
Abstract
Purpose
The Scoliosis Research Society-22 (SRS-22) questionnaire is a widely accepted questionnaire used to assess the health-related quality of life for scoliosis patients in the United States. However, its adaptation in other languages is necessary for its multinational use. A cross-sectional study was performed to evaluate the validity and reliability of an adapted Thai version of the SRS-22 questionnaire.
Methods
An expert committee performed translation/retranslation of the English version of the SRS-22 questionnaire, as well as a cross-cultural adaptation process. Later, SRS-22 questionnaires and previously validated Short Form-36 version 2 (SF-36v2) outcome instruments were given to patients treated for idiopathic scoliosis with a minimum of 1 year of follow-up. Internal consistency and reproducibility were determined by Cronbach's alpha statistics and the intraclass correlation coefficient, respectively. Concurrent validity was measured by comparing SRS-22 results with a previously validated questionnaire (SF-36v2). Measurement was made using the Pearson correlation coefficient (r).
Results
The study showed satisfactory internal consistency with Cronbach's alpha values for all of the corresponding domains (pain, 0.72; self-image/appearance, 0.87; mental health, 0.83; satisfaction with management, 0.63; and function/activity, 0.83). The test–retest reproducibility was also excellent or good for all domains (pain, 0.72; self-image/appearance, 0.85; mental health, 0.82; satisfaction, 0.62; and function/activity, 0.81). For concurrent validity, excellent correlation was found in two domains, good in six domains, moderate in five domains, and poor in five domains of the 18 relevant domains.
Conclusions
The Thai version of the SRS-22 outcome instrument has satisfactory internal consistency, excellent reproducibility, and acceptable validity.
Introduction
Idiopathic scoliosis is the most common type of back deformity [1]. Although it does not result in death, it usually interferes with the quality of life of the patient. The goal of the treatment for these patients is to improve the deformity and prevent further progression of the curve. These outcomes improve the quality of life of these patients. In the past, we evaluated the outcomes by measuring the corrected curve both clinically and on radiographic film, but did not measure its effect on the patient's physical and mental well-being and quality of life [2, 3]. The Scoliosis Research Society-22 (SRS-22) questionnaire addresses the patient's perception of their medical condition and self-image, and its development has allowed us to effectively evaluate the impact of treatment on quality of life. The strengths of this questionnaire are the simplicity of the questions, its specificity to idiopathic scoliotic patients, and its reliability and concurrent validity. This questionnaire was invented by Haher et al. [4] and then improved by Asher et al. [5–7] into the English version. It is widely used in the English-speaking countries. It has also been translated into many other languages, such as Turkish [8], Spanish [9], and Chinese [10] versions. As Thai people are culturally distinct, it is important to adapt and translate the SRS-22 questionnaire into Thai and to validate it before its use.
The purpose of this study was to assess the Thai version of the SRS-22 and to determine its reliability and concurrent validity.
Materials and methods
The study was performed according to the recommended protocol issued by the American Association of Orthopedic Surgeon (AAOS) outcomes committee and as outlined by Beaton et al. [11]. Firstly, the English version of the SRS-22 questionnaire was translated independently into Thai by two bilingual translators whose native tongue was Thai. After comparing the two translations, the different points were identified and resolved by consensus. Two native English speakers who were also fluent in Thai then retranslated this Thai version into English. The expert committee, which was composed of two spine surgeons (WL, WW), four translators, and two researchers (PL, GK), further assessed the forward and back translations, and then a consensus was achieved on the final translation.
The research ethics committee of our institute approved this study and informed consent was obtained from all participants. Two surveys, one for evaluating the validity and the other for evaluating the reliability, were carried out at a single center, the Spine Unit of Ramathibodi Hospital. We included all patients who were diagnosed with idiopathic scoliosis treated by either surgery or conservative method for at least 1 year prior inclusion. The data were collected at the outpatient clinic during the study period between September 2008 and October 2009. Other criteria included age more than 12 years and an understanding of the Thai language. For the first survey, each patient completed the SRS-22 questionnaire (Thai version) and the previously validated Thai version of the Short Form-36 version 2 (SF-36v2) health survey questionnaires [12–14]. By comparing the scoring in the correlating domains of the SRS-22 and SF-36v2, we could then determine the validity of the Thai version of the SRS-22 questionnaire [15].
A second survey was then performed about 10 days later. We sent the SRS-22 questionnaire (Thai version) to the same patients and then returned the completed form by mail. This test–retest design was used to measure the temporal stability of the questionnaire. The reproducibility of the Thai SRS-22 was then evaluated by comparing the domain scores of the two surveys.
