
Abstract
Abstract
Purpose
The aim of this cross-sectional cohort study is to describe the incidence of joint laxity and the correlation between joint laxity and radiological migration of the hip in children with Down syndrome.
Methods
Sixty-five children (2–19 years) with Down's syndrome were examined for joint laxity. For each subject, laxity scores for joints were carried out with the Bulbena method. Plane pelvic radiographs were used to determine the migration of the hip, according to Reimer's migration index.
Results
In this study, 26 out of 65 children with Down's syndrome (40 %) were diagnosed with general joint laxity. On the radiographs of the hips we found a mean Reimer's Migration Index of 5.2 % for all the subjects. Children with general joint laxity showed a lower Reimer's Migration Index (2.1 %). No significant correlation was found between general joint laxity and migration of the hip.
Conclusions
This study showed no relationship between joint laxity and migration of the hip in children with Down's syndrome. This implicates that we were not able to prove that joint laxity is the major factor in developing hip migration in children with Down's syndrome.
Introduction
Down syndrome (DS) is the most common chromosomal disorder among newborns, with an estimated prevalence in the Netherlands of 16 per 10,000 live births (1.6 per thousand; 54 % boys) [1]. Subluxation and dislocation of the hip in this patient group is reported to be between 7 and 30 % [2, 4–6]. The symptoms are characteristically identified between the ages of 2 and 10 years [8, 9]. The etiology of this pathologic development is still not known. Joint laxity as a possible cause is discussed in several studies but remains questionable [3–5, 7, 8].
In the normal population, Carter and Wilkinson [6] demonstrated persistent generalized joint laxity in newborn infants to be an important predisposing factor in subluxation and dislocation of the hip. General joint laxity was found in 7 % of normal schoolchildren and in 45 % in children with congenital dislocation of the hip. They concluded that capsular laxity is an etiological factor and considered to be part of a generalized joint laxity affecting both axial and limb joints. In children with DS, Livingstone et al. [5] found two out of 39 children had general joint laxity. One of the children with no detectable joint laxity had a dislocated hip. They concluded that joint laxity is not a major etiological factor in joint problems in children with DS.
Next to joint laxity as a possible factor in femoral head migration, muscle imbalance, as described in children with cerebral palsy, is known as a main reason for subluxation of the hip [12, 18]. Reports on motor development of children with DS indicate a disturbance in dynamic stabilization of joints, especially in the leg [19]. From this observation, muscle imbalance could also be a main cause of migration of the hip.
In children with DS, the relation between joint laxity and hip migration with (sub)luxation has been poorly reported. The aim of our study is to describe in children with DS, the prevalence of general joint laxity, the prevalence of migration of the hip and their correlation.
Materials and methods
In the Netherlands, children with DS are regularly seen including a continuous follow-up of the child's gross motor function. In our outpatient clinic the children with DS have a standardized radiological follow-up of the hips.
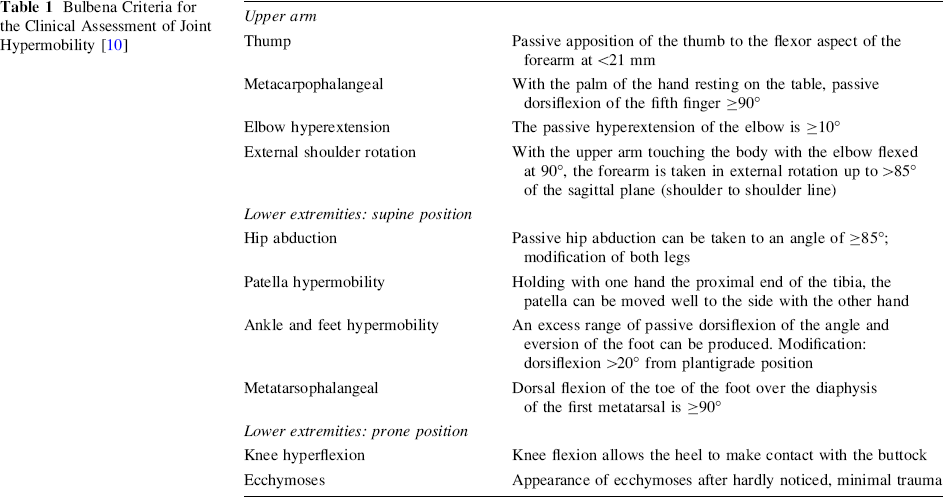
We examined all children with DS between 0 and 19 years, who were visiting our outpatient clinic between 2005 and 2008. Because of delayed development of walking in children with DS, the mean age of independent walking is after the age of 2 years [8]. In this study, patients were included when they were able to walk independently. This selection criterion was used because, in the absence of active muscle contraction, the joints of children with DS demonstrate lower stiffness which can affect the joint laxity scores [10]. Participants were taken through a standardized protocol which included weight, age, gender, pain localization as present, walking pattern, as well as general joint laxity. The extent of generalized joint laxity was quantified using the method of Bulbena [11]. This scale uses nine maneuvers plus the appearance of bruises to assess joint laxity (Table 1). General joint laxity was diagnosed when five of the 10 characteristics for girls and four of the 10 characteristics for boys were found. All scores were done by a specialized pediatric physiotherapist (MB) and a pediatric orthopedic surgeon (JEHP).
