
Abstract
Objective
To investigate the effect of coronavirus disease 2019 restrictions on ultrasound (US) screening of developmental dysplasia of the hip (DDH) in a children’s hospital.
Methods
The records of US screening of DDH were retrospectively evaluated in the pandemic period (April 2020 to July 2021) and the pre-pandemic period (January 2019 to February 2020). The monthly US number, sex, radiologist number, and age at the initial examination were recorded.
Results
A total of 6107 US scans were performed during the pre-pandemic period, which significantly decreased to 3340 during the pandemic. The number of monthly US scans performed did not change between the pre-pandemic (142.7/month) and pandemic (128.2/month) periods. The number of delayed examinations in the total population did not significantly change between the two periods. However, the number of delayed examinations in patients with abnormal hips was significantly increased during the pandemic compared with that in the pre-pandemic period.
Conclusions
Coronavirus disease 2019 restrictions decreased the US screening rate of DDH by almost half, but the number of US scans performed by each radiologist was unchanged. The compliance with follow-up recommendations was reduced by half, which may lead to an increase in the incidence of delayed and untreated DDH cases.
Keywords
Introduction
Developmental dysplasia of the hip (DDH) is a generic term for a wide spectrum of conditions, from mild hip joint laxity to frank dislocation. DDH occurs because of the absence of normal maturation and is the most common congenital cause of a hip prosthesis. 1 The incidence of DDH varies by region and ethnicity. Moreover, DDH is more common in regions such as southeastern Turkey where tight swaddling is customary. The estimated incidence of DDH in Turkey is 0.5% to 1.5%, which is high compared with that in other nations. 2
Hip ultrasound (US) is a well-established tool for evaluating the hip in infancy because a clinical examination may be insufficient for diagnosis, especially in the neonatal period. The method of hip US screening was first introduced by Graf. 3 In this method, the hips are categorized according to the structure of the bony roof, shape of the bony rim, and the coverage of the cartilaginous roof. Additionally, angles are measured for classification between three reference points (acetabular labrum, bony acetabular rim, and lower iliac margin). 4 Graf’s method is widely used for US screening of DDH. The accuracy of US screening is highest when performed between the 4th and 12th weeks of life. 5 Some centers routinely perform US screening in the first weeks of life to start treatment as early as possible, whereas others extend the period up to 6 months of age.6–9 Early US screening can lead to a high incidence of false-positive results and unnecessary follow-up examinations, and screening at later than 3 months reduces the accuracy of the US examination and can lead to a delay in the proper treatment. 6 Because the prognosis of DDH is highly correlated with the time of diagnosis, early screening is important.
There are two approaches for determining the population for DDH screening. In selective US screening of DDH, infants are referred for routine screening owing to abnormal clinical findings or when considered at particular risk for DDH (e.g., breech presentation, foot deformity, or a recent family history of DDH), whereas in universal screening, all infants are recruited for screening.10,11 In Turkey, the selective DDH US screening program was started by the Ministry of Health in 2010.
During the coronavirus disease 2019 (COVID-19) pandemic, several measures have been implemented in Radiology Departments. International and national societies have published guidelines that adhere to the COVID-19 restrictions. 12 In addition, various recommendations have been published regarding the continuation or postponement of screening programs.13,14 During the pandemic period, the number of daily active radiologists has decreased, and the time interval between each US examination has extended in the author’s center, but US screening of DDH has been conducted according to the earlier schedule. The author’s hospital is a referral children’s hospital for the southeastern region of Turkey, where several patients are admitted from nearby cities. Consequently, a decline in the number of US screening of DDH in the COVID-19 period was expected because of external restrictions (transportation and other social measures) and internal restrictions (hospital) that have been implemented along with anxiety faced by the general population.
In this study, the first objective was to evaluate changes in the number of US screenings of DDH during the pandemic. Because previous reports evaluated only the first few months of the pandemic,15,16 this study aimed to examine the effect of the longest period of COVID-19 restrictions on a screening program. The second objective was to determine the ratio of infants older than 3 months who received delayed admission. The third objective was to compare the number of hip joints with abnormalities of dysplastic or dislocated hips detected by US before and during the COVID-19 pandemic, which indicate potentially missed cases of DDH.
Materials and methods
Ethical considerations
This retrospective study protocol was approved by the University of Health Sciences, Diyarbakır Gazi Yasargil Training and Research Hospital Noninvasive Clinical Research Ethical Committee (approval number: 2022/5, date of approval: 14/01/2022). All details of the patients were de-identified for the study. Informed consent was waived because of the retrospective design of the study and the anonymous use of clinical data. The reporting of this study conforms to the STROBE guidelines. 17 US examinations of the hip were performed within the framework of the DDH screening protocol.