Statistical analysis
Reliability assessment of the Thai version of the SRS-22 questionnaire was determined by calculating Cronbach's alpha statistic and intraclass correlation coefficient (ICC) values. According to Asher et al. [6], the Cronbach α of internal consistency was defined as follows: very satisfactory (Cronbach α 0.80–0.89), good (Cronbach α 0.50–0.79), lower than the original questionnaire <0.5. For test–retest reproducibility, the ICC was defined as follows: excellent (ICC ≥ 0.75), good (ICC 0.40–0.75) [16]. Concurrent validity was evaluated by comparing SRS-22 domains with relevant domains in the SF-36 questionnaire. Correlation was made using the Pearson correlation coefficient (r), interpreted as: excellent >0.75, good 0.50–0.75, moderate 0.25–0.50, poor <0.25 [8, 10]. Statistical difference was defined as a P-value of less than 0.01. All analyses in this study were calculated by STATA 10.0 (STATACORP, College Station, Texas).
Results
In total, 34 patients met the inclusion criteria during the study period. Four patients did not complete or return a second questionnaire, thus, 30 patients were enrolled in the study. There were two males and 28 females, with a mean age of 17.2 years (range, 13–30 years). The mean gap between the first and the second mailings was 10 days (range, 7–14 days).
The distribution of scores for five SRS-22 and nine SF-36v2 domains in terms of domain means, minimum floor score, and the ceiling and floor effect for both of the translated Thai versions of SRS-22 and SF-36v2 are shown in Table 1. All of the SRS-22 domains demonstrated a low level of floor effect (less than 7%, as shown in Table 1), but a domain (vitality) of SF-36v2 exhibited a high level of floor effect (more than 7%). Three domains of SRS-22 (pain, functional/activity, and satisfaction with management) and six domains of SF-36v2 (physical function, role limitations due to physical health problems, role limitations due to emotional problems, social functioning, bodily pain, and health transition) resulted in a high level of ceiling effect.
Descriptive statistics on individual domain scores
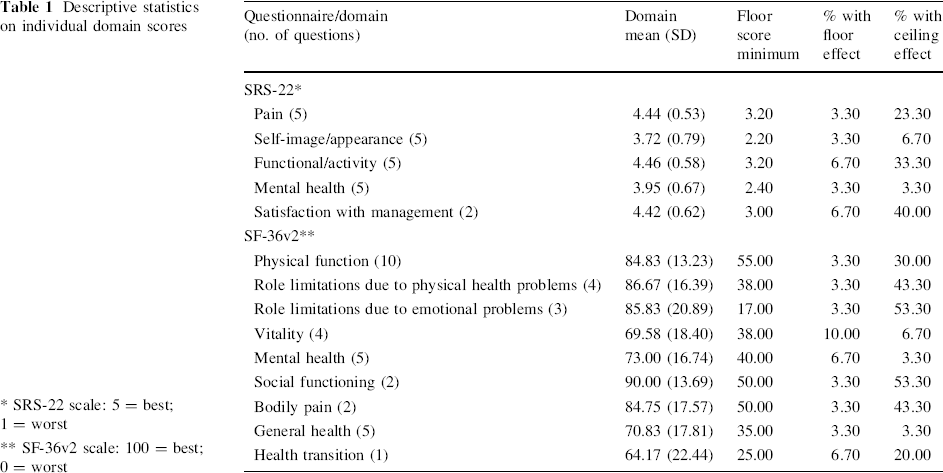
SRS-22 scale: 5 = best; 1 = worst
SF-36v2 scale: 100 = best; 0 = worst
Table 2 shows the comparison between SRS-22 and SF-36v2 domains by converting the score of the SRS-22 from a 0–5 to a 0–100 scale, followed by analysis distribution into quartiles. Score distributions were weak and tended to be high in all domains of SRS-22 and in the SF-36v2 domains of physical function, role limitations due to physical health problems, role limitations due to emotional problems, social functioning, bodily pain, and health transition.
