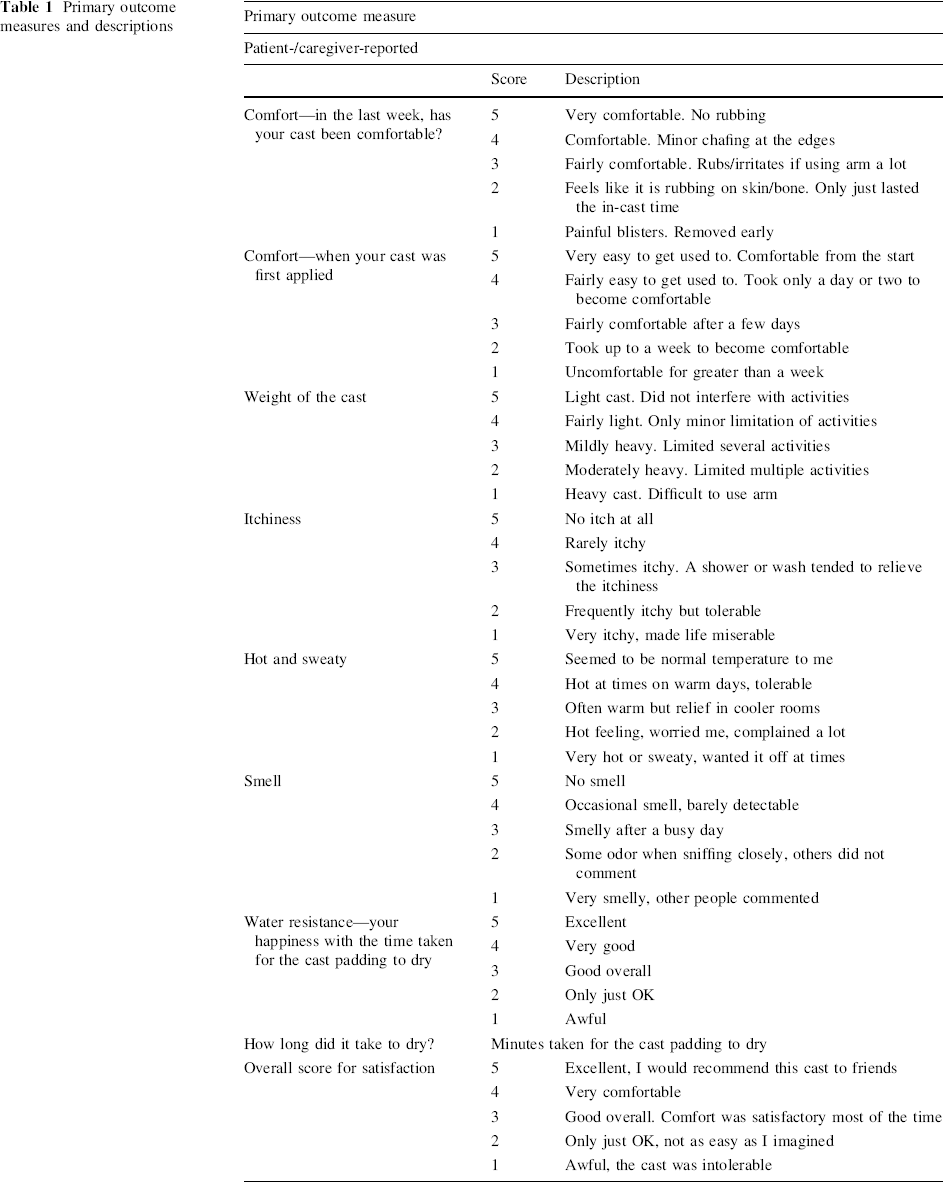
The primary outcome measure was the patient's/caregiver's qualitative assessment of the undercast padding material at removal. Patient-reported outcomes pertaining to physical perception and personal satisfaction were executed through the completion of a questionnaire (Table 1).