Subjects
In the first phase of the study; the radiology archive of Diyarbakır Children’s Hospital was searched to identify the number of US screenings of DDH that were performed between 1 January 2018 and 31 December 2021. The search yielded 16,881 infants with 17,332 US examinations. In the author’s hospital, US screening is ideally performed between the fourth and 12th weeks of birth at outpatient clinics. However, patients in the neonatal inpatient clinics and neonatal intensive care unit are examined just before leaving the hospital if they are discharged after the second week of life. Accordingly, the US examinations performed were divided into two groups (2–12 weeks and >12 weeks) according to the age at examination.
In the second phase of the study, two study groups were created according to the COVID-19 lockdown and restrictions. In Turkey, the first COVID-19 case was reported on 11 March 2020, and a few relevant restrictions were gradually implemented. A flexible working arrangement and extended time interval for the examinations started on 1 April 2020. The lockdown period and local travel restrictions ended on 1 July 2021. Accordingly, the pandemic period was defined as between 1 April 2020 and 1 July 2021. In August 2020, US examinations were not performed at our hospital because of the absence of an attending radiologist. Consequently, the pandemic period in this study was defined as 14 months, and for comparison, the duration of 14 months before the pandemic between January 2019 and March 2020 was defined as the control period. The purpose of the first phase of the study was to determine the seasonal changes of the number of US screenings overall, and the second phase of the study provided data regarding the whole period of COVID-19 restrictions.
US examination and classification
All US reports were evaluated individually, and the patients’ age, sex, Graf type, compliance with follow-up, and treatment for the pathological hips were noted. According to Graf’s method 4 and the follow-up records, the infants were classified as type I, type IIa (normal on follow-up), type IIa (absent for follow-up), type IIb (delayed initial examination), type IIb (following type 2a), type IIc, type D, type III, and type IV. The author divided type IIa and type IIb cases to determine missed follow-up for type IIa and delayed admission for type IIb. The number of US examinations in the study was 451 more than the number of patients, and the majority of those were type IIa (followed by type IIb). Although we enrolled the patients for US screening of DDH until 31 July 31 2021, the search for treatment and follow-up was extended until 30 November 2021 because follow-up may occur after several weeks. Additionally, the number of US examinations performed by each radiologist each month was recorded.
Statistical analysis
Statistical analysis was performed using the IBM Statistical Package for the Social Sciences (SPSS) 25.0 (IBM Corp., Armonk, NY, USA). The Kolmogorov–Smirnov test was used to evaluate the normal distribution of the data. Student’s t-test and analysis of variance were performed to compare parametric data. Pearson’s chi-square test was used to compare non-parametric data. Mean values and standard deviations were calculated for the descriptive data.
Results
During the pandemic and control periods, 9676 infants underwent a US examination of the hip. The annual and monthly changes in the number of infants with US screening of DDH from 2018 to 2021 in the author’s institution are shown in Figure 1. The mean monthly number of US screenings was 451.5 ± 83.8 in 2018, 439.8 ± 96.9 in 2019, 263.5 ± 93.8 in 2020, and 306.3 ± 77.4 in 2021. Infants whose initial examinations were at the ideal examination time were compared with the entire study sample. In 2018 and 2019, 93% of infants were classified as the ideal (2–12 weeks of age) period. This rate increased at the beginning of the pandemic period (2020) to 95% and then decreased slightly to 92% by 2021. However, no significant difference was found between the annual percentages (p = 0.089). The monthly percentages of examinations at the ideal time are shown in Table 1.

Line graph of the number of ultrasound screenings of developmental dysplasia of the hip each month by year.
Ratio of infants who were admitted for ultrasound screening of developmental dysplasia of the hip between the second and 12th weeks of life to the entire study sample.
