
Abstract
Abstract
Purpose
The aim of our study is to report our complication rate and analyze the associated risk factors when removing cannulated stainless steel screws for SCFE fixation.
Methods
This was a multicenter retrospective study of patients who underwent removal of cannulated stainless steel screws after a mean time of 2.03 years of implantation. Thirty-two patients were included (38 hips) with a mean of 13.7 years of age during screw removal surgery. The mean post-removal follow up time was 1.6 years. In all cases the removal of screws was done systematically. Demographic data, possible risk factors related to removal failure, as well as post-removal complications such as post-removal fractures, infections and scar issues were recorded.
Results
A removal failure rate of 15.79 % (6/38) was found. The removal surgical time was longer than the initial fixation time but without statistical significance (70.78 vs 61.84 m, p = 0.196). However, the duration of screw implantation (r2: 7.09; IC: 1.12–13.06) and screw head bony coverage (r2: 21.32; IC: 5.58–37.06) were both related to this prolonged time. Multivariant analysis revealed that a fully threaded cannulated screw had the lowest removal failure risk (OR: 0.3; IC: 0.14–0.61). There were no postremoval complications recorded.
Conclusions
We recommend to use full threaded cannulated stainless steel screws and to perform the procedure as soon as the physis are closed to decrease the surgical time. It is a safe procedure based on a low rate of complications such as post-removal fractures, infection and scar issues.
Keywords
Introduction
The paediatric skeleton differs in many respects from that of the adult. Despite its greater capacity for healing and remodelling, internal fixation is required in many circumstances [1]. Metal removal is one of the most commonly performed operations in paediatric orthopaedics; however, indications are controversial in asymptomatic patients after completion of bone union [2]. It has generally been recommended that implants in children be removed to avoid stress shielding and allow complete remodelling of the bone, and to decrease the risk of infection, allergic reaction, ion toxicity, and possibility of malignant transformation [3, 4].
Slipped capital femoral epiphysis (SCFE) is the most common hip disorder in adolescents and its treatment is based on the premise that the onset of osteoarthritis is directly related to the severity of slip [5]. The most common initial treatment is in situ screw fixation and later degenerative joint disease is a concern [6]. Major problems can be expected when arthroplasty is necessary years later, if the screws are still inside the proximal femur [7].
According to Raney et al. [8] an overall complication rate for implant removal surgery could be 10 %; however, the reported rate for slipped capital femoral epiphysis (SCFE) implant removal could be up to 34 %, accounting for 44 % of all reported complications. There have been several reports of difficulty in removing implants, ranging from 33 to 83.3 % [5, 7, 11] of failure, due to a heterogeneous type of implant used. Actually, screws are the prefered implants utilized. Several risk factors have been described, the screw type being one of the most important. The usage of cannulated titanium screws is associated with high implant removal rate failure; based on this fact, some authors have advocated fixation using cannulated steel screws [5]. We think that the failure rate during this procedure is still high, as in this sense, so we analyzed the possible associated risk factors.
Materials and methods
The operating room database was queried at our level I pediatric orthopaedics divisions to identify those patients who underwent steel screw fixation due to slipped capital femoral epiphysis (SCFE). For each of those patients, surgical notes were screened in order to identify those who underwent removal of implants. We further included only those patients who were treated at our centers with a minimum follow up of 3 months. Patients were excluded if they were treated in outside facilities, if there was not complete information within their medical charts or pre- and post-surgical hip radiographs, and those with less than 3 months of follow up. All implants were removed systematically after proximal femur physeal closure. All procedures were performed under general anesthesia by orthopaedic attending surgeons through either an open approach (84.21 %) or a percutaneous technique (15.79 %) using a “C-arm” to verify screw position.
For those patients who met the initial inclusion criteria, surgical notes, clinical charts and pre- and post-surgical radiographs were retrospectively reviewed to determine demographic information such as age at SCFE fixation, age at removal of screw, gender, affected hip, duration of screw implant, severity of SCFE and follow up time. Surgical notes were reviewed for surgical time of SCFE fixation, surgical time of implant removal, threaded length (16, 32 mm, full threaded), presence of bone covering screw head, screw diameter (6.5, 7.3 mm), screw length and failure of screw retrieval. Follow up radiographs and clinical charts from each visit were assessed for the presence of complications such as fracture after removal of implant, superficial or deep infections and scar issues. The failure of screw retrieval was defined for purposes of this study as either the inability to remove the entire screw or breakage and retaining of a fragment of the screw involved.
Between January 1996 and December 2011, we identified 32 patients (38 hips) that met the inclusion criteria. There were 21 boys and 11 girls. The average age of the patients in our series during SCFE fixation was 11.75 years (range 8–14 years) and during screw removal was 13.68 years (range 12–15.5 years). The left hip was affected in the majority of cases (63.16 %). The mean time of screw implant duration was 2.03 years (CI: 1.64–2.43). and the mean follow up time after screw removal was 1.57 years (range 1–3 years).