Primary outcome measures and descriptions
The secondary outcome measure was the plaster technician's qualitative assessment of the undercast padding material at application and removal. This was executed through the completion of a questionnaire (Table 2).
Secondary outcome measures and descriptions

All qualitative questionnaire components were scored on a 3- or 5-point scale. Temporal measures of application and drying duration were quantified in minutes. Due to the lack of validated scoring systems, the above-mentioned questionnaires were devised considering the relevant outcomes.
Blinding
Following cast removal by a clinical nurse, an assessment of skin condition was completed by the cast technician. The cast technician assessing the skin condition was, thus, blinded to the type of liner; however, the authors are aware that the pattern of liner on the skin may have indicated the type of padding used, thus, inducing some observer bias. The person who removed the cast recorded the ease of removal, padding durability, and longevity factors.
Statistical methods
Fisher's exact test and ordinal logistic regression analyses were used to compare the ordinal level ratings of the two liner groups. The Wilcoxon rank-sum test was used to compare continuous (ratio level) data that were significantly skewed.
All the analyses were performed using Stata Intercooled 12.1 for Windows.
Results
Participant flow
A total of 105 patients were recruited, with 51 and 54 patients in the Wet or Dry® and Delta Dry® cohorts, respectively, all receiving the assigned intervention. No participants were lost to follow up. With regards to the time taken to dry (a primary outcome measure from the patient-/caregiver-reported questionnaire), two patients were excluded from the Wet or Dry® group, as one failed to expose the cast to water, whilst the other did not quantify the duration of exposure, and four patients were excluded from the Delta Dry® group, all failing to quantify the duration of water exposure.
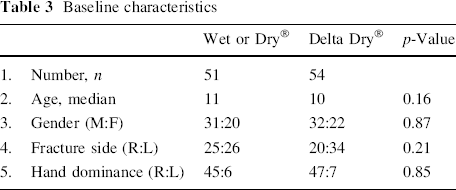
Baseline data
The mean age of the entire cohort was 9.98 years [standard deviation (SD) 3.11] and the male:female ratio was 3:2. The two groups were comparable with regards to age, gender, side of cast, and hand dominance. The baseline data are recorded in Table 3.
Baseline characteristics
Numbers analyzed
In both groups, except for the outcome of “time taken to dry”, the number of patients with complete data (denominator) was the same as the number of patients recruited. For the “time taken to dry”, the total number of patients with complete data was 49 in the Wet or Dry® group and 50 in the Delta Dry® group.
Outcomes and estimation
Primary outcome measures
Patient/caregiver report
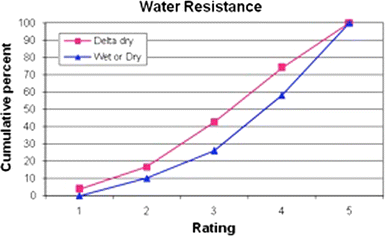
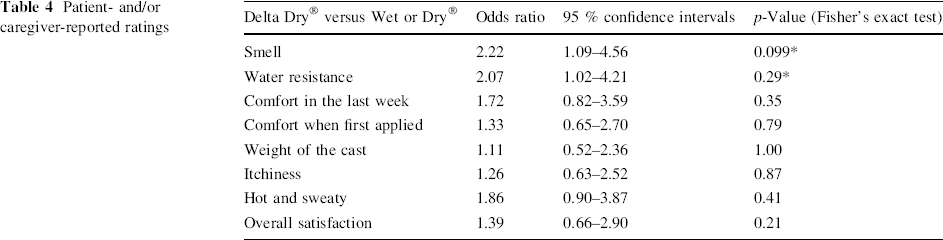
For the categories “smell” and “water resistance”, the Wet or Dry® group rated significantly higher (as per the ordinal logistic regression analyses) than the Delta Dry® group (Figs. 2 and 3). However, there was no statistically significant difference in the ratings for the categories ‘Comfort in the last week’, ‘Comfort when cast first applied’, ‘Weight of the cast’, ‘Itchiness’, ‘Hot and Sweaty’, and for ‘Overall satisfaction’ (Table 4). The difference in the ‘time to dry’ was not statistically significant between the two groups; however, there was an indication of less time to dry for the Wet or Dry® group compared to the Delta Dry® group (p = 0.069). The median time to dry was 30 and 60 min for the Wet or Dry® and Delta Dry® groups, respectively.