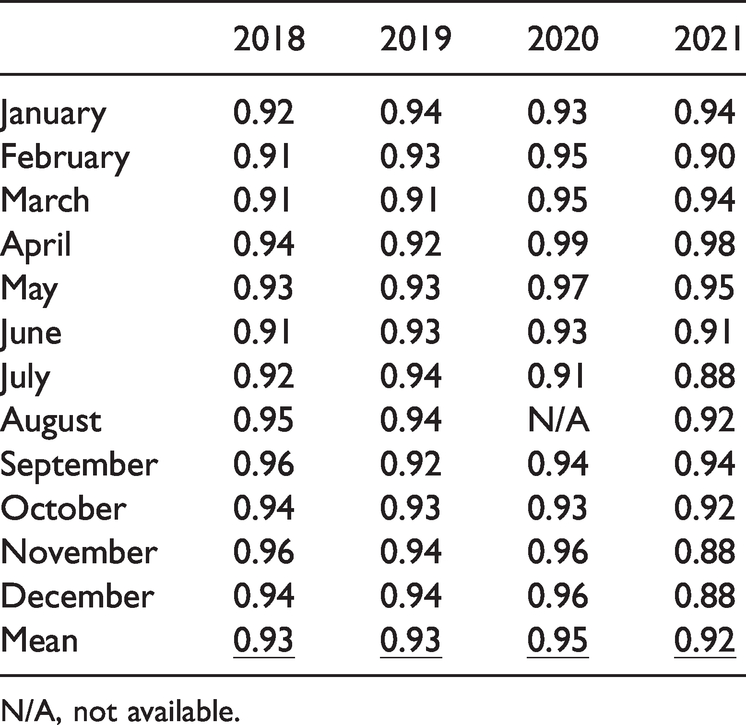
N/A, not available.
In the second phase of the study, the 14-month period before the onset of COVID-19 (pre-pandemic period) was compared with the 14-month pandemic period with a more detailed evaluation. The number of infants screened each month according to the Graf type is shown in Table 2. Patients with an abnormal Graf type in the two groups were thoroughly evaluated. In the pre-pandemic period, among eight infants who were classified as type IIc, a Pavlik bandage was applied to six patients and Tubingen orthosis was applied to two patients. On follow-up, a closed reduction procedure was performed in two patients whose hip findings did not improve. The findings of all other patients were found to improve on follow-up. During the pandemic, among five infants who were classified as type IIc, a Pavlik bandage was applied to three patients, and a Tubingen orthosis was applied to one patient. One patient missed the US follow-up and the orthopedic consultation. The remaining four infants demonstrated improvement following treatment.
Number of US screening results of DDH according to the Graf method in the pre-pandemic period (between January 2019 and February 2020) and during the pandemic (between April 2020 and June 2021).

*No examinations were performed in August 2020 owing to the absence of a radiologist. Therefore, this month was excluded.
DDH, developmental dysplasia of the hip; US, ultrasound.
In the pre-pandemic period, among four infants who were classified as type D, one patient improved with a Pavlik bandage and two underwent closed reduction who did not improve with bandages. Additionally, one of the four infants was ineligible for surgery owing to severe comorbidities. During the pandemic, among three infants who were classified as type D, one patient improved with a Pavlik bandage, and two underwent closed reduction who did not improve with bandages. In the pre-pandemic period, six infants were classified as type III and three were classified as type IV. Among these, one patient with type III improved with a Pavlik bandage, closed reduction was performed in three with type III (Figure 2), and open reduction was performed in two with type IV. Two infants with type III and one with type IV could not undergo surgery because of co-existing severe multisystem anomalies. However, none of the infants were classified as type III or IV disease during the pandemic. The rate of hip abnormalities during the pandemic period was significantly lower than that during the pre-pandemic period (p = 0.018, Table 3). Despite the decreased rate of abnormalities, there was a 1.5-fold increase in patients who missed follow-up or experienced a delay in receiving an initial US examination (p = 0.013).

A 70-day-old girl was admitted for hip ultrasound screening in November 2019. (A) Ultrasound image of the right hip showing a bony roof angle (α angle) of 42° and cartilage roof angle (β angle) of 79°, consistent with a type III hip. (B) Radiograph taken shortly before closed reduction at the age of 4 months (February 2020) showing a displaced right hip with an interrupted Shenton line (dashed lines). A continuous Shenton line can be seen on the normal side (curved line). Delayed ossification of the right femoral head can also be seen compared with an ossified epiphysis of the left hip (arrow). (C) Radiograph at the age of 12 months (October 2020) shows that the right hip has improved, but the ossified right femoral head is slightly smaller than the left femoral head and (D) Radiograph at the age of 23 months (September 2021) shows a recovered right hip that almost appears the same as the left hip.
Comparison of the 14-month pre-pandemic period and the 14-month pandemic period.

US, ultrasound; DDH, developmental dysplasia of the hip; SD, standard deviation.
*No examinations were performed in August 2020 owing to the absence of a radiologist. Therefore, this month was excluded.
