
Abstract
Purpose
To describe three cases of mirror foot and to develop a new classification of the mirror feet with an emphasis on their treatment.
Methods
Surgical treatment was performed on three patients with mirror foot. Mirror feet in the English literature were surveyed and cases found in PubMed as well as our three cases were classified according to a new classification that was an analogy of the mirror hand classification proposed by Al-Qattan et al. (J Hand Surg Br 23:534–536, 1998).
Results
All three cases obtained satisfactory outcome after the treatment. In addition to these cases, 28 mirror feet were well described in the English literature, among which only seven cases have been documented for their treatment. All of the cases could be assigned to one of the categories of the proposed classification.
Conclusion
Mirror foot is a very rare congenital deformity of the foot. We successfully treated three novel cases of mirror feet. A classification of the mirror feet proposed in this article was useful in order to understand its nature and obtain a guideline for its treatment.
Introduction
Mirror image duplication of the foot (mirror foot) is a very rare congenital anomaly. As far as we know, 28 cases have been reported in the English literature [2–22], among which only seven cases have been documented for their treatment [2–7, 11]. Mirror foot may occur as an isolated deformity [8, 9] or as part of a syndrome of multiple congenital abnormalities; fibula dimelia [3, 5, 10–13], tibia hypoplasia [5, 7, 14], and nasal abnormalities such as Laurin–Sandrow syndrome [4, 6, 15–20] and Martin syndrome [21].
There was no strict definition of mirror foot. Some called mirror foot as a mirror-image polydactyly, but few cases among the reported cases showed a true mirror image. The number of toes in the reported cases varied from five to ten. Some had hallux, while others did not. Here, we report the outcome of surgical treatment of three cases with mirror foot and propose a classification of this condition.
Results
Case 1
A 4-month-old female was referred to our clinic. The right foot had eight toes, including hallux (the fourth toe from medial) (Fig. 1a), showing a mirror-image polydactyly. The baby was born after a full-term pregnancy. She was the first baby of healthy and non-consanguineous parents. Birth weight was 2,484 g. Family history was negative for congenital anomalies. Clinical examination showed that the trunk and upper limbs were normal. Right crus was bowing and was shorter than the left. Preaxial polydactyly was present in the left foot.
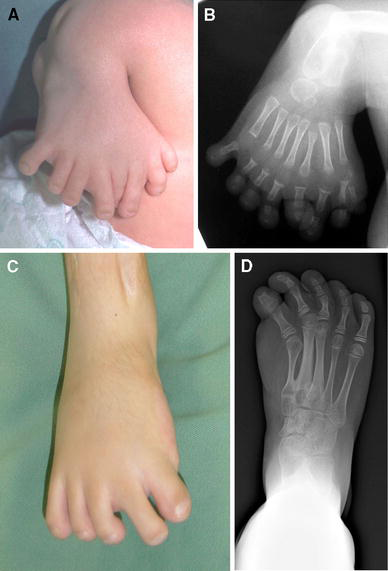
Case 1.
Radiographic examination showed there was complete absence of the right tibia, and the fibula was laterally displaced. The right foot had eight toes and seven metatarsals. The fourth toe consisted of two phalanges, while the others seemed to consist of three phalanges (Fig. 1b).
Preaxial three rays of the right foot were resected at the age of 1 year and 2 months. At the same time, the fibular was centralized to reconstruct the knee joint, and the ankle fusion was performed. Six months after the surgery, she acquired plantigrade foot and started to walk with a long leg brace. Since then, bone lengthening of the fibula and femur was performed as a separate operation, and now she can walk and run without the need for a brace. The appearance of the right foot has been satisfactorily improved (Fig. 1c, d).
Case 2
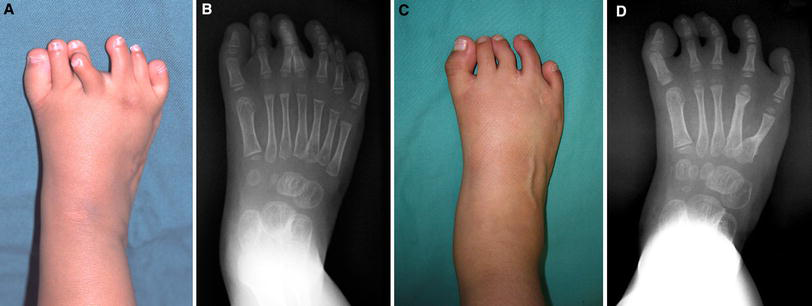
A 4-month-old female was seen for the assessment of a congenital anomaly of the right foot. The right foot had eight toes with a well-formed hallux (the fourth toe from medial) (Fig. 2a), showing mirror-image polydactyly. The baby was born at term after an uneventful pregnancy and delivery. She was the first baby of a 38-year-old father and 35-year-old mother, both healthy and non-consanguineous. Birth weight was 2,680 g. There was no family history of limb anomaly or congenital abnormalities. Examination revealed that she had clubfeet, and that her trunk and upper limbs were normal.