Distribution of SRS-22 and SF-36v2 domain scores by quartiles
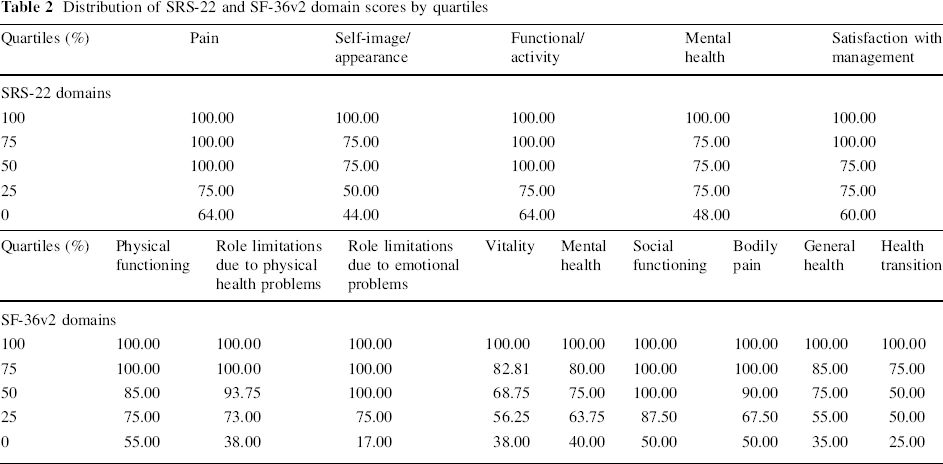
Table 3 shows the internal consistency assessment of SRS-22 by using the Cronbach's alpha value. The results were very satisfactory (Cronbach α = 0.80–0.89) in the self-image/appearance, functional/activity, and mental health domains, and showed good consistency (Cronbach α = 0.50–0.79) in the pain and satisfaction with management domains. Also, the Cronbach's alpha value of SF-36v2 had a similar value from a previous publication, thus, we could calculate the concurrent validity properly [13].
Internal consistency reliability (Cronbach's alpha value)
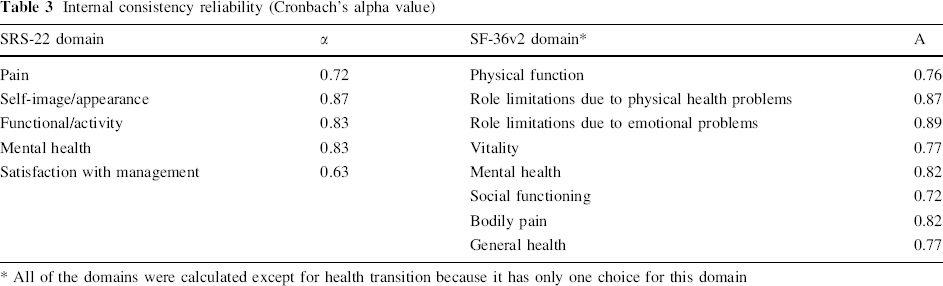
All of the domains were calculated except for health transition because it has only one choice for this domain
Table 4 shows the test–retest reproducibility by using statistical analysis of the ICC. There were excellent (ICC > 0.75) results in all of the domains except for pain and satisfaction of management, which showed good (ICC = 0.40–0.75) results.
Test–retest reproducibility as determined by the intraclass correlation coefficient (ICC)
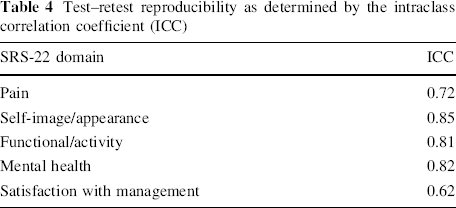
Table 5 shows the concurrent validity in comparison with SF-36v2. The correlation was calculated by the Pearson correlation coefficient (r). We found statistical significance in all of the domains except that in satisfaction with management of the SRS-22, which did not correlate with all of the related domains of SF-36v2 (physical function, role limitations due to physical health problems, bodily pain, general health, and health translation). So, there was excellent correlation (r ≥ 0.75) in two domains, good (r = 0.50–0.75) in six domains, moderate (r = 0.25–0.50) in five domains, and poor (r < 0.25) in five of the 18 relevant domains.