Statistical analysis
Distribution of frequencies were used for qualitative variables and the mean with its 95 % CI for quantitative variables. Risk factors were compared between the group that achieved a successful removal of the screw and the group in which the removal failed using the Fisher's exact test and the non- parametric Mann–Whitney test based on the nature of the variable (qualitative vs quantitative). A logistic regression was performed to find out the relationship between the final outcome (removal failure) and the possible risk factors. An OR and its 95 % CI were obtained. Finally, a linear regression was done to assess the possible variables associated with a prolonged removal of implant surgical time (SPSS version 16.0, SPSS Inc., Chicago, IL). Statistical significance was set at alpha level of p = 0.05.
Results
During the treatment period, six of 38 hips met the criteria for screw removal failure (15.8 %). Based on bi-variable statistical analysis, threaded length (16, 32 mm, full threaded) was the only variable found to be significantly different between the ones with a successful removal and those with a failed one (Table 1).
Bi-variable analysis of potential risk factors for screw removal failure in the entire group of patients
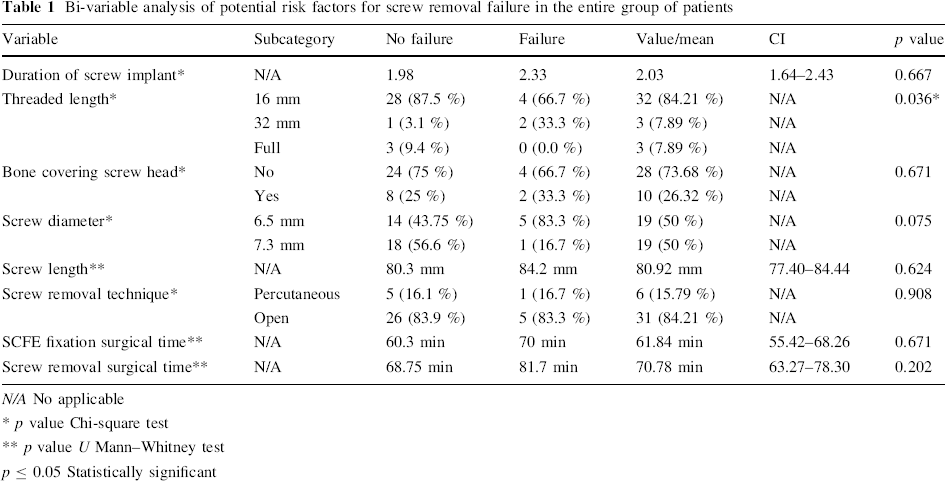
N/A No applicable
p value Chi-square test
p value U Mann–Whitney test
p ≤ 0.05 Statistically significant
Multivariate logistic regression revealed that the threaded length was a “protective” factor, being a longer threaded screw associated with less risk of failure during screw removal (full threaded vs 32 vs 16 mm) (OR: 0.3; CI: 0.14–0.61).
Of the six hips in which the screw removal was not successful, in four cases it was not possible to remove the implants, and in the other two cases, the screws were partially cut, as it was not possible to put them back or remove them completely (Fig. 1a, b).
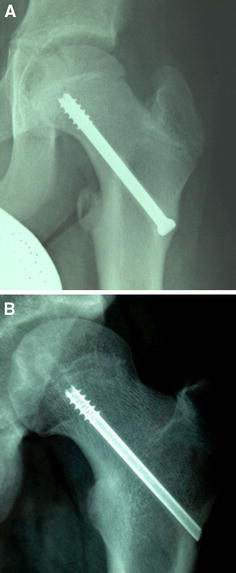
9 year old girl in whom a percutaneous stainless steel screw fixation was performed due to a right SCFE. At 13 years old, screw removal was attempted with no success.
The mean surgical time during SCFE fixation was 61.8 min (range 55.4–68.2 min) and during screw removal was 70.8 min (range 63.3–78.3 min); even though screw removal procedure tends to be a longer procedure, we were not able to find a statistically significant difference (p = 0.196). When the screw removal surgical time was analyzed by linear regression, it revealed that the duration of screw implant was related to a longer surgical time (coefficient: 7.09; CI: 1.12–13.06) as well as coverage of the head's screw by bone (coefficient: 21.32; CI: 5.58–37.06) (Table 2). If the duration of screw implant is greater than 2 years, the screw removal surgical time is increased by 16 min (coefficient: 16.75; p = 0.045).
Linear regression analysis to assess possible variables related to a prolonged screw removal surgical time
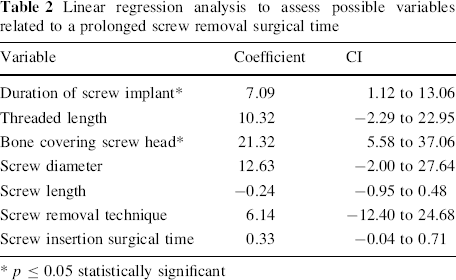
p ≤ 0.05 statistically significant
There were no fractures after screw removal, or superficial or deep infections, and no scar issues.