We also evaluated the number of radiologists who performed US screening of DDH. In 2019, four radiologists worked from January to April, four worked in June and October, three worked in May, September, November, and December, two worked in August, and one worked in July. The decline in summer procedures was owing to annual leave taken in that period. In 2020, three radiologists worked from January to March, two worked from April to July, September, October, and December, one worked in November, and none worked in August. In 2021, two radiologists worked until the end of the pandemic. A total of 6107 (2937 women, 3170 men) US screening examinations of DDH were performed during the pre-pandemic period, and 3340 (1625 women, 1715 men) examinations were performed during the pandemic period (p = 0.007). However, no significant difference was found in the mean monthly US screening of DDH by each radiologist or the female-to-male ratio between the two periods.
Discussion
This study evaluated the effect of COVID-19 restrictions on US screening of DDH in a dedicated children’s hospital located in a city where 36,933 births were recorded in 2020. 18 This hospital attempted to adhere to the DDH US screening program throughout the restriction period, with a limited number of admissions and flexible working arrangement of operators. A 45.3% decline in the number of US examinations was observed at the children’s hospital in the 14-month pandemic period, and the lowest observed rate was in the first wave of COVID-19 (April and May 2020) in this period. The ratio of abnormal or immature hip joints was also reduced during the pandemic, indicating a potential of missed DDH cases during this time. This result may lead to a lapse in conservative treatment of cases and an increased requirement for surgical treatment in the future, with an additional burden placed on the health system.
Following the announcement of the first COVID-19 case, precautionary measures were gradually implemented in Turkey. On 16 March 2020, schools and universities switched to distance education and employees with chronic diseases or those older than 60 years were granted administrative leave. Lockdown rules were imposed for those older than 65 years and those younger than 20 years on 21 March and 3 April 2020, respectively. First, lockdown for all of the citizens in Diyarbakır was introduced on 10 April 2020, and continued throughout the weekend until 1 June 2020. Owing to the reduction in COVID-19 cases, the lockdown was halted and restrictions were softened during the summer. On 26 August 2020, flexible working arrangements and leave for disabled workers were reimplemented. On 13 January 2021, the vaccination program was started throughout the country. However, the second wave of COVID-19 continued to rise, and lockdown during weekends and travel restrictions were reimposed on 14 April 2021, while schools switched back to online education on 29 April 2021. Because of the reduction in cases and for socioeconomic reasons, the restrictions were softened on 1 June 2021, and completely repealed on 1 July 2021. 19 At that point, the government recommended self-isolation for all citizens, and partially supported a working from home arrangement.
According to the above-mentioned timeline, the pandemic period in our study was determined to be between 1 April 2020 and 1 July 2021. The number of US examinations for DDH markedly decreased at the beginning of the pandemic and gradually increased over time. A possible reason for this result could be the fear and anxiety experienced by parents during the first phase of the pandemic, which resolved over time. Although the number of examinations was remarkably reduced during the pandemic period, the number of examinations by each operator did not significantly change. This result suggests that the time interval for each screening examination was not significantly affected, and that the decrease in examinations during the pandemic was related to the flexible working time arrangement.
The female-to-male ratio of infants examined did not significantly change during the pandemic at our center. However, male infants were examined more frequently than female infants, even though girls have been found to be more affected by DDH than boys.9,15 This finding might be due to the traditional values of the region, which favor boys over girls.
Several studies have examined US screening of DDH in the COVID-19 era.15,16,20 In a study by Guindani et al, 16 US screening examinations decreased by 22% in 2020 (1083 examinations) compared with those in 2019 (1401 examinations). In the current study’s center, US screening decreased (by 45%) during the 14-month pandemic period compared with that in the pre-pandemic period. Although the hospital in the Italian study is located in a world-famous pandemic region (northern Italy), the US screening in the current study decreased by two fold. This discrepancy between studies might be due to the higher number of annual examinations in our center, where 5278 US screenings of DDH were performed in 2019 (3.5 times more than the Italian center). Doğan et al. 15 compared a 4-month period in 2019 and 2020 in their center. Interestingly, the number of US screenings of DDH increased in their study from 830 in 2019 to 935 in 2020. Hip US screening from April to May 2020 decreased by 63% compared with that observed in April to May 2019, but increased by 94% in June to July 2020. In the current study's center, the number of US screenings of DDH decreased by 71% in April to May 2020 and by 52% in April to July 2020 compared with that in the corresponding period in 2019. Similarly, according to Guindani et al., the number US screenings of DDH performed did not recover in June and July. 16