Concurrent validity of SRS-22 domains with relevant SF-36v2 domains as determined by the Pearson correlation coefficient (r)
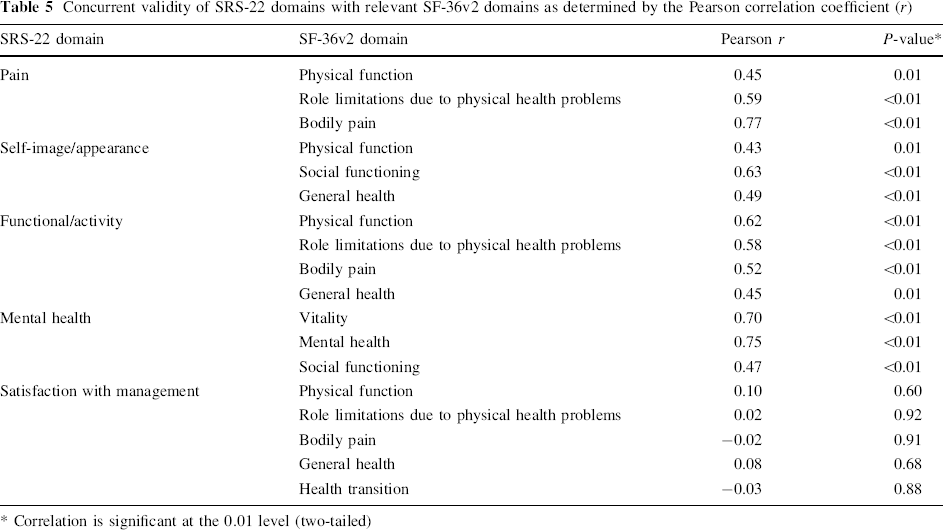
Correlation is significant at the 0.01 level (two-tailed)
Discussion
In this study, we culturally and linguistically adapted the SRS outcome instrument (SRS-22) into Thai. The first part of the study showed that most of the patients recruited into the study expressed mild clinical complaints, as the lowest score in all of the domains was only 2.2 and the percentage of floor effect in each domain was also less than 7%. The score distribution, in Table 2 (converting the score of SRS-22 from 0–5 to 0–100), shows that, in each of the domains, most of the patients had a score of more than 50 and many over 75. This score distribution correlates well with the SF-36v2 scores and represents that the patients could answer both questionnaires in the same way.
The mean value of the Cronbach's alpha obtained from the Thai version of SRS-22 was slightly lower than the original study (0.78 vs. 0.86) [6]. Although this tendency has been observed in other transcultural adaptations of questionnaires [9], the lower internal consistency of satisfaction with management domain was principally responsible for the lower Cronbach's alpha value. This might be explained by the fact that Thai people usually have respect for doctors. For example, though they are unsatisfied with the result of their back treatment, they are likely to respond that they are happy with the treatment. Conversely, in the second question of this domain, “Do you want to have the same management if you have the same condition?”, they select the choice “no” instead of stating that they are unsatisfied with their treatment. Therefore, low Cronbach's alpha value was identified in this domain. In addition, as there are only two questions in this domain, the internal consistency showed a slightly lower value of Cronbach's alpha.
The test–retest reproducibility demonstrated excellent or at least a good reproducibility with high ICC levels in all domains which are comparable to the original questionnaire [5]. This means that there was acceptable reproducibility of this Thai version of the SRS-22 questionnaire. Moreover, the study of concurrent validity resulted in an excellent correlation coefficient when compared with SF-36v2, except in the satisfaction of management domain. As stated above, the possible reasons for this point include the fact that the response to these questions in the SRS-22 relate to the patient's feelings toward their physician's treatment. Since Thai patients are considerate of their doctors’ feelings, it is possible that they usually respond in a positive way. On the other hand, the correlated domain from the SF-36v2 usually refers to the patient's feeling towards their back condition or their limitation of activity, and Thai patients are more likely to respond accordingly. Secondly, Lai et al. demonstrated that the SRS-22 management satisfaction domain correlated poorly with the related domains of SF-36, while the other domains showed a satisfactory correlation [16]. Consequently, we propose that the lower correlation coefficient in our study was a reflection of both the intrinsically poor correlation of the satisfaction with management domain of the SRS-22 with the related domains of SF-36 and the Thai culture, rather than a validity problem of the translated questionnaire. The satisfaction with management domain in our translated SRS-22 should be carefully interpreted when this questionnaire is used in scoliosis patients.
There are a number of limitations of our study. The number of subjects could have been greater. In addition, the study was conducted at one institution; a multicenter study would provide a wider range of severity of scoliosis patients, which may improve the quality of analysis. However, we could demonstrate a reliable, valid, and reproducible translated questionnaire using a sample size recommended by the guideline for cross-cultural adaptation process, which could be used further in clinical scoliosis research in our societies.
Conclusion
In order to effectively use a health-related quality of life questionnaire across cultures, we always consider both cultural adaptation and linguistic translation as important issues. The Thai version of the Scoliosis Research Society-22 (SRS-22) outcome instrument has satisfactory internal consistency, good to excellent reproducibility, and acceptable validity. Thus, it may be used as a standard assessment in clinical studies of idiopathic scoliosis in Thai language societies.