Bulbena Criteria for the Clinical Assessment of Joint Hypermobility [10]
Reimer's migration index was used on anterior-posterior (AP) radiographs as a method to assess migration of the hip. Fig. 1 shows an example of the measurement. Hilgenreiner's line and Perkins’ line were drawn as defined by Reimer [12]. The migration percentage was calculated as the visible part of the femoral head outside Perkins’ line divided by the total width of the femoral head multiplied by 100 [12]. The migration index of a normal hip is 0 % from 2 years to the age of 4 years and less than 10 % between the ages of 4 and 16 years [12]. A subluxated hip has a migration index of 33–99 % and a dislocated hip has a migration of 100 % [12]. Hips with a migration index >33 % have a high risk for further displacement, indicating the need for surgical intervention. All measurements were performed by one of the authors (JEHP).
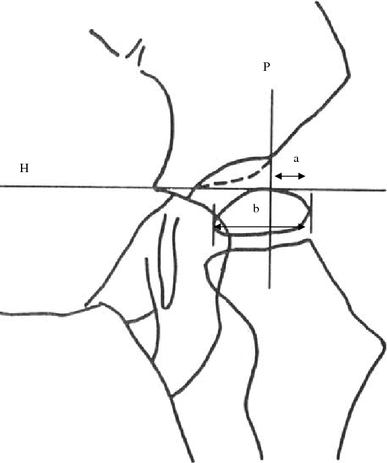
Reimer's hip migration percentage. This is calculated by dividing measurement a by measurement b and then converting the ratio into a percentage. P Perkins’ line, H Hilgenreiner's line
Data were processed by the statistical package SPSS. For statistical analysis, Spearman's rank correlation coefficient was used for quantifications of correlation.
Results
Between 2005 and 2008, 96 children with DS were seen in our outpatient clinic. Thirty-one patients (32 %) (mean age 1.2 years; range 0.5–3.0 years) were not able to walk at the time of investigation and were excluded for this study. Sixty-five children (68 %) (130 hips) could be included for this study. There were 22 girls (34 %) and 43 boys (66 %) (age range 2–19 years). In the girls’ group, six of 22 children (27 %) scored ≥5 on the Bulbena score. In 20 out of 43 boys (46 %), a Bulbena score ≥4 was found. There was no significance different in mean Bulbena score between boys and girls (p > 0.05). By combining boys and girls, 26 out of 65 children (40 %) scored above the cut-off point and can be seen as having general joint laxity.
On the radiographs of the hips we found a mean Reimer's Migration Index of 5.2 % for all the subjects. Children with general joint laxity showed a lower Reimer's Migration Index (2.1 %). A Reimer's Migration Index >33 % was seen in two children (four hips): one boy with and one girl without general joint laxity (Table 2).
Data on mean Bulbena score and Reimer's Migration Index (%) for girls and boys with DS
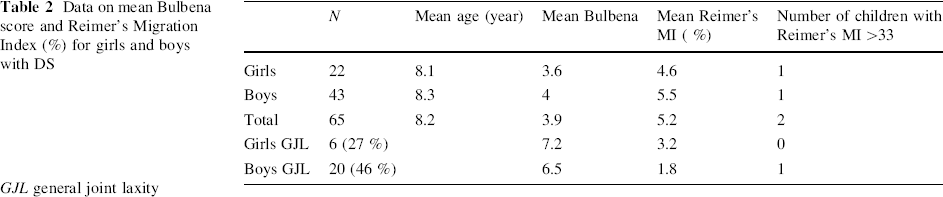
GJL general joint laxity
A significant negative correlation was found between age and joint laxity (Spearman rho −0.38; p < 0.05); joint laxity was more present at a younger age for the whole group.
Furthermore, there was a significant positive correlation between age and migration (Spearman rho 0.29, p < 0.05); migration of the hip was more present at an older age for the whole group.
In Table 3 the correlations between joint laxity and radiographic measurements of the hip are presented. No significant correlation was found between Bulbena joint laxity score and Reimer's migration index.