Cumulative percentage of “smell” in the Wet or Dry® and Delta Dry® groups Cumulative percentage of “water resistance” in the Wet or Dry® and Delta Dry® groups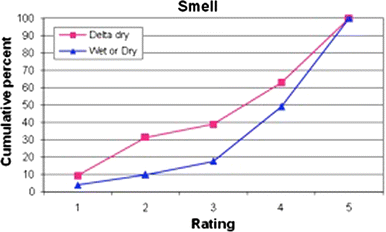
Patient- and/or caregiver-reported ratings
Ancillary analysis
Considering the possibility that a fracture in the dominant extremity could affect the subjective functional outcomes, an ordinal logistic regression for predicting overall satisfaction was completed. A negligible influence upon the odds ratio was revealed after adjusting for a fracture in the dominant side [unadjusted odds ratio: 1.387, 95 % confidence interval (CI) 0.665–2.895 and adjusted odds ratio: 1.388, 95 % CI 0.665–2.897].
Adverse events
No major adverse events were noted.
Secondary outcome measures
Technician-reported ratings at application
In all the categories reported at application, the Delta Dry® group achieved a significantly higher rating compared to the Wet or Dry® group: ease of application (p < 0.001), moldability (p = 0.011), durability (p = 0.001), and padding level (p < 0.001) (Table 5).
Technician-reported ratings at application

Estimation of an odds ratio was not possible because of zero values in the end categories
Technician-reported ratings at removal
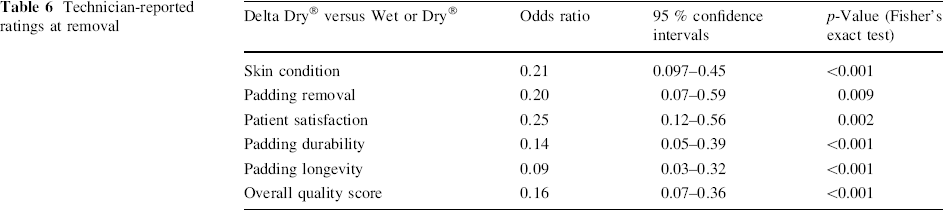
In all the categories reported at removal, ratings for the Delta Dry® group were significantly higher compared to those of the Wet or Dry® group: skin condition (p < 0.001), padding removal (p = 0.009), patient satisfaction (p = 0.002), padding durability (p < 0.001), padding longevity (p < 0.001), and overall quality score (p < 0.001) (Table 6). No significant association could be demonstrated between the type of liner used and whether there was evidence of poking objects down the cast (p = 0.21).
Technician-reported ratings at removal
Discussion
This study investigated the technical, clinical, and functional outcomes between two water-resistant undercast padding materials, Wet or Dry® and Delta Dry®, in the treatment of paediatric forearm fractures.
With respect to the patient's and caregiver's qualitative assessment of the undercast padding material at removal (primary outcome measure), both groups were equally satisfied. Although the Wet or Dry® group achieved marginally superior smell and water resistance appraisal, no statistically significant difference amongst the remaining patient-reported domains and overall satisfaction was demonstrated.