Case 2.
Radiographic examination showed that the right foot had eight toes and nine metatarsals. The fourth toe consisted of two phalanges, and the others seemed to consist of three phalanges. A set of cuneiforms seemed to be duplicated (Fig. 2b). The long bones of the arms and legs were normal.
Serial cast correction for the clubfeet was successfully completed, except equinus deformity. Operation was performed at the age of 11 months. Preaxial three toes and four metatarsals were ablated and two cuneiforms were resected and excess cartilage of the remaining cuneiforms and the navicular was shaved. The flexor and extensor tendons of the hallux were hypoplastic. The dorsal capsule of the metatarsophalangeal joint of the hallux was released to correct hyperextension deformity of the joint. At the same time, subcutaneous tenotomy of the Achilles tendon was performed to correct equinus deformity of the foot. The foot became plantigrade and she could wear normal shoes. Night splint was used in order to maintain correction of the clubfoot. Although the big toe remained short, the appearance of the right foot was much improved postoperatively (Fig. 2c, d).
Case 3
A 1-month-old female baby was referred to our clinic. The right foot had seven toes, including hallux (Fig. 3a). The third and the fourth toes were crossing. Hallux was present at the most medial side. She was born at term after an uneventful pregnancy and delivery. Her parents were healthy and non-consanguineous. Birth weight was 2,962 g. There was no family history of limb anomaly or congenital abnormalities. Clinical examination revealed that the trunk, the upper limbs, and the left lower limb were normal. She had a clubfoot on the right side.
Case 3.
Radiographic examination showed that the right foot had seven toes and seven metatarsals. The most medial toe had two phalanges, while the others had three phalanges. The calcaneus and the cuboid were duplicated (Fig 3b). The long bones of the arms and legs were normal, except for the presence of an incomplete fibula dimelia in the right lower limb.
Z-lengthening of the right Achilles tendon was done when she was 1 year and 2 months old in order to correct the equinus deformity. The Achilles tendon bifurcated distally and inset into both calcanei. The operation for polydactyly was performed at the age of 2 years and 1 month. The fourth and sixth toes were resected, because they were hypoplastic and deformed. The fifth and seventh rays were respectively transferred to the fourth and fifth rays to improve the appearance of the foot. Nine years after the operation, the appearance of the right foot is satisfactory (Fig. 3c, d). She can run and wear normal shoes with no pain.
Discussion
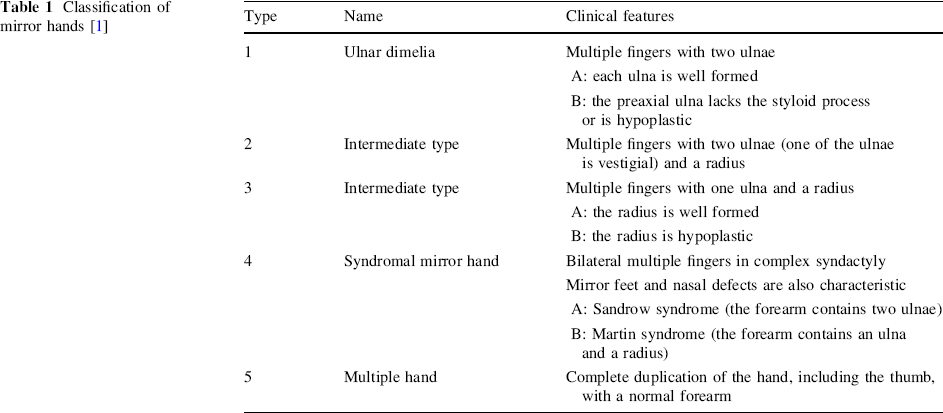
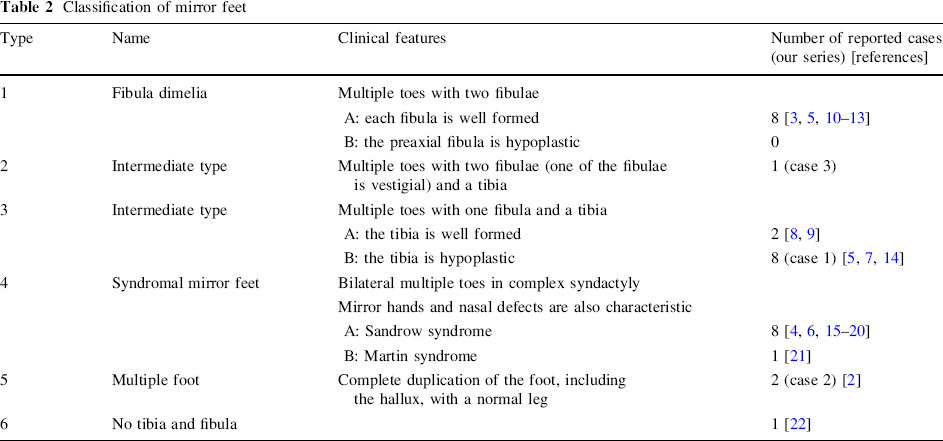
Corresponding to a mirror foot, mirror-image duplication of the hand is known as a mirror hand. Al-Qattan et al. [1] classified mirror hands into five types, mainly according to the condition of the ulna and the radius (Table 1). Most cases of mirror hand were classified into type 1A and type 1B, which were associated with ulnar dimelia. Type 1A ulnar dimelia was much less common than type 1B. The remaining types of mirror hand were very rare; one case of type 2, two cases of type 3A, one case of type 3B, one case of type 4A, three cases of type 4B, and six cases of type 5 have been reported. From the embryologic point of