Discussion
Slipped capital femoral epiphysis (SCFE) is an adolescent hip disorder in which there is a displacement of the metaphysis that moves superiorly and anteriorly, with the epiphysis held in the acetabulum by the ligamentum teres [6]. Once a diagnosis is made, treatment is indicated to prevent slip progression and to avoid complication, especially osteonecrosis and chondrolysis [6, 9, 10].
Cannulated screws are commonly used because they can be accurately placed under fluoroscopic control through small incisions. The necessity for pin removal after closure of the physeal plate is widely accepted in adolescents due to the risk of trochanteric bursitis [11, 12], proximal femur fractures because the pin acts as a stress riser [5, 13], present difficulty with subsequent arthroplasty and the theoretical risk of neoplasia from long-term corrosion at the metal/bone interface [5, 14].
Even though Vresilovic et al. [5] reported no failures during stainless screws removal, we found a failure rate of 15.8 %. There have been few studies dealing with risk factors associated with surgical removal failures rates [5, 7]. Vresilovic et al. [5] found that failure of pin removal was dependent on weight of the patient at the time of pin removal, duration of pin implantation, and the type of pin implanted. However, there were no significant differences in patient weight or in duration of implantation when compared by pin type. Therefore, they concluded that pin failures based on pin type are not secondary to population differences. In our study, the type of screw was not taken into account since in all cases stainless steel screws were used. After performing a bi-variable analysis (Table 1) of potential risk factors, the threaded length was the only variable found to be statistically significant. We found that with a full threaded screw, the risk of failure was the lowest. This finding is based on the fact that a fully threaded cannulated screw does not need a cutting back mechanism; however, it might lead to a higher initial torque due to a larger contact area of the screw and bone [11]. This was observed in some of our cases. It's also important to bear in mind that stainless steel screws have a lower fatigue and yield strength in comparison to titanium, predisposing them to an occasional risk of breakage. We didn't have any case like this. The only screws which broke did so after an unsuccessful attempt to remove them and the screws had to be cut.
It has been observed that screw removal surgical time varies in comparison to the initial fixation surgical time [7, 15]. Ilchmann et al. [7] found a mean fixation surgical time per pin of 25 min (13–46 min) and a mean removal surgical time of 51 min (17–107 min), this being two times the fixation time. Lee et al. [15] also found a significantly higher removal operative time; in both studies, titanium screws were used. What about stainless steel screws? Lee et al. [15] didn't find such a difference among surgical times; however, we found a longer removal surgical time in comparison to the fixation operative time without a statistically significant difference. How can this finding be explained? Titanium has been suggested to provide an interface to bony tissues that allows greater bony apposition to the implant than does stainless steel [16, 17]. If this is true, removal of similarly configured titanium requires greater forces and probably longer operative times than removal of stainless steel screws.
There is some controversy with regard to the variables associated with this increased removal surgical time. In the case of titanium screws, Ilchmann et al. [7] reported no correlation between surgical removal time and duration of screw implant (r2 = 0.059, linear regression); however, Lee et al. [15] observed an association between the duration of screw implant and a cutoff time of 12 months. In our study using stainless steel screws, we found a correlation between duration of screw implant and an increase of 16 min if the screw was implanted for more than 2 years. This could be explained by the fact that with a longer time of implantation, a harder bone/screw interface could be formed. We also found that bone covering the screw head was a statistically significant variable that prolongs the surgical removal time (Table 2). It's possible to see this bone covering the screw head in a pre-operative plain X-ray of the affected hip; in these cases, we recommend performing an open approach since starting with a percutaneous approach may further increase the surgical removal time. These two variables are important to take into account when discussing the details of the surgery with the parents and patients, since having a screw implanted for a long time and bone covering the screw head (also related to the time of implantation) may increase the surgical removal time with the possible issues related to this.
There have been few complications associated after performing this procedure. Ilchmann et al. [7] reported two proximal femoral fractures through the former entry point of the screw due to weakness of the lateral femoral cortex because a chisel was used at the time of screw removal. In our study, there were no complications such as fractures, infection and scar issues during the follow up time. We think that it's important to recommend protected weight bearing in the cases where the lateral femoral cortex was weakened.
This study has some limitations such as its retrospective nature, the lack of long-term follow up to assess the long-term outcome of the affected hips and the need for joint arthroplasty and even we found some variables to be significant, the sample size is small. Regardless of these limitations this study indicates, that even though some studies recommend the use of cannulated stainless steel screws instead of cannulated titanium screws for fixation of SCFE to decrease the failure of removal rate, it is still higher in comparison to the overall complication rate of implant removal within the pediatric population. In order to decrease this removal failure rate we recommend the use of fully threaded cannulated screws and to perform the procedure as soon as the physis are closed to decrease the surgical time. Also, it is important to observe if the screw head is covered by bone so an open approach could be done initially with the subsequent decreased risk of increasing the operative time. We think it is a safe procedure based on a low rate of complications such as post-removal fractures, infection and scar issues.
Footnotes
The authors didn't receive any financial support related to the study.
IRB approval was not needed.