The comparable performance of the two materials is not surprising when the exposure and demands placed upon the materials are considered. The combination of a synthetic cast with a water-resistant undercast padding liberates the immobilization construct to water exposure, with high physician and patient satisfaction in the past [6]. This property is valued in the paediatric population, in whom both hygiene and recreational activities are made significantly easier. Such a tolerance for moisture is important in the Australian climate, plagued by high temperatures and humidity in the summer. Despite written and verbal instructions encouraging full water exposure, the majority of casts were only wet in supervised and restricted showering environments. The parental perception and historical association of “keeping casts dry at all costs” proved to be a difficult belief to challenge. A number of children tested their casts to full immersion, either in the bath or chlorinated swimming pools. No cast was exposed to an ocean water environment. This challenge was both safe, with no skin compromise, and positively evaluated by the supervising parents, who noted that social inclusion in activities and continuation of swimming classes was invaluable.
The limitation of demand upon the cast was compounded by the relatively cylindrical structure of the forearm cast. Without an angular challenge of the material (i.e., above-elbow cast), the imposition of creases upon skin and impeded water drainage was not evaluated.
Cast immobilization is applied in many facets of paediatric orthopaedics. The safety and satisfaction parameters of this study may be extrapolated for other indications. The hygiene demands of hip spicas may be augmented with the use of water-resistant undercast padding. Wolff and James have shown benefits of a Gore-Tex waterproof cast liner in children with hip spicas [7]. Safe partial and complete immersion may be exploited to optimize cleaning and recreation activates under parental supervision.
Interestingly, the two cast liners differ in their chemical composition. Wet or Dry® contains a polypropylene/polyethylene knit and non-woven fiber, whilst Delta Dry® contains a polypropylene, polyamide (nylon), polyester, and acrylic adhesive. The nylon and adhesive component of the Delta Dry® imparts a marked tactile difference. This was not reflected clinically, as both itching and comfort measures were similar. The nylon weave of the Delta Dry® padding also provides a relative resistance to shear stress. This is advantageous in patients prone to “picking” the liner from their cast, especially in hip spicas. This characteristic may, however, impose a barrier to removal if used in patients from remote regions with limited health care access. Such patients’ form may be managed with a cotton undercast padding and plaster of Paris cast, eliminating the necessity of a plaster saw for removal.
With respect to the plaster technician's qualitative assessment of the undercast padding material at application and removal (secondary outcome measure), the results demonstrated a preference for the Delta Dry® group at both application and removal. Notably, the assessment of technical handling and physical characteristics of the Delta Dry® material were improved.
With up to 40 % of children sustaining a fracture by the age of 16 years [1], the population volume demand upon casting materials and the technician is high. A rationalized casting construct must, therefore, be physically sound, clinically acceptable, and technically compliant. Modern emphasis on the efficient use of health funding suggests that improving service delivery through refining material cost as well as user-friendliness is important. In the absence of clinical and patient-reported differences, the choice between materials may rest upon fiscal markers and technician preference.
The advantages of this study are the methodology used and the adequate sample size that allows the detection of statistically and clinically significant differences in the primary outcome measures. The methodology provides a suitable template for an evidence-based approach to evaluating casting materials and other interventions in institutions considering modifications to their casting protocols. The limitations of this study are the lack of a validated scoring system, which necessitated the use of subjective scores. The simple randomization technique may be questioned; however, the lack of a significant difference in the relevant baseline characteristics of the groups indicates adequate randomization. The possibility of bias due to prior experience of the technician and the learning curve is inherent to the study design. Future trials aimed at evaluating outcomes with the use of similar materials in the operative reduction of fractures and different fracture morphologies could provide additional knowledge of expanded potential use.
Future advances in casting materials and techniques will necessitate modifications to treatment protocols as well as evaluation to ascertain safety and effectiveness. This current research provides a scoring system to evaluate the outcome of cast application and, once validated, will allow reliable and accurate comparisons.
Conclusion
Patients and caregivers were equally satisfied with the Wet or Dry® and Delta Dry® undercast padding materials. The technician-reported outcome measures reflected a preference for Delta Dry®. The use of a synthetic casting material with a waterproof liner provides a safe alternative for the management of simple forearm fractures in children.
Footnotes
Acknowledgments
The authors would like to acknowledge Ms. Sophie McCallum for her contribution to the data collection.
None.