view, the ulna corresponds to the fibula, while the radius corresponds to the tibia [23]. Therefore, referring to the above classification, we classified the reported and our series of mirror foot with the classification of mirror hand by changing ulna into fibula and radius into tibia (Table 2). There were eight cases of type 1A, no case of type 1B, one case of type 2 (case 3 in our series), two cases of type 3A, eight cases of type 3B (including case 1 in our series), eight cases of type 4A, one case of type 4B, and two cases of type 5 (including case 2 in our series). A new category was created for one case as type 6, where the mesomelic bones were missing. Using this classification, three differences between mirror hand and mirror foot could be pointed out. Firstly, mirror foot had no case of type 1B, which consisted of the majority of mirror hands. Although ulnar dimelia was associated with most cases of mirror hand, fibula dimelia was present in less than half of the cases of mirror foot. In other cases of mirror foot, there was a normal or hypoplastic tibia [21] or the mesomelic bones were missing [22]. Secondly, type 3B was most frequent in mirror foot. Thirdly, mirror foot was more evenly distributed among the classification than mirror hand. In addition, mirror hands typically had seven or eight digits and no thumb, while mirror feet were more variable, ranging from five to ten toes [17]. Some of the mirror feet had central hallux with or without bony fusion, and others had no obvious hallux [13, 21].
Classification of mirror hands [1]
Classification of mirror feet
In our three cases, the numbers of toes were seven or eight. Hallux was present in all feet. In case 3, the foot had seven toes, associated with fibular dimelia and duplication of the tarsal bones. We considered that it was a mirror foot, although hallux was at the most medial side, because the computed tomography image clearly showed mirror symmetry on the dorso-plantar plane (Fig. 4), although this foot did not form mirror symmetry on the tibio-fibular (antero-posterior) plane.

Computed tomography image of the right foot of case 3, demonstrating a possible duplication on the dorso-plantar plane
In cases of mirror hand, in which most cases had no thumb, the functional reconstruction of the thumb, such as pollicization, is more important than the cosmetic reconstruction. The treatment of mirror foot was not well described in the literature. Simple ablation of the supernumerary rays was performed in five cases [2, 4–7]. Two feet were disarticulated [3, 11]. In our series of mirror foot, in which there was hallux, the supernumerary preaxial lays of feet were resected, or lay transfer was performed to improve function and appearance. In types 1 and 3B, the tibia is missing and there presents severe flexion contracture of the knee and equinus deformity of the ankle. Because these deformities are very difficult to correct, disarticulation of the knee will be a reasonable treatment of choice. In types 2, 3A, and 5, the tibia is well formed. Ablation of the supernumerary rays will be indicated. In these circumstances, one should pay attention to hypoplasty of the rays and consider the best combination of rays that will be left. In types 4 and 6, the deformities of the feet are severe and complicated with severe syndactyly. Also, the patients usually have multiple anomalies. The treatment must be tailored individually.