Correlation between Bulbena score and Reimer's migration index
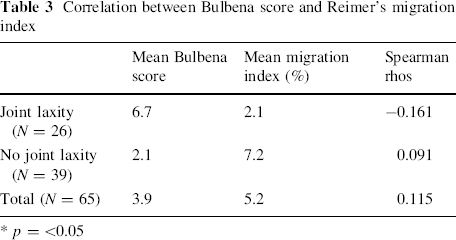
* p = <0.05
Discussion
In this cross-sectional study of 65 children with DS we determined the prevalence of general joint laxity, the prevalence of migration of the hip and their correlation.
In our study, there was no correlation between general joint laxity and migration of the hip in children with DS. We showed that the children with joint laxity demonstrated less migration of the hip (2.1 %) as compared to the children without joint laxity (7.2 %). The results of our study are in line with the conclusion of Livingstone et al. [5]. They concluded that joint laxity is not a major etiological factor in joint problems in children with DS. Furthermore, we found that two out of 65 (3 %) children with DS showed a subluxation of the hip. Compared to the published data about subluxation in children with DS [2, 4–6], our study showed a much lower percentage of subluxation. This can be explained by the fact that we, in contrast to the other published studies, included only the children who were able to walk.
In our study, 26 out of the 65 children with DS (40 %) had general joint laxity. This confirms that the prevalence of general joint laxity in children with DS is higher as compared to the 7–25 % in the normal population [6, 13, 14]. Few other authors have published the prevalence of joint laxity in children with DS but no congruous numbers exists [5, 7]. Semine [7] reported 65 out of 85 (76.4 %) children with DS with general joint laxity. By contrast, Livingstone & Hirst [5] described general joint laxity in children with DS to be 5 % (two out of 39). However, there are several methodological differences between the studies. The prevalence of hyperlaxity decreases with age [6, 15, 16]. We tested a slightly younger age group than Livingstone (mean 10.3 years) but a slightly older age group than Semine (mean 6.6 years). Furthermore, both studies did not mention if the children were able to walk independently at the time of including, which can affect the joint laxity scores [9]. Then there is a difference in scoring system. For measuring joint laxity Livingstone and Semine followed the criteria of Carter and Wilkinson [6]. Livingstone, compared to Semine, used a more strict interpretation of the criteria, which can explain part of the differences in outcomes. Carter and Wilkinson [6] developed the first clinical scoring system to measure laxity in children. In 1992, Bulbena introduced a new laxity scale with rather similar criteria. The new method proposed to be a more reliable instrument because of an improved internal consistency [11]. In addition, they established gender related cut-off points. Bulbena considered the new method the best ability to distinguish individuals with general joint laxity from those who did not have general joint laxity. In our study we used the Bulbena method, which may enable more reliability, because of a higher internal consistency and gender cut-off points.
Although women are known to be generally more lax jointed than men at all ages [14], this was not found in our study. The explanation is not clear. It may be caused by gender related cut-off points used by the Bulbena method or by the relatively small number of girls (34 %) participating in this study compared to normal DS population (46 % girls) [1]. Furthermore, we showed that joint laxity is negatively correlated with patient's age. In other words, joint laxity was more present at a younger age for the whole group. Hip migration may be the result of accumulation of joint laxity from birth to adolescence. A certain patient with relatively less joint laxity at the time of adolescence could have more severe joint laxity in earlier life. Because of our cross-sectional study, we don't know the accumulation effect of joint laxity.
In the literature there is conflicting evidence for joint laxity as a factor for development of hip migration [4–6, 17]. El-Shahaly [17] demonstrated that 2 % (2/108) of the normal children with joint laxity showed a subluxation of the hip. In our study group we found 3 % (1/36) of the children with joint laxity had a subluxation of the hip. Carter and Wilkinson [6] presented that 45 % (33/74) of the children with a congenital dislocation of the hip had joint laxity. They concluded that persistent general joint laxity is an important predisposing factor to congenital dislocation of the hip. However, they used a selective population with just children with a congenital dislocation of the hip.
In our cross-sectional study, we showed that joint laxity is more present in children with DS, compared to the normal population. However, no correlation was found between joint laxity and migration of the hip. This data implicates that we were not able to prove that joint laxity is the major factor in developing hip migration in children with DS. Other factors than joint laxity, such as muscle imbalances around the hip, described in children with cerebral palsy, seem to play a more important role in developing hip migration. There are, however, no reports on muscle imbalance and migration of the hip in children with DS. Only few reports describe that the ability to stabilize the hip and knee joint by a counteracting force of different muscle groups is less developed in children with DS [19]. This indicates that muscle imbalance might play a more important role in developing hip migration. Further research is needed to establish the relation between muscle imbalance and migration of the hip in children with DS.
Footnotes
None.