In the study by Guindani et al., the rate of delayed admission for US screening of DDH during the lockdown was 74%, 16 which is higher than that observed in the previous years. In addition, the rate of delayed US examinations increased by 5.5% compared with that observed in the previous year in another study. 15 In contrast, the lowest percentage of delayed US examinations in the current study was observed during the most severe period of the pandemic. The lowest delayed initial admission rate was observed in April 2020 (1%), followed by April 2021 (2%) and May 2020 (3%). One probable reason for this discrepancy between studies might be the routine clinical protocol established for US screening of DDH in the center of the current study. This protocol consists of neonatal screening performed after 2 weeks of life and before discharge of inpatient services. Because outpatient admissions decreased in the lockdown period, inpatient US screening became proportionally higher. Similarly, the latest guidelines recommend US screening to be performed at 4 weeks of age so that the treatment is performed as early as possible. 21
The ratio of abnormal or immature hip bone cases to the total number of screened infants was reduced during the pandemic period compared with that in the pre-pandemic period. Consanguineous marriages, genetic syndromes, and tight swaddling, which are risk factors for DDH, are more common in the rural areas than in the metropolitan areas of southeastern Turkey. Families living in these regions might have been more affected by the public travel restrictions of the pandemic regarding having US screening performed. However, this finding could also be due to the small sample of the pandemic period. Therefore, further multicenter studies at pediatric orthopedic clinics in the same area evaluating delayed or untreated cases are required to validate this speculation. No patient was diagnosed with type III or IV disease during the 14-month pandemic period, which is unexpected. During the period before the COVID-19 pandemic, nine type III or IV cases were classified through US screening. Furthermore, a 3.5-fold decrease in compliance with the follow-up examinations was observed in the follow-up recommendation during the pandemic period (348 in the pre-pandemic period and 93 in the pandemic period). According to Guindani et al., compliance with the recommended follow-up schedule was reduced from 70.1% to 35.9% during the pandemic period. 16 These findings clearly suggest that some DDH cases were missed during the pandemic period. Additionally, the progressed form of this disease will probably be treated in orthopedic clinics, leading to heavy physical and psychological burdens to patients in the future.
After the initial measures were implemented in Radiology Departments during the COVID-19 crisis, several guidelines and recommendation reports were published by radiology societies and hospitals worldwide.12,22,23 Similarly, several opinions regarding the application of US screening of DDH were provided. Hip US screening can be performed successfully up to the age of 6 months, as the femoral head and acetabulum have not yet ossified; the American Institute of Ultrasound in Medicine recommends US examination between ages 4 and 6 weeks.7 In Canada, Farrel et al. 13 recommended postponing pediatric US screening during the COVID-19 pandemic for at least 3 months and adjourning follow-up examinations after the end of the pandemic. However, new variants of severe acute respiratory syndrome coronavirus 2 have appeared, and the world’s population is still currently struggling with the COVID-19 crisis. Regarding the early treatment of DDH, reports from the International Hip Dysplasia Institute showed a 79% success rate with the use of the Pavlik harness in infants up to 6 months of age, as well as a 91% success rate of closed reduction in infants at a median of 8 months of age.24,25 Accordingly, even for dislocated hips, we observed better outcomes with the early diagnosis and treatment of DDH. Therefore, the continuation of US screening of DDH is recommended with a single accompanying parent allowed in the setting of community-based clinics at a considerable distance from COVID-19 clinics. 14 To prevent contamination and perform a safe US scan, the guidelines of the American Institute of Ultrasound in Medicine 26 or those of the World Federation of Ultrasound in Medicine and Biology 27 can be followed.
A major limitation of this study was the varied performance of the radiologists throughout the study. During annual leave and sick leave (including during the COVID-19 pandemic), radiologists were substituted temporarily from other hospitals or US appointments were postponed. Because US examinations of DDH and the Graf classification were highly operator-dependent, this might have reduced the credibility of the statistical results. Accordingly, some of the operators did not provide an information about the bony roof, shape of the bony rim, and coverage of the cartilaginous roof in their reports. The retrospective study design is another important limitation of this study, which led to an unstandardized initial examination and follow-up time. Additionally, we did not compare the exact timing of examinations between normal and pathological hips owing to archiving of age records, which may provide an idea regarding US screening referral by clinicians according to risk factors.
In conclusion, US screening of DDH is an indispensable method for the early diagnosis of DDH and has been well integrated into the health system in many countries. This study suggests that the downward trend observed in US screening rates during the COVID-19 pandemic could lead to missed or delayed cases of DDH. Therefore, there should be adherence to US screening of DDH as much as possible. Further studies evaluating the effect of the pandemic on DDH treatment may reveal more important results.
Footnotes
Acknowledgements
I am grateful to the families who took care of their infants by attending US screening for DDH, even during the pandemic.
Data availability statement
The data upon which this study is based are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The author declares that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sector.